Explain heart murmurs in detail (easily)
Reading File
Finding Sources
Finding Sources
Searching Images
heart murmur auscultation cardiac cycle diagram
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from Harrison's and Braunwald's. Let me compile the complete, easy-to-understand explanation.
Heart Murmurs — A Complete, Easy Guide
What Is a Heart Murmur?
A heart murmur is simply an extra sound heard between the normal "lub-dub" heartbeats when a doctor listens with a stethoscope. Normal heart sounds (S1 = "lub", S2 = "dub") are made by heart valves snapping shut. A murmur is the sound of turbulent blood flow — like the sound of water rushing through a narrow pipe.
Murmurs are caused by:
- Accelerated blood flow through a normal or abnormal opening (e.g., fever, anemia, pregnancy)
- Flow through a narrowed/irregular orifice into a wider chamber — like aortic stenosis
- Backward (regurgitant) flow through a leaky valve or defect — like mitral regurgitation
Are All Murmurs Dangerous?
No! Murmurs are divided into two main categories:
| Type | Meaning | Action Needed? |
|---|---|---|
| Innocent (Functional) | No structural heart problem; common in children, athletes, pregnancy, fever, anemia | Usually none |
| Pathological | Caused by a valve defect, hole in the heart, or structural disease | Further workup required |
A soft midsystolic murmur in an asymptomatic child or young adult is almost always innocent and does not require an echocardiogram. — Harrison's Principles of Internal Medicine (2025)
How Are Murmurs Described?
1. Timing — When in the Heartbeat?
This is the most important feature. The cardiac cycle has two phases:
- Systole = when the heart squeezes (pumps blood out) → between S1 and S2
- Diastole = when the heart relaxes (fills with blood) → between S2 and the next S1
Types by timing:
| Timing | When Heard | Classic Causes |
|---|---|---|
| Early systolic | Starts at S1, fades before S2 | Acute mitral regurgitation, small VSD |
| Midsystolic (ejection) | Starts after S1, peaks in mid-systole, fades before S2 | Aortic stenosis, pulmonic stenosis |
| Holosystolic (pansystolic) | Spans entire systole from S1 to S2, plateau-shaped | Mitral regurgitation, tricuspid regurgitation, VSD |
| Late systolic | Starts mid-systole, ends at S2 | Mitral valve prolapse |
| Early diastolic | Starts at S2, decrescendo | Aortic regurgitation, pulmonary regurgitation |
| Mid-diastolic | Starts after S2, low rumbling sound | Mitral stenosis, tricuspid stenosis |
| Presystolic | Just before S1, in sinus rhythm | Mitral/tricuspid stenosis |
| Continuous | Runs through both S1 and S2 | Patent ductus arteriosus (PDA) — "machinery murmur" |
Here is a visual reference showing exactly when each murmur type occurs in the cardiac cycle:
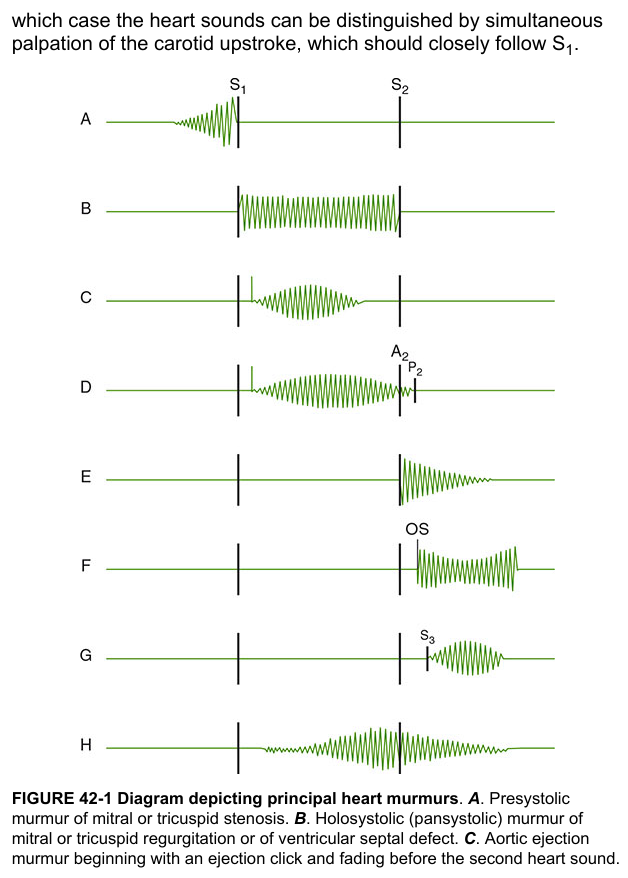
2. Intensity (Loudness) — Graded I to VI
| Grade | Description |
|---|---|
| I/VI | Very soft; heard only with great effort |
| II/VI | Easily heard, but not loud |
| III/VI | Loud, no thrill felt |
| IV/VI | Loud + palpable thrill (vibration felt on chest) |
| V/VI | Heard with only the edge of the stethoscope touching the chest |
| VI/VI | Heard with stethoscope slightly off the chest |
Clinical rule: Grade ≥ III usually signals important structural heart disease and warrants echocardiography. — Harrison's, 2025
A thrill = a grade IV+ murmur. You can actually feel it vibrating with your hand.
3. Shape / Configuration
| Shape | What It Sounds Like | Example |
|---|---|---|
| Crescendo | Gets louder → | Presystolic murmur of mitral stenosis |
| Decrescendo | Gets softer ← | Aortic regurgitation |
| Crescendo-decrescendo | Builds then fades (diamond shape) | Aortic stenosis |
| Plateau (flat) | Steady throughout | Mitral regurgitation |
4. Location & Radiation — Where on the Chest?
Each murmur is loudest in a specific area and may radiate:
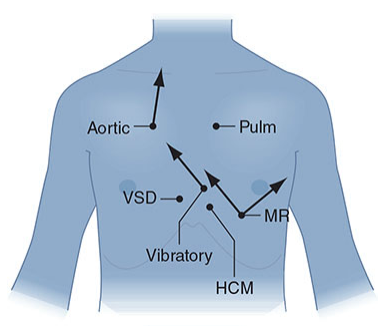
| Murmur | Best Heard At | Radiates To |
|---|---|---|
| Aortic stenosis | Right upper sternal border (2nd R intercostal space) | Neck/carotids |
| Mitral regurgitation (MR) | Apex (left midclavicular line) | Left axilla |
| Pulmonic stenosis | Left upper sternal border (2nd L intercostal space) | Left shoulder |
| VSD | Left lower sternal border | Across entire precordium |
| HCM | Left lower sternal border to apex | — |
5. Quality (Sound Character)
| Quality | Example |
|---|---|
| Blowing, high-pitched | Aortic regurgitation, mitral regurgitation |
| Harsh, rough | Aortic stenosis, VSD |
| Low rumbling | Mitral stenosis (best heard with bell of stethoscope) |
| Machinery-like | Patent ductus arteriosus (PDA) |
Common Specific Murmurs — Quick Reference
🔴 Aortic Stenosis (AS)
- Midsystolic, crescendo-decrescendo (diamond shape)
- Harsh, heard at right upper sternal border, radiates to carotids
- Due to: calcified/narrowed aortic valve → LV has to push hard
- Signs of severity: parvus et tardus pulse (weak, slow carotid upstroke), soft A2
🔴 Mitral Regurgitation (MR)
- Holosystolic (pansystolic), plateau
- Blowing, best at apex, radiates to left axilla
- Due to: leaky mitral valve → blood flows backward into left atrium during systole
🔴 Aortic Regurgitation (AR)
- Early diastolic, decrescendo
- Blowing, high-pitched, heard at left sternal border leaning forward
- Due to: incompetent aortic valve → blood leaks back into LV during diastole
🔴 Mitral Stenosis (MS)
- Mid-diastolic rumble, follows opening snap (OS)
- Low-pitched, heard at apex with bell of stethoscope
- Due to: thickened/fused mitral leaflets (often from rheumatic fever) → LA-LV gradient
🔴 VSD (Ventricular Septal Defect)
- Holosystolic, harsh, loud (Grade IV+)
- Left lower sternal border
- Small VSD = louder murmur (high-velocity jet through tiny hole)
🔴 PDA (Patent Ductus Arteriosus)
- Continuous "machinery" murmur (runs through S2)
- Left upper sternal border
- Due to: persistent connection between aorta and pulmonary artery after birth
🟡 HCM (Hypertrophic Obstructive Cardiomyopathy)
- Midsystolic, between lower left sternal border and apex
- Unique behavior: gets louder with Valsalva or standing (decreased preload); gets softer with squatting (increased preload)
Bedside Maneuvers — How to Identify Murmurs
| Maneuver | Effect on HCM | Effect on AS/MR |
|---|---|---|
| Valsalva (strain) | Louder ↑ | Softer ↓ |
| Standing quickly | Louder ↑ | Softer ↓ |
| Squatting | Softer ↓ | Louder ↑ |
| Passive leg raise | Softer ↓ | Louder ↑ |
The rule: less blood in the heart (↓ preload) → HCM murmur worsens; more blood → HCM murmur improves. All other outflow murmurs do the opposite.
When to Get an Echo?
| Situation | Recommendation |
|---|---|
| Soft midsystolic (I-II/VI), asymptomatic child/young adult | Echo usually not needed |
| Loud systolic ≥ Grade III/VI | Echo indicated |
| Holosystolic or late systolic murmur | Echo indicated |
| Any diastolic murmur | Echo indicated |
| Continuous murmur | Echo indicated |
Summary
Think of a heart murmur as the sound of turbulence — like hearing water rush through a narrowed pipe. The key questions when evaluating any murmur:
- When does it occur? (systolic vs. diastolic vs. continuous)
- How loud? (Grade I–VI)
- What shape? (crescendo, decrescendo, plateau)
- Where is it heard, and where does it radiate?
- What does it sound like? (blowing, harsh, rumbling)
- How does it respond to maneuvers?
Answering these questions systematically almost always leads to the correct diagnosis — even before doing an echocardiogram.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Braunwald's Heart Disease, The Harriet Lane Handbook 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.