Hydronephrosis Treatment
Reading File
Finding Sources
Searching PubMed
"hydronephrosis"[MeSH Terms] AND "treatment"[MeSH Terms]
Searching the Web
hydronephrosis treatment management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-structured answer.
Hydronephrosis: Treatment
Hydronephrosis is dilation of the renal pelvis and calyces — with accompanying parenchymal atrophy — caused by obstruction to urine outflow. Treatment is directed at the underlying cause and severity, with the shared goal of relieving obstruction and preserving renal function before irreversible damage occurs.
Grading (Guides Urgency and Approach)
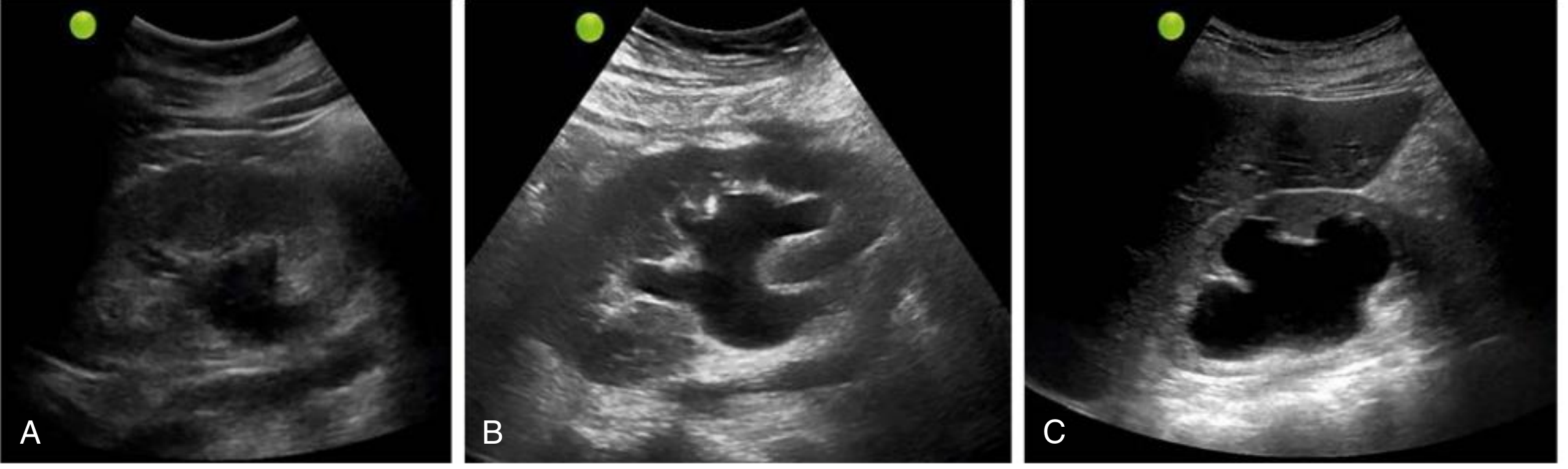
| Grade | Ultrasound Features |
|---|---|
| Mild | Renal pelvis and calyceal dilation; parenchymal architecture preserved |
| Moderate | Medullary pyramids flatten; increasing pelvicalyceal dilation |
| Severe | Ballooned pelvis/calyces occupying most of kidney; corticomedullary differentiation lost; thin parenchyma |
Principles of Management
The treatment strategy depends on:
- Acuity — acute complete obstruction vs. chronic partial obstruction
- Location of obstruction (ureteropelvic junction, ureter, ureterovesical junction, bladder outlet, urethra)
- Laterality — unilateral (above the bladder) vs. bilateral (below the bladder level)
- Cause — stone, stricture, BPH, malignancy, pregnancy, retroperitoneal fibrosis, etc.
- Presence of infection — pyonephrosis is a urologic emergency
- Renal function — split function on MAG3 renogram guides surgical vs. conservative approach
I. Emergency Decompression (Immediate Priority)
Indications for Urgent Decompression
- Infected obstructive hydronephrosis (pyonephrosis) — fever + flank pain + internal echoes on ultrasound; prompt decompression is lifesaving
- Solitary kidney with obstruction
- Bilateral obstruction with rising creatinine / oliguria / AKI
- Electrolyte abnormalities (hyperkalemia, acidosis)
- Hemodynamic instability
Methods of Decompression
1. Ureteral Stenting (Retrograde JJ Stent)
- First-line in most stable patients
- Placed cystoscopically under fluoroscopic guidance
- Internalized; allows the patient to go home
- Preferred when retrograde access is feasible
2. Percutaneous Nephrostomy (PCN)
- Indicated when retrograde stenting fails or is contraindicated (e.g., sepsis with hemodynamic instability too great for general anesthesia, impassable ureteral obstruction due to stone, tumor, or stricture)
- A nephrostomy catheter is placed under fluoroscopic/ultrasound guidance through the renal parenchyma into the collecting system
- PCN can later be converted to internal antegrade stent drainage even if retrograde stenting had failed
- Whitaker test via the PCN tract can confirm functional obstruction (differential pressure >22 cm H₂O at 10 mL/min = moderate-to-severe obstruction)
"In a critically ill patient with electrolyte abnormalities and little or no urine output, nephrostomy tube placement is favored." — Campbell-Walsh-Wein Urology
II. Cause-Specific Definitive Treatment
A. Urolithiasis (Most Common Acquired Cause)
After decompression, stone removal is achieved by:
- Extracorporeal Shock Wave Lithotripsy (ESWL) — for smaller stones (<2 cm), noninvasive
- Ureteroscopy (URS) + laser lithotripsy — ureterally located stones; direct endoscopic fragmentation
- Percutaneous Nephrolithotomy (PCNL) — large renal stones (>2 cm) or staghorn calculi
B. Ureteropelvic Junction (UPJ) Obstruction
The most common cause of hydronephrosis in children; also occurs in adults.
Indications for surgery:
- Symptomatic obstruction (flank pain, Dietl's crisis — pain with high fluid intake/diuretics)
- Associated urolithiasis
- Recurrent UTIs
- Deteriorating renal function on MAG3 renogram (T½ >20 min after furosemide)
- Split function <40% on the affected side
Surgical Options:
| Technique | Details |
|---|---|
| Dismembered Pyeloplasty (Anderson-Hynes) | Gold standard; excises the atretic UPJ segment; widely spatulates and re-anastomoses the renal pelvis to the ureter over a stent; preferred when crossing vessel is present; >90% long-term patency |
| Non-dismembered Pyeloplasty (Culp-DeWeerd / Spiral Flap) | Posterior wall kept intact; flap of redundant renal pelvis sutured as onlay over the stricture; useful when dismemberment is not needed |
| Approach | Open → Laparoscopic (introduced 1993) → Robotic (preferred in most modern centers) |
| Endopyelotomy (Antegrade/Retrograde) | Endoscopic incision of the stricture; suitable for secondary/recurrent strictures post-pyeloplasty, associated urolithiasis, or patients with major comorbidities prohibiting surgery; relative contraindications: stricture >2 cm, severe hydronephrosis, split function <25%, crossing vessel, ischemic stricture |
Relative contraindications to endoscopic management include lengthy strictures (>2 cm), severely impaired ipsilateral function (<25%), and the presence of an aberrant crossing vessel. — Hinman's Atlas of Urologic Surgery
C. Benign Prostatic Hyperplasia (BPH) / Bladder Outlet Obstruction
- Medical therapy: α-blockers (tamsulosin, alfuzosin), 5α-reductase inhibitors (finasteride, dutasteride)
- Surgical: TURP (transurethral resection of prostate), laser prostatectomy, or HoLEP for refractory cases
- Catheter drainage (urethral or suprapubic) for acute urinary retention
D. Ureteral Strictures (Iatrogenic, Radiation, Retroperitoneal Fibrosis)
Treatment options per location and stricture length:
- Endoscopic balloon dilation or incision for short strictures
- Ureteral reimplantation (distal strictures) — direct or with Psoas hitch / Boari flap
- Ureteroureterostomy (mid-ureteral, strictures <1 cm)
- Ileal ureter — for very long ureteral defects
- Nephrectomy — if split function <15% (non-functional kidney)
For retroperitoneal fibrosis: ureteral stenting → ureterolysis ± omental wrapping; corticosteroids for idiopathic RPF.
E. Malignant Obstruction (Cervical Ca, Prostate Ca, Retroperitoneal Lymphoma, Bladder Tumor)
- Ureteral stenting (JJ stent) or PCN for decompression while underlying malignancy is treated
- Metallic self-expanding ureteral stents for long-term palliation in malignant obstruction
- Definitive oncologic management (chemotherapy, radiation, surgery) per tumor type
F. Pregnancy-Associated Hydronephrosis
- Usually mild and physiological; managed conservatively
- Symptomatic cases: lateral decubitus positioning (left side), hydration
- Rarely requires stenting or PCN (reserved for symptomatic nephrolithiasis or pyonephrosis)
G. Neurogenic Bladder
- Clean intermittent catheterization (CIC)
- Anticholinergics (oxybutynin, solifenacin) for overactive bladder
- Botulinum toxin injection into detrusor
- Surgical: augmentation cystoplasty, urinary diversion
III. Pediatric and Antenatal Hydronephrosis
- Most antenatally detected hydronephrosis resolves spontaneously
- Continuous antibiotic prophylaxis (CAP) reduces febrile UTI risk in high-grade antenatal hydronephrosis (SFU grade III/IV), especially with ureteral dilation ≥7 mm, VUR, or UVJ obstruction
- VCUG indicated in neonatal period if renal insufficiency or bladder outlet obstruction is suspected
- Functional assessment with DMSA scan at 4–6 weeks; MAG3 renogram for outflow obstruction
- Pyeloplasty for UPJO with worsening function, recurrent pain, or UTIs
IV. Post-Obstructive Diuresis
After relief of bilateral obstruction or obstruction of a solitary kidney, post-obstructive diuresis can occur:
- Mechanism: accumulated urea (osmotic), impaired tubular concentrating ability, ANP elevation
- Monitor fluid and electrolyte status closely
- Replace urine output volume 50–75% with IV fluids (0.45% NaCl) to avoid volume depletion while allowing gradual diuresis to clear retained solutes
V. Monitoring After Treatment
- Serial renal ultrasound to assess resolution of dilation
- MAG3 renogram at 4–6 weeks post-intervention to confirm drainage improvement
- Serum creatinine/BUN to monitor renal recovery
- Urine culture (treat any UTI promptly — obstructed, infected systems are dangerous)
Key References:
- Sabiston Textbook of Surgery, 20e — UPJ Obstruction and Ureteral Reconstruction
- Campbell-Walsh-Wein Urology, 12e — Hydronephrosis and Obstruction
- Hinman's Atlas of Urologic Surgery — Antegrade Endopyelotomy & Laparoscopic Pyeloplasty
- Smith and Tanagho's General Urology, 19e — Percutaneous Catheter Placement
- Robbins & Kumar Basic Pathology — Pathogenesis of Hydronephrosis
- Comprehensive Clinical Nephrology, 7e — Ultrasound Grading
UTI TREATMENT
Reading File
Finding Sources
Searching PubMed
"urinary tract infection"[MeSH Terms] AND "anti-bacterial agents"[MeSH Terms]
Searching the Web
UTI treatment guidelines 2024 2025 antibiotics uncomplicated complicated
Finding Sources
Reading File
Reading Web Page
UTI treatment antibiotics duration 2025 IDSA guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive, authoritative data from multiple major textbooks plus the 2025 IDSA guidelines update. I have everything needed to write a thorough answer.
Urinary Tract Infection (UTI): Treatment
Classification (Determines Treatment)
| Type | Definition |
|---|---|
| Uncomplicated UTI | Infection confined to the bladder in otherwise healthy, non-pregnant women with a normal urinary tract |
| Complicated UTI (cUTI) | UTI beyond the bladder OR in the presence of comorbidities/structural/functional abnormalities (includes pyelonephritis, CAUTI, UTI in men, obstruction, immunosuppression, diabetes, pregnancy, neurogenic bladder, recent instrumentation) |
| Uncomplicated pyelonephritis | Fever + flank pain ± vomiting in a woman with anatomically normal urinary tract and no comorbidities |
| CAUTI | UTI in a person currently or recently (within 48 h) catheterized; ≥10³ CFU/mL with symptoms |
| Asymptomatic bacteriuria | ≥10⁵ CFU/mL without symptoms — treat only in pregnancy and pre-urologic procedure |
Common Pathogens
- E. coli (80% of community-acquired UTI)
- Staphylococcus saprophyticus (young sexually active women)
- Klebsiella pneumoniae, Proteus mirabilis, Enterococcus faecalis
- Pseudomonas aeruginosa, Enterobacter — hospital-acquired/complicated/catheter-associated
I. Uncomplicated Cystitis (Women)
Clinical diagnosis based on dysuria, frequency, urgency in the absence of vaginal discharge or irritation. Urine culture not required for typical uncomplicated cystitis.
First-Line Agents
| Antibiotic | Dose (Oral) | Duration | Notes |
|---|---|---|---|
| Nitrofurantoin (macrocrystal/monohydrate) | 100 mg twice daily | 5 days | First-line; effective vs. E. coli; inactive vs. Proteus, Pseudomonas; avoid if CrCl <30 mL/min; not for pyelonephritis (poor tissue penetration) |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | 160/800 mg (DS) twice daily | 3 days | First-line if local resistance <20%; avoid in third trimester of pregnancy |
| Fosfomycin | 3 g as single dose | Once | Useful for multidrug-resistant organisms (ESBL); only for E. coli cystitis; convenient for ED use; reserve to prevent resistance development |
Second-Line Agents (use only when first-line agents are not feasible)
- Fluoroquinolones (ciprofloxacin 250 mg BID × 3 days; levofloxacin 250 mg × 3 days) — NOT first-line for uncomplicated cystitis due to adverse effects (tendinopathy, CNS effects) and resistance promotion
- Beta-lactams (cephalexin 500 mg BID × 5–7 days; amoxicillin-clavulanate 500 mg BID × 5–7 days) — inferior cure rates; use when no alternatives
"Fluoroquinolones such as ciprofloxacin or levofloxacin should not be used as first-line agents for empirical treatment of uncomplicated UTIs. Instead, they should be reserved for patients who have failed or have contraindications to first-line antibiotics." — Rosen's Emergency Medicine
Symptomatic Relief
- Phenazopyridine (Pyridium) 200 mg TID for 1–2 days — urinary analgesic; relieves dysuria; warn patients of orange-red urine discoloration; not an antibiotic
II. Acute Uncomplicated Pyelonephritis
Outpatient (Mild–Moderate, Patient Can Tolerate Oral Intake)
| Antibiotic | Dose (Oral) | Duration |
|---|---|---|
| Ciprofloxacin | 500 mg twice daily | 7 days |
| Levofloxacin | 750 mg once daily | 5 days |
| TMP-SMX | 160/800 mg twice daily | 10–14 days |
- Fluoroquinolones are first-line for pyelonephritis (excellent tissue/blood penetration)
- If local fluoroquinolone resistance >10%: give initial parenteral dose (ceftriaxone 1 g IV/IM) then 10–14 days oral cephalosporin
- Nitrofurantoin and fosfomycin are contraindicated for pyelonephritis — they do not achieve adequate renal tissue/blood levels
Inpatient (Severe, Vomiting, Sepsis Signs, Inability to Tolerate PO)
Start empiric parenteral therapy; transition to oral after 24–48 h afebrile:
| Agent | Dose (IV) |
|---|---|
| Ceftriaxone | 1–2 g IV once daily |
| Ciprofloxacin | 400 mg IV every 12 h |
| Cefepime | 1–2 g IV every 8 h |
| Piperacillin-tazobactam | 3.375 g IV every 6 h |
| Ertapenem | 1 g IV once daily |
| Meropenem / Imipenem | 500 mg–1 g IV every 8 h (reserved for ESBL/resistant organisms) |
| Gentamicin/tobramycin | 3 mg/kg/day divided every 8 h ± ampicillin 2 g every 6 h |
Total treatment duration: 7–14 days (5–7 days with fluoroquinolones; 7–10 days with beta-lactams per 2025 IDSA guidelines)
2025 IDSA Update: For cUTI with clinical improvement on appropriate antibiotics, shorter courses are supported — 5–7 days fluoroquinolone or 7 days non-fluoroquinolone (vs. traditional 10–14 days). However, shorter durations are not appropriate for patients with indwelling catheters, severe sepsis, significant immunocompromise, renal abscesses, CKD, complete obstruction, or recent urologic procedures.
III. Complicated UTI (cUTI)
2025 IDSA Four-Step Framework for Empiric Therapy:
- Assess severity — Is the patient septic?
- Review patient-specific risk factors for resistant organisms (recent antibiotics, healthcare exposure, prior ESBL/MDR infection, travel)
- Consider allergies and drug interactions
- Consult local antibiogram (mandatory if septic)
Empiric Antibiotic Choices for cUTI
| Severity | Preferred Agents | Duration |
|---|---|---|
| Non-septic, stable | 3rd/4th-gen cephalosporins, piperacillin-tazobactam, or fluoroquinolones PO/IV | 7 days (FQ) or 7–10 days (non-FQ) |
| Septic | Carbapenems or newer beta-lactam/beta-lactamase inhibitors based on local antibiogram | Individualize; 7–14 days |
| ESBL-producing organisms | Ertapenem, meropenem (preferred); carbapenem-sparing with quinolones or cefepime if susceptible | 7–14 days |
| Pseudomonas | Ciprofloxacin 400 mg IV q8–12h, levofloxacin 750 mg IV, piperacillin-tazobactam, cefepime, ceftazidime, or aminoglycoside | 7–10 days |
| Difficult-to-treat Pseudomonas / CRE | Ceftazidime-avibactam, ceftolozane-tazobactam, imipenem-cilastatin-relebactam, cefiderocol | Per ID consultation |
IV-to-Oral Switch
- Acceptable once patient is clinically improving and can tolerate oral intake
- Preferred oral step-down: Fluoroquinolones or TMP-SMX (high bioavailability)
- Oral beta-lactams: acceptable if susceptible and adequate serum/urinary concentrations expected; duration may need to extend to 10–14 days
IV. Catheter-Associated UTI (CAUTI)
- Remove or replace catheter before collecting culture and initiating antibiotics
- Treat only if symptomatic (fever, rigors, altered mental status, flank pain, suprapubic tenderness) — asymptomatic bacteriuria with a catheter should not be treated
- Antibiotic choice: same as cUTI, guided by culture results
- Duration: 7 days if prompt clinical response; 10–14 days if delayed response
V. UTI in Men
- All UTIs in men are considered complicated (rule out prostatitis, epididymo-orchitis, structural abnormality)
- Treat for 7–14 days (7 days if no immunocompromise or complications per recent evidence)
- If prostatitis suspected: TMP-SMX or fluoroquinolone for 14 days (fluoroquinolones preferred for prostate tissue penetration)
- Refer to urology for recurrent UTI, hematuria, or suspicion of prostatic involvement
VI. UTI in Pregnancy
- Screen all pregnant women with urine culture at 12–16 weeks (USPSTF Grade A)
- Treat asymptomatic bacteriuria — up to 30% will develop pyelonephritis if untreated
- Safe agents in pregnancy:
- Cephalexin 500 mg BID × 3–7 days
- Nitrofurantoin 100 mg BID × 3–7 days (avoid at term/third trimester — risk of neonatal hemolysis)
- Amoxicillin 500 mg TID × 7 days
- TMP-SMX (avoid in first trimester [neural tube defects] and third trimester [kernicterus])
- Pyelonephritis in pregnancy → admit for IV ceftriaxone 1 g daily; follow-up culture post-treatment mandatory
VII. Recurrent UTI (Women)
Defined as ≥2 UTIs in 6 months or ≥3 in 12 months.
| Strategy | Details |
|---|---|
| Continuous prophylaxis | TMP-SMX 40/200 mg or nitrofurantoin 50–100 mg nightly × 6–12 months |
| Post-coital prophylaxis | Single dose TMP-SMX or nitrofurantoin within 2 h of intercourse |
| Self-start therapy | Patient-initiated 3-day course at symptom onset; requires prior positive culture confirmation |
| Non-antibiotic measures | Cranberry products (modest evidence), topical vaginal estrogen (postmenopausal), avoid spermicides, adequate hydration, post-coital voiding |
VIII. Resistant Organisms — Special Agents
| Organism | Preferred Treatment |
|---|---|
| ESBL-producing E. coli / Klebsiella | Ertapenem or meropenem; carbapenem-sparing with FQ/cefepime if susceptible |
| KPC-producing CRE | Ceftazidime-avibactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam |
| NDM-producing CRE | Ceftazidime-avibactam + aztreonam, cefiderocol |
| Difficult-to-treat Pseudomonas | Ceftazidime-avibactam, ceftolozane-tazobactam, cefiderocol |
For Pseudomonas UTI: "Urinary catheters, stents, or stones should be removed if possible. In general, 7 to 10 days of antibiotic treatment will suffice." — Goldman-Cecil Medicine
IX. When to Admit
| Indication | Action |
|---|---|
| Unable to tolerate oral fluids/medication | Admit for IV antibiotics + hydration |
| Systemic signs (fever, hypotension, rigors) suggesting urosepsis | Admit; treat as sepsis per surviving sepsis guidelines |
| Obstruction + UTI (pyonephrosis) | Emergency decompression (PCN or ureteral stent) + IV antibiotics |
| Immunocompromised / diabetic with complicated pyelonephritis | Admit |
| Pyelonephritis in pregnancy | Admit, obstetric consultation |
| Suspected renal/perirenal abscess | Admit; drain if ≥3 cm + prolonged antibiotics (4–6 weeks) |
Quick Reference: Treatment Duration Summary
| Condition | Duration |
|---|---|
| Uncomplicated cystitis (nitrofurantoin) | 5 days |
| Uncomplicated cystitis (TMP-SMX) | 3 days |
| Uncomplicated cystitis (fosfomycin) | Single dose |
| Uncomplicated pyelonephritis (FQ) | 7 days |
| Uncomplicated pyelonephritis (TMP-SMX) | 10–14 days |
| Complicated UTI (FQ, clinical improvement) | 5–7 days (2025 IDSA) |
| Complicated UTI (non-FQ, clinical improvement) | 7 days (2025 IDSA) |
| Bacteremic UTI (gram-negative) | 7 days (BALANCE trial — non-inferior to 14 days) |
| cUTI with oral beta-lactam step-down | 10–14 days (individualized) |
| CAUTI (prompt response) | 7 days |
| Prostatitis | 14 days (FQ or TMP-SMX) |
| Renal/perirenal abscess | 4–6 weeks |
Key References:
- Rosen's Emergency Medicine, 9e — Uncomplicated & Complex UTI Treatment
- Tintinalli's Emergency Medicine, 9e — UTI Classification, Complicated UTI Tables
- Goldman-Cecil Medicine, 26e — Pseudomonas UTI, ESBL/CRE Treatment
- Comprehensive Clinical Nephrology, 7e — UTI Classification
- 2025 IDSA Guideline on Complicated UTI — Four-step framework, shorter duration evidence, BALANCE trial
This is a shared conversation. Sign in to Orris to start your own chat.