Why is subdural hemorrhage more common in elderly
Reading File
Finding Sources
Searching PubMed
subdural hematoma elderly brain atrophy bridging veins
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a thorough answer drawing from multiple authoritative medical textbooks:
Why Subdural Hemorrhage is More Common in the Elderly
Subdural hematoma (SDH) preferentially affects older adults due to several converging anatomical, physiological, and pharmacological factors:
1. Brain Atrophy - The Central Mechanism
As the brain ages, it undergoes progressive atrophy - it physically shrinks within the cranial vault. This is the most important factor. Here's how it leads to SDH:
- The bridging veins run from the cerebral cortex, through the subarachnoid space, and drain into the dural venous sinuses. They must traverse the subdural space to get there.
- Normally, the brain fills the skull snugly, keeping the bridging veins short and under minimal tension.
- With brain atrophy, the brain recedes from the dura. The bridging veins must now span a longer distance to reach the sinuses, which stretches them and puts them under chronic tension.
- Even trivial acceleration-deceleration forces - such as a minor fall or whiplash - are enough to tear these already-taut, stretched veins.
- In a young brain, the same force would not produce enough displacement to tear them.
"In older individuals with brain atrophy, the bridging veins are stretched, hence the increasing incidence of subdural hematoma with aging." - Robbins & Cotran Pathologic Basis of Disease
"Atrophy allows the brain to move more freely within the cranial vault, thus making the bridging veins more susceptible to shear injury... this type of hematoma may be seen with minimal or no known history of trauma." - Neuroanatomy through Clinical Cases, 3rd Edition
2. Greater Brain Mobility
A corollary of atrophy: the atrophied brain has more room to move inside the skull during acceleration-deceleration. Greater movement means greater shear force on the bridging veins, further compounding the risk.
3. Larger Subdural Space - More Room for Expansion
Brain atrophy also creates a larger potential subdural space. This allows blood to accumulate gradually without producing dramatic symptoms (the "chronic" pattern). The brain can accommodate the slow bleed over weeks to months, which is why elderly patients often present late with vague symptoms like:
- Cognitive decline or confusion
- Headache
- Unsteady gait
- Focal neurological deficits
This delayed presentation is particularly characteristic of chronic subdural hematoma in the elderly.
4. Anticoagulant and Antiplatelet Use
Elderly patients disproportionately take blood thinners, which dramatically amplify bleeding risk:
- Warfarin, direct-acting oral anticoagulants (DOACs) like rivaroxaban or apixaban
- Antiplatelet agents such as aspirin or clopidogrel
"Risk factors for subdural hematomas are frequent falls, alcoholic dependence, and use of anticoagulant medications such as warfarin, direct-acting anticoagulants, or aspirin." - Symptom to Diagnosis, 4th Edition
"Direct cranial trauma may be minor and is not always required... especially in the elderly and those taking anticoagulant medications." - Harrison's Principles of Internal Medicine, 22E
5. Frequent Falls
Falls are far more common in the elderly due to gait instability, balance disorders, orthostatic hypotension, and polypharmacy. Even falls from a standing height - which would rarely injure a young person - generate enough acceleration-deceleration to tear stretched bridging veins.
6. Additional Risk Factor: Chronic Alcoholism
Heavy alcohol use causes brain atrophy independently of age and also impairs coagulation. This is why chronic alcoholics of any age share a similar risk profile to elderly patients.
Gross Pathology
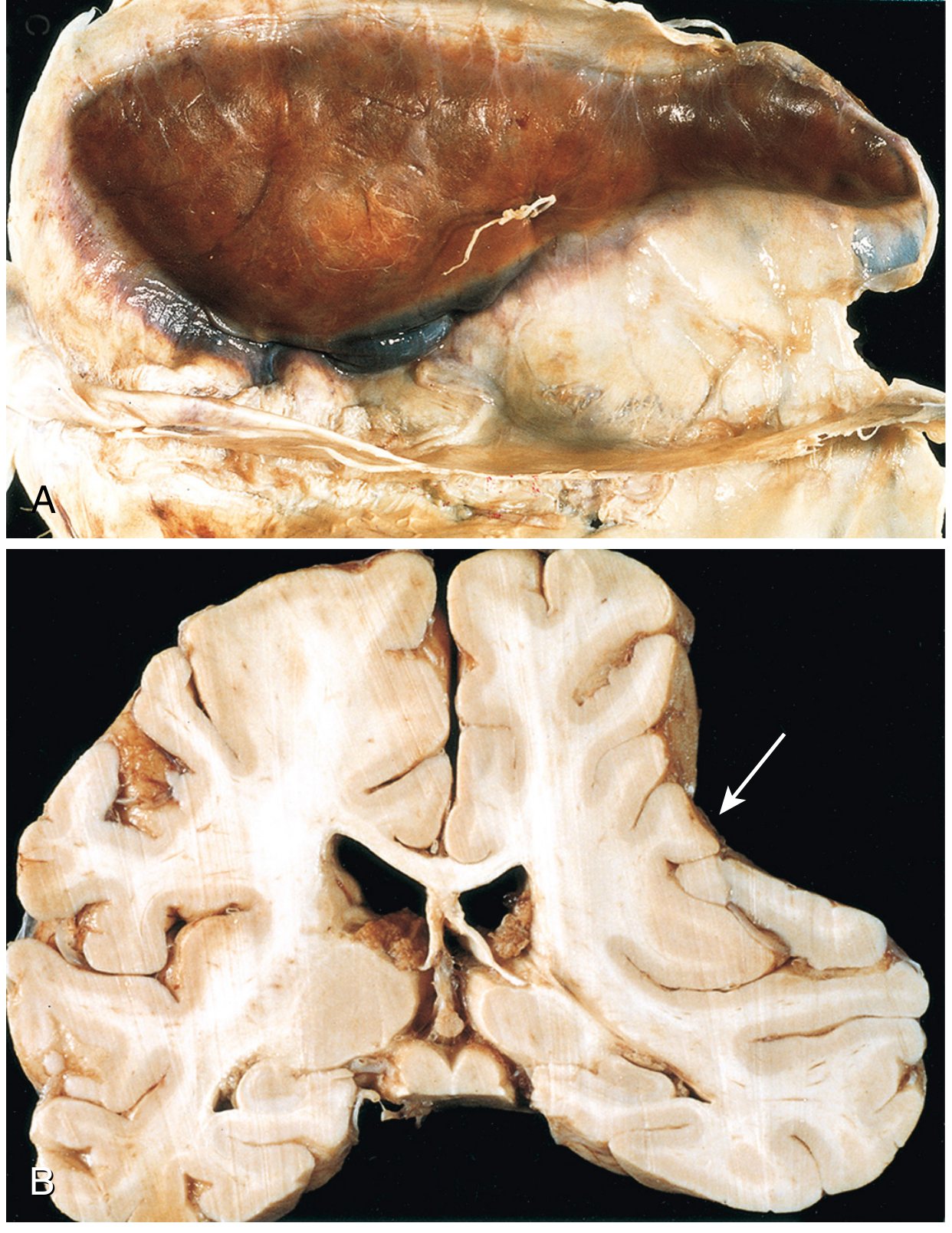
Fig. 28.21 - Subdural hematoma (A) Large organizing SDH attached to the dura (B) Coronal section showing atrophy of the compressed hemisphere. - Robbins & Cotran Pathologic Basis of Disease
Summary Table
| Factor | Mechanism |
|---|---|
| Brain atrophy | Stretches bridging veins over a longer distance, making them prone to tearing |
| Greater brain mobility | More movement inside the skull = more shear on bridging veins |
| Enlarged subdural space | Allows slow blood accumulation without early symptoms (chronic SDH) |
| Anticoagulant/antiplatelet use | Impairs clotting; minor venous bleed becomes a significant hematoma |
| Frequent falls | More opportunities for the triggering trauma |
| Thin-walled veins | Vascular aging reduces vessel wall integrity |
The mean age at diagnosis for subdural hematoma is around 70 years in most studies, and in up to 50% of chronic cases, no obvious antecedent trauma is identified - a direct consequence of how trivial the inciting event can be in the elderly brain.
- Robbins, Cotran & Kumar: Pathologic Basis of Disease, p. 1162
- Harrison's Principles of Internal Medicine, 22E
- Neuroanatomy through Clinical Cases, 3rd Ed., p. 174
- Tintinalli's Emergency Medicine, p. 1733
- Symptom to Diagnosis: An Evidence Based Guide, 4th Ed., p. 380
This is a shared conversation. Sign in to Orris to start your own chat.