Treatment of strep throat ulcer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"streptococcal pharyngitis" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching the Web
strep throat pharyngeal ulcer treatment antibiotics 2024 guidelines
I now have comprehensive information to give a complete, well-cited answer. Here is the full treatment guide for strep throat (Group A Streptococcal pharyngitis), including its ulcerative/exudative presentation:
Treatment of Strep Throat (Group A Streptococcal Pharyngitis)
What is "Strep Throat Ulcer"?
Strep throat caused by Streptococcus pyogenes (Group A Streptococcus / GAS) typically presents with pharyngeal erythema, tonsillar exudate, and cervical lymphadenopathy. The "ulcerative" appearance refers to the inflamed, eroded tonsillar/pharyngeal mucosa seen in severe cases. True pharyngeal ulcers with strep should also prompt consideration of other causes (herpes simplex, mononucleosis, agranulocytosis, Behçet's, HIV, or gonococcal pharyngitis).
1. Symptomatic / Supportive Treatment (all patients)
For all pharyngitis — streptococcal and non-streptococcal — regardless of antibiotic use:
- Analgesics/antipyretics: Acetaminophen or NSAIDs (ibuprofen) — primary pain relief
- Saline gargles
- Humidification
- Soft foods
- Tea with honey
- Adequate hydration
Note on glucocorticoids: A single dose of dexamethasone 10 mg may reduce pain within 24 hours but does not decrease absenteeism or relapse rates, and even short courses carry risks of sepsis, GI bleeding, VTE, and fracture within 30 days — not routinely recommended. — Harrison's Principles of Internal Medicine, 22nd Ed., p. 302
2. Antibiotic Treatment
GAS is the only common cause of pharyngitis requiring antibiotics. Goals: symptom reduction, prevent spread, prevent suppurative complications (peritonsillar abscess), and prevent acute rheumatic fever.
Penicillin is the antibiotic of choice — no GAS isolate has ever been resistant to it. — Harrison's, p. 302; Red Book 2021
Duration: 7–10 days (unlike many other infections, shorter courses are less effective for GAS pharyngitis).
Table: Antibiotic Treatment of GAS Pharyngitis
| Category | Antibiotic | Adult Dose | Duration |
|---|---|---|---|
| Drug of choice | Penicillin V | 500 mg PO QID or 1000 mg PO BID | 10 days |
| Alternative (non-penicillin allergic) | Amoxicillin | 500 mg PO BID or 1000 mg PO QD | 10 days |
| Mild penicillin allergy | Cephalexin | 500 mg PO BID | 10 days |
| Cefadroxil | 1 g PO QD | 10 days | |
| Severe penicillin allergy | Erythromycin | 250–500 mg PO QID or 500–1000 mg PO BID | 5 days |
| Clarithromycin | 500 mg PO BID | 5 days | |
| Clindamycin | 300 mg PO TID | 10 days |
Harrison's Principles of Internal Medicine 22E, Table 37-5, p. 302
Amoxicillin is preferred in children (palatable liquid form; equally effective as penicillin). — Red Book 2021
Benzathine penicillin G IM (single dose) is an option when oral compliance is a concern.
3. Diagnostic Approach Before Treating
- Use Centor/McIsaac criteria (tonsillar exudate, tender anterior cervical lymphadenopathy, fever, absence of cough)
- Confirm with Rapid Antigen Detection Test (RADT) — do not treat empirically in adults without testing (GAS carriage rates ~5% in adults can cause false-positive reasoning)
- Throat culture if RADT negative but clinical suspicion is high
4. When Pharyngeal Ulcers Suggest a Different Diagnosis
If ulcers are present and strep testing is negative or the patient fails to respond to penicillin, consider:
| Finding | Alternative Diagnosis |
|---|---|
| Posterior cervical adenopathy, splenomegaly, palatal petechiae | Infectious mononucleosis (EBV) — avoid amoxicillin (causes rash) |
| Unresponsive to penicillin + risk factors (MSM, fellatio) | Gonococcal pharyngitis (N. gonorrhoeae) |
| Grayish pseudomembrane | Diphtheria (C. diphtheriae) |
| New sexual partner, fever, rash, myalgias | Acute HIV |
| Rigors, neck swelling, not resolving | Lemierre syndrome (Fusobacterium necrophorum) |
| White plaques that scrape off, bleeding surface | Oral candidiasis |
— Harrison's Principles of Internal Medicine 22E, Table 37-3, p. 301
5. When to Seek Urgent Care
Symptoms requiring immediate re-evaluation:
- Shaking chills (rigors)
- Neck swelling beyond lymphadenopathy
- Difficulty swallowing or drooling
- Symptoms persisting >5 days without improvement
These may signal peritonsillar abscess, deep neck space infection, or Lemierre syndrome.
6. Post-Treatment
- Pharyngitis should resolve within 3–5 days with appropriate treatment
- No routine "test of cure" needed unless symptoms recur or complications develop
- Household contacts with symptoms should also be tested
Recent evidence (2023–2025): A 2025 Lancet Infectious Diseases umbrella review (PMID: 39243792) confirmed that GAS pharyngitis specifically requires the full 10-day course — unlike most other respiratory infections where shorter courses are now preferred.
Cefpodoxime for pharyngitis
Finding Sources
Finding Sources
Searching the Web
cefpodoxime pharyngitis strep throat dose duration FDA approved
Reading File
Searching PubMed
cefpodoxime pharyngitis streptococcal
I have all the information needed for a comprehensive answer.
Cefpodoxime for Pharyngitis (GAS / Strep Throat)
Drug Overview
Cefpodoxime proxetil (brand: Vantin) is a third-generation oral cephalosporin (prodrug — deesterified in the GI tract to active cefpodoxime). It is one of only three oral antibiotics FDA-approved for a 5-day course of Group A Streptococcal (GAS) pharyngitis/tonsillitis — the others being cefdinir and azithromycin.
Place in Therapy
Cefpodoxime is used as an alternative to penicillin — specifically for patients with:
- Non-anaphylactic (mild) penicillin allergy — cephalosporins are safe (cross-reactivity <2%)
- Poor compliance with 10-day regimens — the shorter 5-day course improves adherence
- Recurrent GAS pharyngitis — broader β-lactamase coverage may help
"FDA has approved three oral antibiotics for 5-day strep throat treatment in both children and adults: cefdinir, cefpodoxime, and azithromycin." — Harriet Lane Handbook, 23rd Ed.
A meta-analysis of 22 trials (n = 7,470) found 5-day cefpodoxime achieved 90% bacterial cure vs. 70% for 10-day penicillin (OR 1.47) — though this does not change its second-line status given penicillin's proven rheumatic fever prevention record.
Dosing
Adults & Adolescents (≥12 years)
| Parameter | Detail |
|---|---|
| Dose | 100 mg PO every 12 hours |
| Total daily dose | 200 mg/day |
| Duration | 5–10 days (5 days is FDA-approved and preferred) |
| Administration | With food (enhances absorption) |
Pediatrics (2 months – 12 years)
| Parameter | Detail |
|---|---|
| Dose | 5 mg/kg/dose PO every 12 hours |
| Max per dose | 100 mg |
| Total daily max | 200 mg/day |
| Duration | 5–10 days |
| Oral suspension | May be given without regard to food |
— Harriet Lane Handbook, 23rd Ed.; FDA prescribing information (Vantin)
Pharmacology
- Mechanism: Inhibits bacterial cell wall synthesis (binds penicillin-binding proteins)
- Spectrum: Active against S. pyogenes (GAS), S. pneumoniae (penicillin-susceptible strains), S. aureus (MSSA), H. influenzae, M. catarrhalis, E. coli, K. pneumoniae, P. mirabilis
- Bioavailability: Enhanced with food; ~50% absorbed as active drug
Key Drug Interactions & Precautions
| Issue | Detail |
|---|---|
| Antacids / H₂ blockers (high dose) | Reduce cefpodoxime absorption — avoid co-administration |
| Probenecid | Increases serum cefpodoxime levels |
| Renal impairment | CrCl ≤29 mL/min → extend dosing interval to every 24 hours |
| Penicillin allergy | Use caution; avoid in anaphylaxis/severe allergy history |
| False-positive | Urine-reducing substance tests (Clinitest, Benedict's, Fehling's); Coombs test — use enzymatic glucose tests (Clinistix) instead |
Common Adverse Effects
- Diarrhea, nausea, vomiting (GI most common)
- Vaginal candidiasis
- Transient ALT/AST elevation
- Headache, rash
Important Limitations
- Does not prevent rheumatic fever with certainty — insufficient data for post-strep prophylaxis
- Not effective for penicillin-resistant S. pneumoniae (unfavorable pharmacodynamic parameters)
- Not recommended for severe penicillin allergy (IgE-mediated/anaphylaxis) — use clindamycin or clarithromycin instead
- IDSA still recommends penicillin/amoxicillin as first-line — cefpodoxime is an alternative
Quick Comparison: Cefpodoxime vs. Standard Agents
| Drug | Duration | Position | Notes |
|---|---|---|---|
| Penicillin V | 10 days | First-line | Narrowest spectrum, no resistance |
| Amoxicillin | 10 days | First-line (esp. children) | Palatable liquid form |
| Cefpodoxime | 5–10 days | Alternative | FDA-approved 5-day course; better compliance |
| Cefdinir | 5–10 days | Alternative | Similar to cefpodoxime |
| Clindamycin | 10 days | Severe PCN allergy | |
| Azithromycin | 5 days | Severe PCN allergy | Higher GAS resistance rates (~10%) |
How to treat step throat ulcer
This was covered in detail in our first response above. Here's a focused summary:
Treatment of Strep Throat Ulcer (GAS Pharyngitis)
The ulcerative/exudative appearance in strep throat is caused by Streptococcus pyogenes (Group A Strep) inflaming and eroding the tonsillar/pharyngeal mucosa. Treatment targets both the infection and the symptoms.
1. Antibiotics (Treat the Infection)
First-line:
| Drug | Dose | Duration |
|---|---|---|
| Penicillin V | 500 mg PO BID or QID | 10 days |
| Amoxicillin | 500 mg PO BID or 1g PO OD | 10 days |
Penicillin allergy — mild (non-anaphylactic):
| Drug | Dose | Duration |
|---|---|---|
| Cephalexin | 500 mg PO BID | 10 days |
| Cefadroxil | 1 g PO OD | 10 days |
| Cefpodoxime | 100 mg PO BID | 5–10 days (FDA-approved 5-day) |
Penicillin allergy — severe (anaphylactic):
| Drug | Dose | Duration |
|---|---|---|
| Clindamycin | 300 mg PO TID | 10 days |
| Clarithromycin | 500 mg PO BID | 5 days |
| Erythromycin | 500 mg PO BID | 5 days |
Harrison's Principles of Internal Medicine 22E, Table 37-5
2. Symptomatic Relief (Soothe the Ulcer/Throat)
| Measure | Purpose |
|---|---|
| Ibuprofen or Paracetamol | Pain and fever relief |
| Saline gargles (warm, ½ tsp salt/glass water) | Reduce local inflammation, soothe ulcers |
| Honey + warm tea | Soothing, mild antimicrobial effect |
| Soft/cold foods | Minimize trauma to ulcerated mucosa |
| Adequate hydration | Prevents dehydration from dysphagia |
| Humidification | Reduces throat dryness |
3. What NOT to Do
- No antibiotics without a positive rapid strep test (RADT) or throat culture — most sore throats are viral
- No glucocorticoids routinely — short steroid courses carry risk of sepsis, GI bleed, VTE within 30 days
- No amoxicillin if mononucleosis (EBV) is suspected — causes a widespread rash
4. Red Flags — Seek Urgent Care If:
- Difficulty swallowing or drooling (possible peritonsillar abscess)
- Neck swelling beyond lymph nodes
- Rigors (shaking chills)
- Symptoms not improving after 5 days on antibiotics
- Muffled "hot potato" voice
These suggest peritonsillar abscess, deep neck space infection, or Lemierre syndrome — all requiring urgent ENT/ED evaluation and possible drainage.
Expected Course
With appropriate antibiotics, symptoms resolve in 3–5 days. The ulcerated mucosa heals fully once the infection clears. Full 10-day antibiotic completion is essential to prevent acute rheumatic fever.
Viral pharyngitis with white spots
Finding Sources
Finding Sources
Searching Images
viral pharyngitis white spots tonsils exudate
Finding Sources
Finding Sources
Searching the Web
viral pharyngitis white spots tonsils causes differential diagnosis treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Now I have everything needed for a comprehensive, image-supported answer.
Viral Pharyngitis with White Spots
Key Point First
White spots/exudate on the throat do NOT automatically mean bacterial infection. Several viral conditions produce white patches, vesicles, or exudate — and antibiotics are not indicated for any of them. The clinical challenge is distinguishing these from bacterial (GAS) pharyngitis.
Causes of White Spots in Viral Pharyngitis
1. Infectious Mononucleosis (EBV) — Most Common Viral Cause of White Exudate
Classic triad: Fever + pharyngitis + marked lymphadenopathy
White spots: Creamy/grey-white tonsillar exudate, often confluent and extensive — can look identical to strep
Key distinguishing features:
- Posterior cervical or auricular lymphadenopathy (highly specific)
- Splenomegaly
- Palatal petechiae
- Gelatinous/swollen uvula
- Age: young adults (15–35)
- Fatigue out of proportion to throat findings
Diagnosis: Monospot (heterophile antibody) — positive in 40–60% at week 1, 80–90% by week 3. WBC: 10,000–20,000/μL with marked lymphocytosis and >10% atypical lymphocytes.
— Harrison's Principles of Internal Medicine 22E, p. 302; Cummings Otolaryngology
2. Herpangina (Coxsackievirus A / Enteroviruses)
Causative agents: Coxsackievirus A (especially A8, A10, A16), echoviruses, enterovirus 71
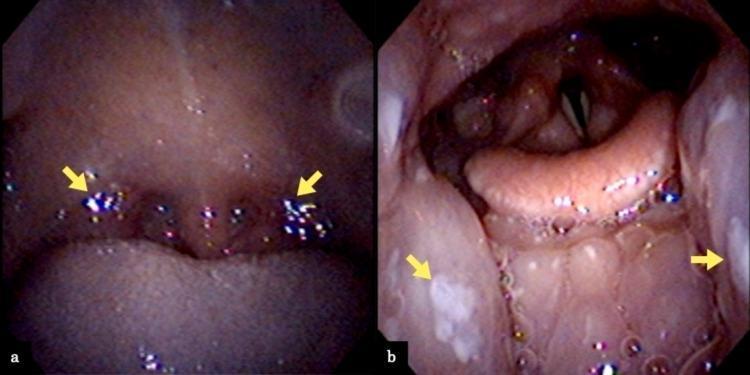
White spots: 2–4 mm yellowish-white vesicles/ulcers on soft palate, anterior faucial pillars, uvula, tonsils — each surrounded by an intense red halo (areola). Vesicles ulcerate to leave shallow, punched-out grayish-yellow craters.
Key distinguishing features:
- Affects children primarily
- Abrupt fever, headache, dysphagia
- Lesions confined to the posterior oropharynx (vs. herpes which involves anterior mouth/gingiva)
- Lesions disappear in 5–10 days spontaneously

Coxsackievirus A10 variant: Causes acute lymphonodular pharyngitis — discrete yellow-white papules (not vesicles) in the same distribution.
— Andrews' Diseases of the Skin, p. 456
3. Primary HSV Pharyngitis (Herpes Simplex Virus)
White spots: Vesicles that rupture into ulcers with grey-white base, can involve soft palate, uvula, tonsillar pillars. Associated with gingivostomatitis (anterior mouth involvement distinguishes from herpangina).
Key features:
- Fever, severe odynophagia
- Anterior oral ulcers often also present (lips, gingiva, buccal mucosa)
- Young adults, immunocompromised patients
4. Hand-Foot-and-Mouth Disease (HFMD — Coxsackievirus A16/EV71)
White spots: 4–8 mm rapidly ulcerating vesicles on buccal mucosa, tongue, soft palate
Key distinguishing feature: Concurrent vesicles on palms, soles, and buttocks (pathognomonic)
— Andrews' Diseases of the Skin, p. 456
Differentiating Viral from Bacterial White Spots
| Feature | Viral (EBV/Herpangina/HSV) | Bacterial (GAS Strep) |
|---|---|---|
| Cough/rhinorrhea/hoarseness | Often present | Absent |
| Posterior cervical nodes | EBV — prominent | Anterior cervical |
| Splenomegaly | EBV — yes | No |
| Exudate character | May be confluent (EBV) / vesicular (herpangina) | Patchy white-yellow plaques |
| Palatal petechiae | EBV | GAS (both possible) |
| Oral ulcers | Common in viral | Uncommon |
| Rash | HFMD (hands/feet/buttocks) | Scarlatiniform (GAS) |
| Rapid strep test | Negative | Positive |
Oral ulcers are a feature that actually favors viral etiology and argues against strep. — Cummings Otolaryngology, p. 3796
Treatment
Viral pharyngitis with white spots — NO antibiotics needed
| Measure | Details |
|---|---|
| Rest | Essential |
| Analgesics/antipyretics | Ibuprofen or paracetamol — primary pain/fever control |
| Hydration | Critical, especially if dysphagia limits intake |
| Saline gargles | Soothe inflamed/ulcerated mucosa |
| Topical anesthetics | Benzocaine/lidocaine gargles or lozenges — helpful for herpangina ulcer pain |
| Soft, cold foods | Ice cream, yoghurt, cold liquids reduce pain |
| Honey + warm liquids | Soothing effect |
EBV-specific cautions:
- Avoid amoxicillin/ampicillin — causes a widespread maculopapular rash in ~80–100% of mono patients
- Avoid contact sports for 3–4 weeks — spleen rupture risk
- Corticosteroids (prednisolone) only if severe airway compromise, thrombocytopenia, or hemolytic anemia
HSV-specific:
- Aciclovir (oral) may shorten duration if started within 72 hours — evidence limited for pharyngeal HSV specifically
- Immunocompromised patients: IV aciclovir
Herpangina / HFMD:
- Strictly supportive — no antiviral treatment established
- Ensure adequate fluid intake (hospitalise if unable to drink in children)
When to Test for GAS Despite Suspected Viral Cause
Even with viral features, test with rapid strep test if:
- Centor score ≥ 2–3 (fever, tonsillar exudate, tender anterior nodes, no cough)
- Immunocompromised patient
- Close contact with confirmed strep case
- Worsening after 3–5 days
If RADT is negative and mono features are present → monospot test. If monospot negative in first week with high suspicion → EBV-specific antibodies (VCA IgM).
Saline gargle vs betadine gargle
Finding Sources
Finding Sources
Searching PubMed
saline gargle "povidone iodine" pharyngitis sore throat
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.