BIRADS
Reading File
Finding Sources
Searching PubMed
BI-RADS breast imaging classification
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Here is a complete, structured overview of the BI-RADS system, sourced from Fischer's Mastery of Surgery (8th ed.), Bailey & Love's Short Practice of Surgery (28th ed.), and Berek & Novak's Gynecology:
BI-RADS (Breast Imaging Reporting and Data System)
Developed by the American College of Radiology (ACR), BI-RADS provides a standardized lexicon and classification system for breast imaging reports across mammography, ultrasound, and MRI. Its purpose is to eliminate ambiguity, ensure consistent communication between radiologists and clinicians, and link each finding directly to a management action.
BI-RADS Assessment Categories
| Category | Assessment | Malignancy Risk | Management |
|---|---|---|---|
| 0 | Incomplete - needs additional imaging | N/A | Recall for additional imaging or prior film comparison |
| 1 | Negative | ~0% | Routine annual screening |
| 2 | Benign finding | ~0% | Routine annual screening |
| 3 | Probably benign | >0% but ≤2% | Short-interval follow-up (6 months) |
| 4 | Suspicious | >2% to <95% | Tissue biopsy |
| 5 | Highly suggestive of malignancy | ≥95% | Tissue biopsy / surgical treatment |
| 6 | Known biopsy-proven malignancy | N/A | Surgical excision when clinically appropriate |
Category 4 Subcategories (Important for Clinical Practice)
Category 4 is subdivided to guide biopsy urgency:
| Subcategory | Suspicion Level | Malignancy Risk |
|---|---|---|
| 4A | Low suspicion | >2% to ≤10% |
| 4B | Intermediate suspicion | >10% to ≤50% |
| 4C | Moderate-high suspicion | >50% to <95% |
These subdivisions help the clinician weigh biopsy options and counsel patients on risk before tissue diagnosis.
Clinical Examples
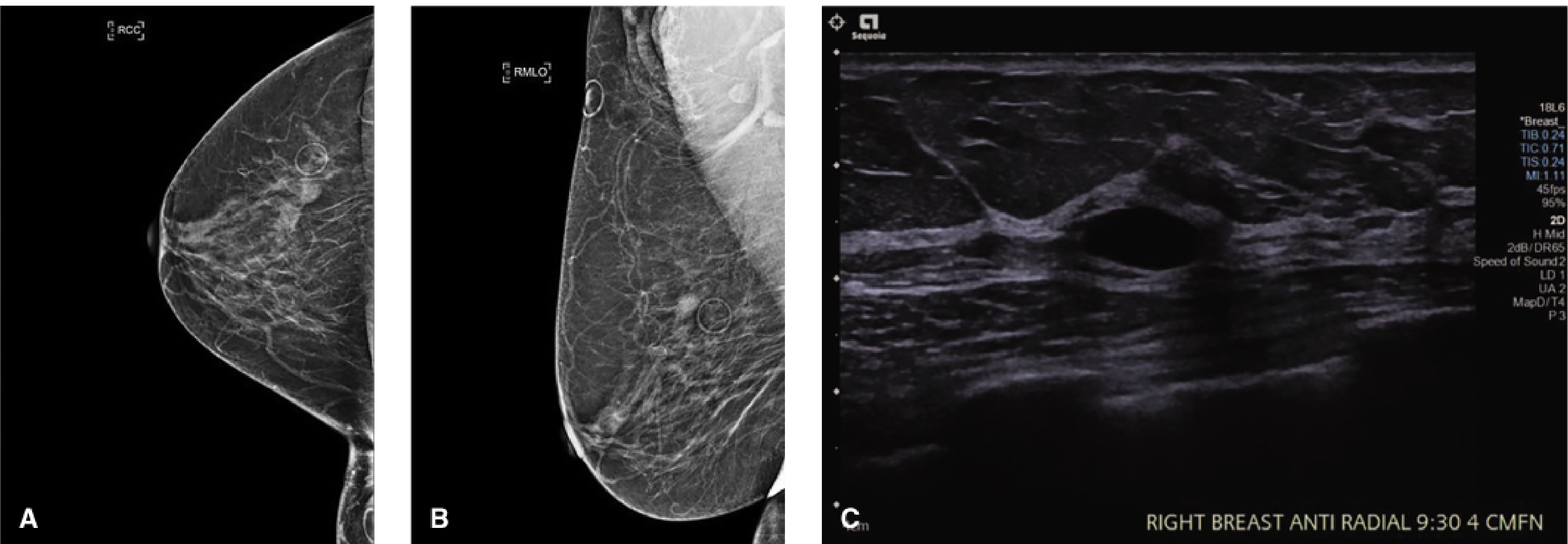
BI-RADS 2 (Benign) - Oval, circumscribed, anechoic mass on ultrasound with posterior through-transmission = simple cyst. Returns to routine 1-year screening.
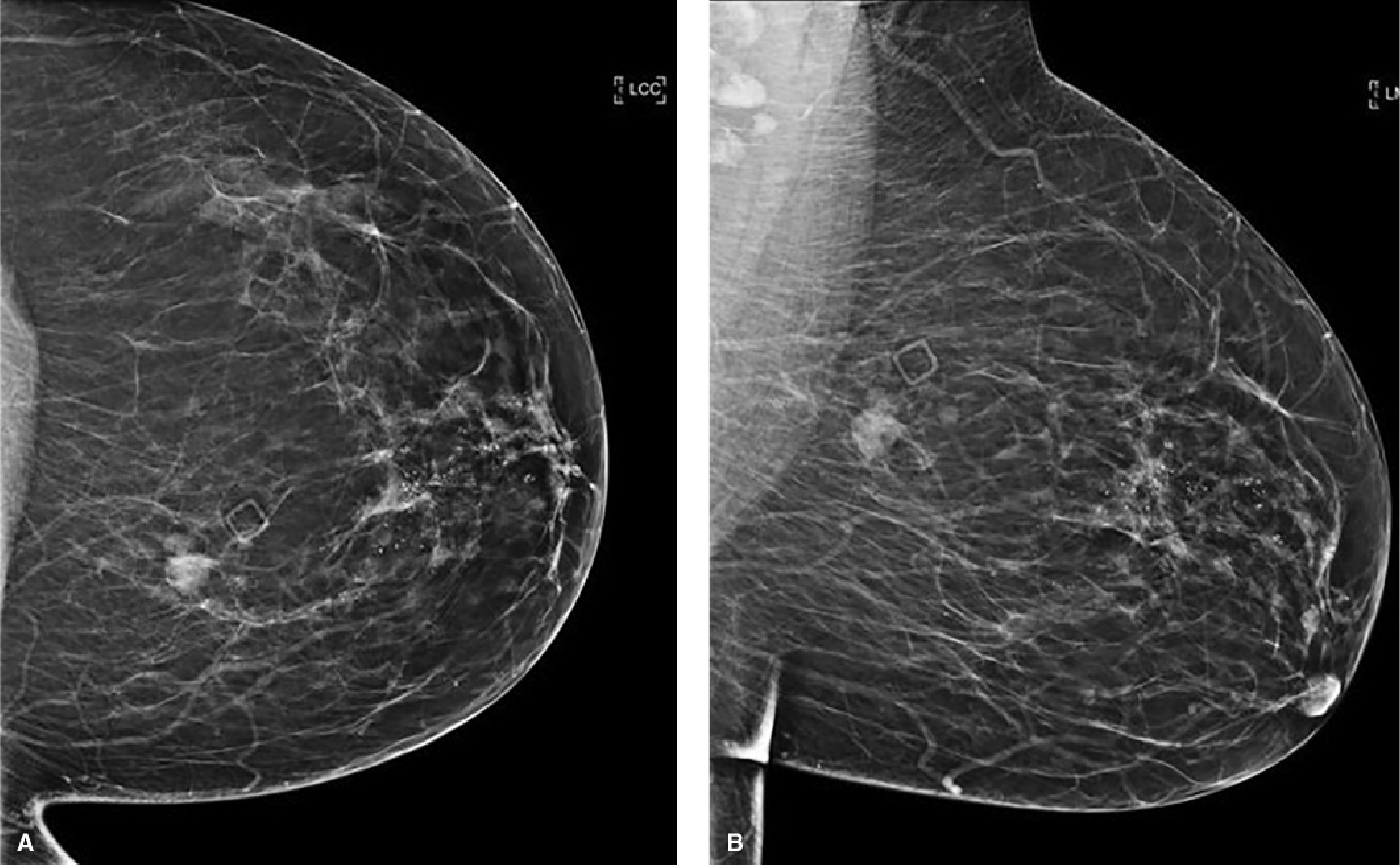
BI-RADS 4/5 (Suspicious/Malignant) - Irregular mass with indistinct/microlobulated margins plus segmental fine pleomorphic calcifications. Biopsy confirmed invasive ductal carcinoma with DCIS.
Key Points by Category
Category 0
- Used almost exclusively in screening (not diagnostic) settings
- Requires comparison with prior films OR spot compression / ultrasound / MRI
Category 1 vs. 2
- Both recommend routine follow-up, but Category 2 requires a positive finding to be described (e.g., calcified fibroadenoma, fat-containing lesion) - it is not just "nothing seen"
- Category 1 means truly negative with nothing to comment on
Category 3
- Reserved for findings with a ≤2% malignancy risk - not "probably benign" arbitrarily
- Classic examples: non-calcified circumscribed solid mass, focal asymmetry, cluster of round calcifications
- Follow-up protocol: 6-month unilateral, then 12-month bilateral, then 24-month bilateral mammogram
- If stable over 2-3 years, can be downgraded to Category 2
Category 4
- Covers a very wide range of findings; subdivisions 4A/4B/4C help guide counseling
- Tissue diagnosis is mandatory - do not "watch" a Category 4
Category 5
- Features: spiculated mass, linear or branching calcifications, architectural distortion
- Even before biopsy, treatment planning (e.g., sentinel node biopsy) may begin
Category 6
- Used for monitoring response to neoadjuvant therapy on serial imaging in a known cancer
- Not assigned after surgical excision
Modality-Specific Notes
Mammography:
- Sensitivity ~80%, specificity 80-95% (affected by breast density, age, hormone use, tumor size)
- Reduced sensitivity in dense breasts - hence adjunctive ultrasound or MRI in high-risk patients
- Digital breast tomosynthesis (DBT, 3D mammography) increases cancer detection by 1.2-4.6/1,000 and reduces recall rates by 15-65% vs. standard 2D FFDM
Ultrasound:
- Modality of choice to distinguish cystic vs. solid masses
- Used as adjunct screening in women with dense breasts
- Higher false-positive rate than mammography
- BI-RADS descriptors: shape (oval/round/irregular), orientation (parallel/not parallel), margin (circumscribed/not circumscribed), echo pattern, posterior features
MRI:
- Most sensitive modality for breast cancer detection
- Indications: BRCA/genetic mutation carriers, staging lobular carcinoma/high-grade DCIS, breast implant evaluation
- MRI-guided biopsy for lesions seen only on MRI
Mammography Sensitivity Caveat
"Mammography is never a substitute for biopsy because it may not reveal clinical cancer, especially when it occurs in the dense breast tissue of young women." - Berek & Novak's Gynecology
A palpable dominant or suspicious mass warrants biopsy regardless of mammographic findings.
Sources: Fischer's Mastery of Surgery, 8th ed. | Bailey & Love's Short Practice of Surgery, 28th ed. | Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.