Retinal detachment details with pictures fundus
Reading File
Finding Sources
Searching Images
retinal detachment fundus photograph
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from Kanski's Clinical Ophthalmology. Let me compile the full answer with all the fundus images.
Retinal Detachment — Comprehensive Overview
Sources: Kanski's Clinical Ophthalmology (10th ed.), Harrison's Principles of Internal Medicine (21st ed.), Robbins & Kumar Pathology
Definition
Retinal detachment (RD) is the separation of the neurosensory retina from the retinal pigment epithelium (RPE), with accumulation of fluid (subretinal fluid, SRF) in the potential subretinal space. There are three distinct types based on mechanism.
Types of Retinal Detachment
| Type | Mechanism | Key Feature |
|---|---|---|
| Rhegmatogenous | Retinal break + liquefied vitreous | Most common; convex, corrugated |
| Tractional | Fibrovascular membrane contraction | Concave; no breaks; no shifting fluid |
| Exudative/Serous | Fluid leaks from vessels without break | Smooth convex; "shifting fluid" |
1. Rhegmatogenous Retinal Detachment (RRD)
Epidemiology & Pathogenesis
- Affects ~1 in 10,000 per year; both eyes in ~10% of cases
- Requires both a retinal break and at least partial vitreous liquefaction with traction
- Over 40% occur in myopic eyes — the higher the refractive error, the greater the risk
- Predisposing lesions: lattice degeneration, snailtrack degeneration, posterior vitreous detachment (PVD)
- Risk factors: cataract surgery (especially with vitreous loss), laser capsulotomy
Location of Breaks
- ~60% superotemporal quadrant
- ~15% superonasal
- ~15% inferotemporal
- ~10% inferonasal
- ~50% of eyes have more than one break
Symptoms (Classic Triad)
- Photopsia (flashing lights) — from vitreous traction on the retina
- Floaters — pigment cells or blood in vitreous
- Curtain/shadow — peripheral visual field defect progressing toward center
The visual field defect is in the opposite quadrant to the primary retinal break. Patients sometimes notice it disappears on waking (overnight absorption of SRF) only to return during the day.
Signs
- Relative afferent pupillary defect (RAPD) — in extensive RD
- Low IOP (~5 mmHg less than fellow eye)
- "Tobacco dust" (Shafer's sign) — pigment cells in anterior vitreous = pathognomonic
- Retinal breaks appear as red discontinuities against the choroidal background
Fundus Photographs
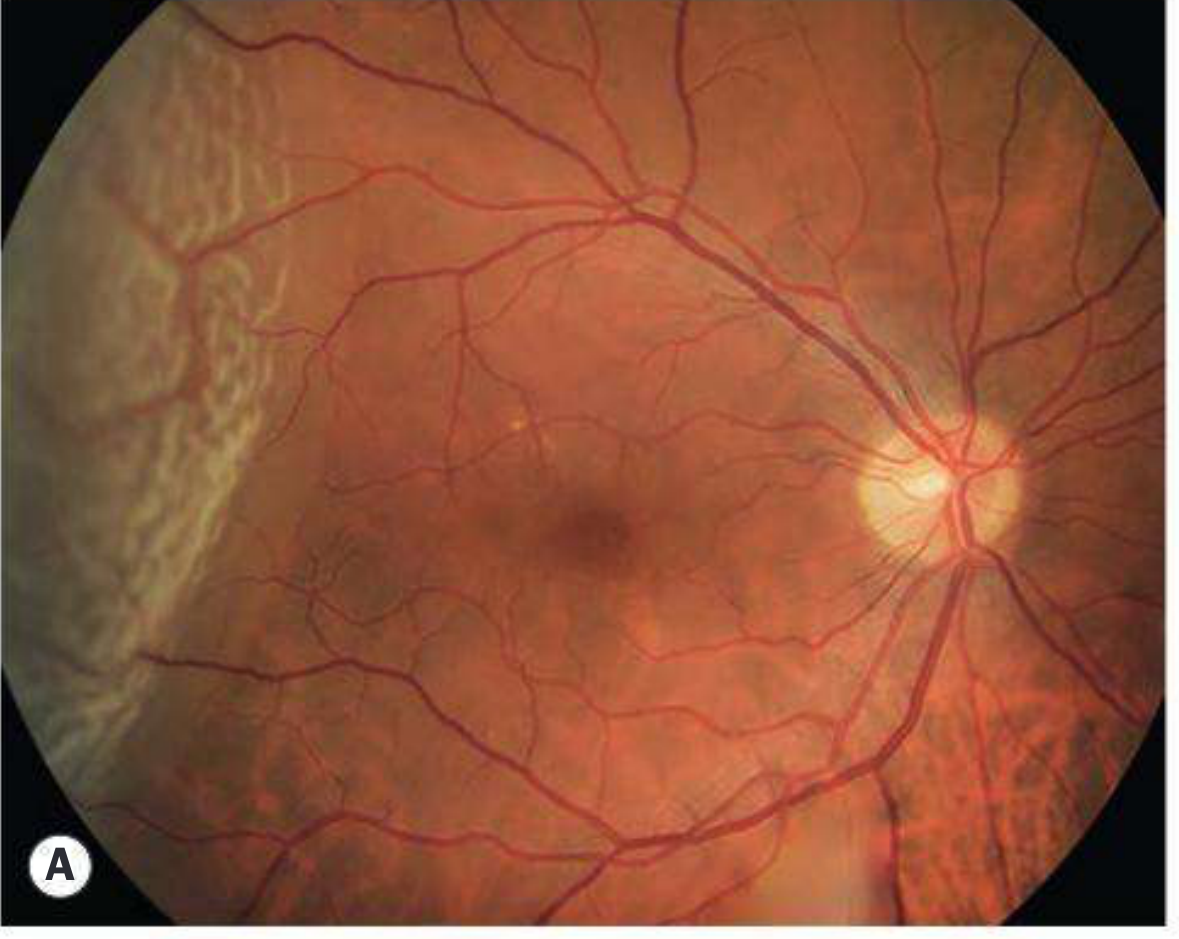
Fresh RRD — Temporal detachment with macula on (Panel A)
The temporal retina shows a pale, elevated, corrugated detachment. The macula is spared; note loss of choroidal detail under the detached area.
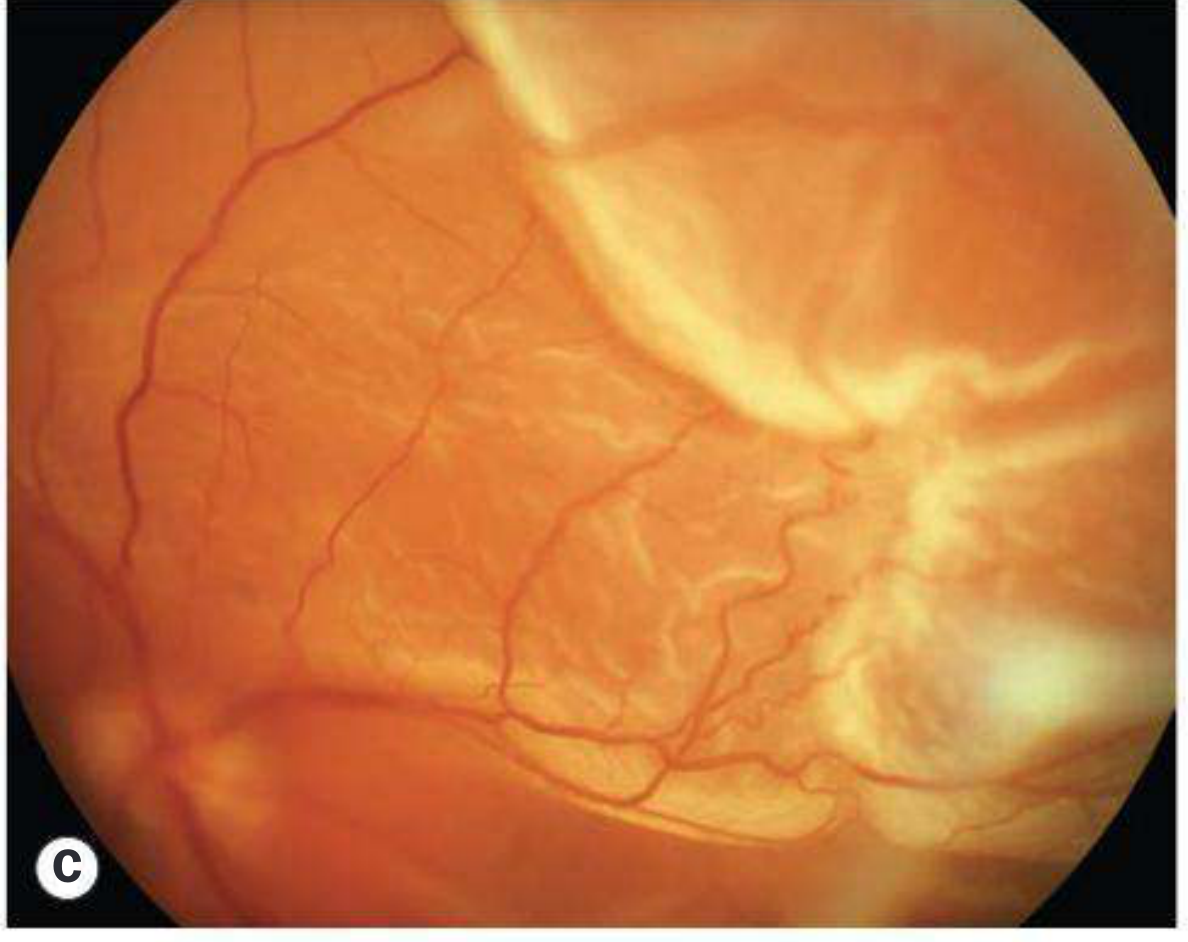
Fresh RRD — Superior bullous detachment with large tear (Panel B)
A bullous, pale-orange elevation fills the superior half of the fundus. The large tear is visible. Severe retinal wrinkling and folding are evident. This appearance is typical when the primary break lies above the horizontal meridian.
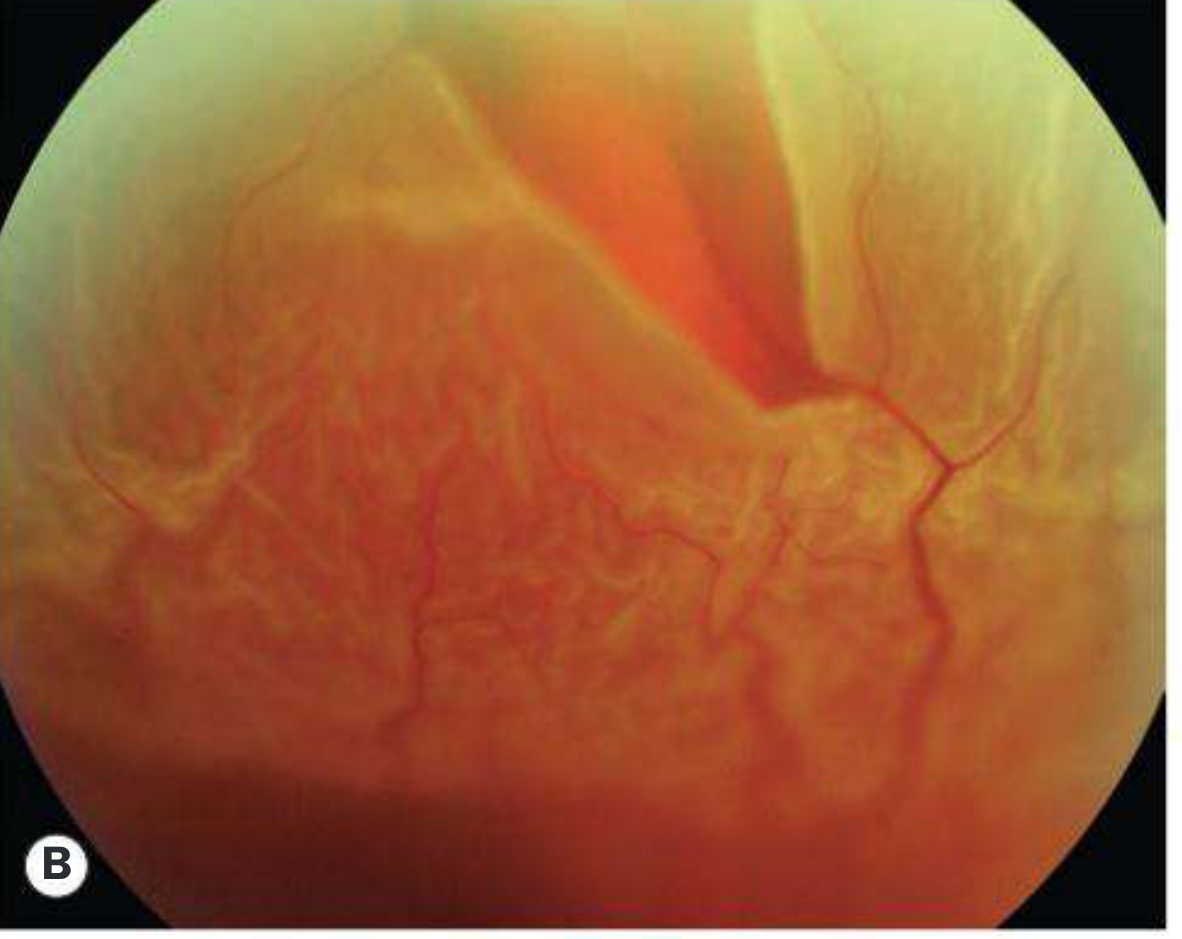
Fresh RRD — Typical corrugated retina, macula off (Panel C)
The classic corrugated (wrinkled) appearance from retinal edema. Loss of choroidal reflex behind the detached retina. Macula is involved.
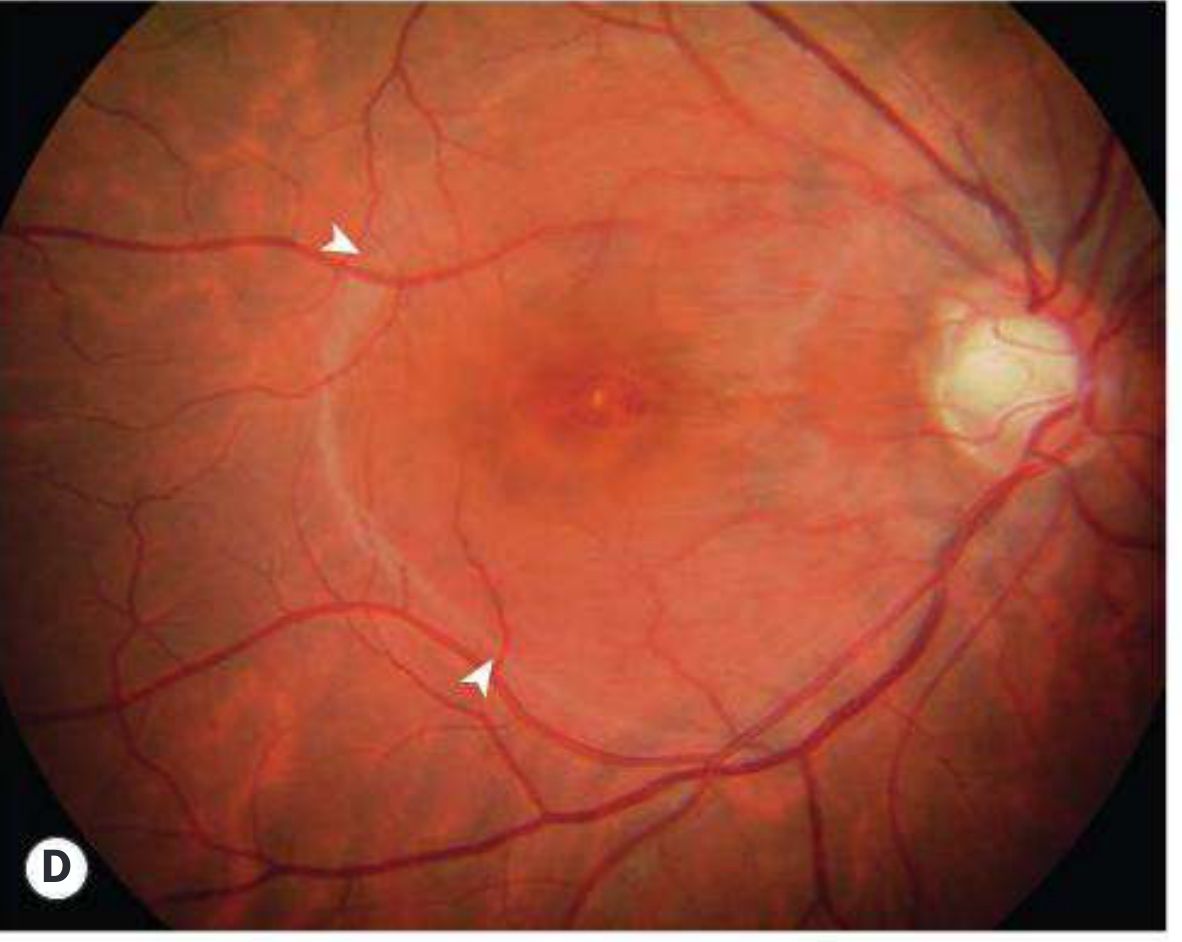
RRD — Macular hole with shallow SRF (Panel D)
A macular hole (foveal break) is surrounded by a halo of shallow subretinal fluid confined to the posterior pole (arrowheads), a characteristic presentation in highly myopic patients.
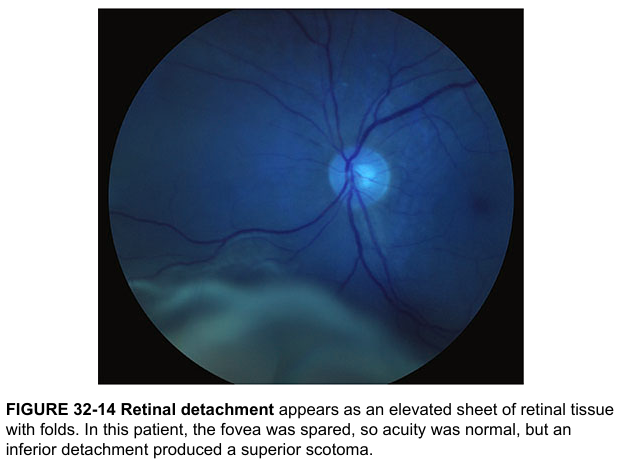
Inferior RRD — Macula spared (Harrison's Principles)
Classic fundus photograph showing an elevated, folded, pale sheet of detached retina in the inferior fundus. The optic disc and vessels are intact. The fovea is spared, so visual acuity was normal — but an inferior detachment produces a superior scotoma.
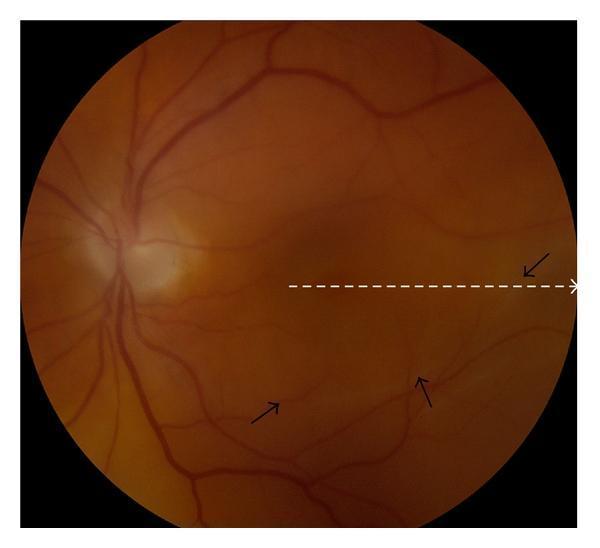
RRD — Rhegmatogenous with demarcation line and subtle inferior detachment
Color fundus photo (clinical VQA). Black arrows indicate the demarcation line of the detachment in the inferior-temporal quadrant. The dashed white line shows the OCT scanning path across the macula — useful for assessing macula-on vs. macula-off status.
2. Tractional Retinal Detachment
Causes
- Proliferative diabetic retinopathy (most common)
- Retinopathy of prematurity (ROP)
- Penetrating posterior segment trauma
Pathogenesis
Contraction of fibrovascular membranes over areas of vitreoretinal adhesion gradually pulls the retina off the RPE. PVD is gradual and incomplete.
Fundus Features
- Concave configuration (contrast with convex in RRD/exudative)
- No retinal breaks
- Reduced retinal mobility; no shifting fluid
- Fibrovascular membranes visible at the posterior pole, often along vascular arcades
3. Exudative (Serous) Retinal Detachment
Causes
- Choroidal tumors (melanoma, metastases, hemangioma) — must be excluded first
- Vogt-Koyanagi-Harada (VKH) disease / Harada syndrome
- Posterior scleritis
- Central serous chorioretinopathy (bullous form)
- Hypertensive choroidopathy (toxemia of pregnancy)
- Choroidal neovascularization
Key Diagnostic Feature: "Shifting Fluid"
The SRF shifts with gravity — collects inferiorly when upright, shifts posteriorly/superiorly when supine. This distinguishes it from RRD.
Fundus Features
- Convex and smooth surface (not corrugated — this distinguishes it from RRD)
- No vitreous pigment cells
- Underlying choroidal lesion may be visible
Longstanding RD — Specific Features
| Finding | Timeframe | Description |
|---|---|---|
| Intraretinal cysts | ~1 year | Disappear after reattachment |
| Subretinal demarcation lines | ~3 months | "High water marks" — RPE proliferation at edge of SRF |
| Retinal thinning/atrophy | Chronic | Should not be misdiagnosed as retinoschisis |
Proliferative Vitreoretinopathy (PVR) — Major Complication
Epiretinal and subretinal membrane formation leads to fixed retinal folds and rigidity. Most common after surgery for RRD or penetrating trauma.
| Grade | Features |
|---|---|
| A (Minimal) | Diffuse vitreous haze, tobacco dust, pigmented clumps |
| B (Moderate) | Inner retinal wrinkling, rolled break edges, reduced retinal mobility |
| C (Severe) | Full-thickness retinal folds, star folds, funnel-shaped detachment |
Lincoff's Rules — Predicting Break Location from SRF Pattern
| SRF Pattern | Predicted Break Location |
|---|---|
| Shallow inferior RD, slightly higher on temporal side | Inferior temporal break |
| Equal inferior fluid levels | 6 o'clock break |
| Bullous inferior RD | Break above horizontal meridian |
| Subtotal RD with superior wedge attached | Peripheral break at highest border |
| SRF crosses midline superiorly | Break near 12 o'clock |
Management Overview
Rhegmatogenous RD
| Approach | Indication |
|---|---|
| Pneumatic retinopexy | Small superior break, no PVR |
| Scleral buckle | Young phakic patients, inferior breaks, multiple breaks |
| Pars plana vitrectomy (PPV) | Complex RD, PVR, giant tears, pseudophakic RD |
Tractional RD
- PPV with membrane peeling, perfluorocarbon liquid, long-acting gas or silicone oil tamponade
- ILM peeling improves success in advanced PVR cases
Exudative RD
- Treat the underlying cause (tumor excision/brachytherapy, immunosuppression for VKH, etc.)
- Surgery not indicated for pure exudative RD without tractional component
Key Pearls
- Macula-on vs. macula-off status determines urgency: macula-on is an ophthalmic emergency (same-day surgery to prevent foveal detachment)
- Tobacco dust (Shafer's sign) in the anterior vitreous = strong indicator of RRD
- IOP is characteristically low in RRD; markedly raised IOP suggests Schwartz-Matsuo syndrome
- Shifting fluid = exudative RD until proven otherwise; always exclude choroidal melanoma
— Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 695–706; Harrison's Principles of Internal Medicine, 21st ed., p. 967
This is a shared conversation. Sign in to Orris to start your own chat.