Create a very simple easy flowchart cover the approach on heamoglobinopathy . Include everything simply
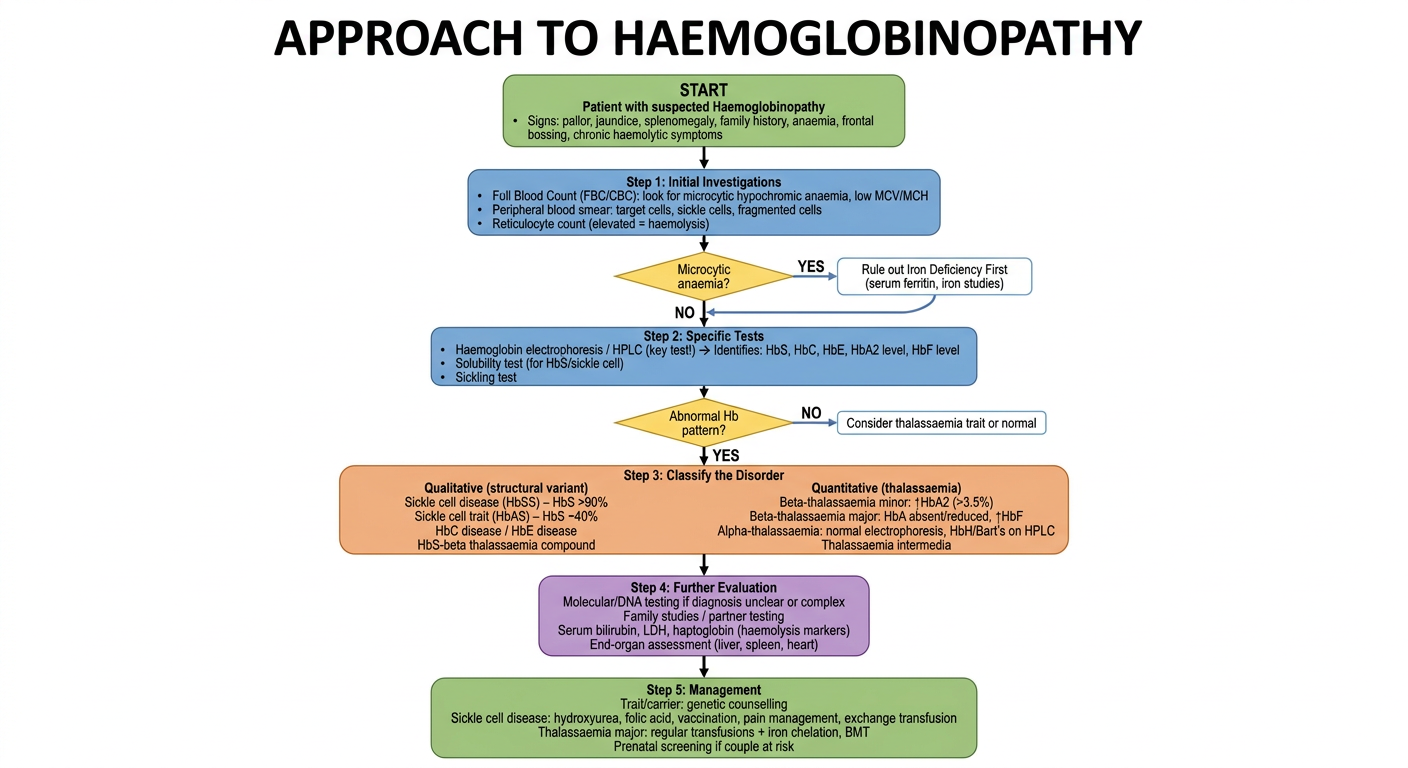
A clean, simple medical flowchart titled "Approach to Haemoglobinopathy" with the following steps flowing downward with arrows: START BOX (green): "Patient with suspected Haemoglobinopathy" - Signs: pallor, jaundice, splenomegaly, family history, anaemia, frontal bossing, chronic haemolytic symptoms STEP 1 BOX (blue): "Step 1: Initial Investigations" - Full Blood Count (FBC/CBC): look for microcytic hypochromic anaemia, low MCV/MCH - Peripheral blood smear: target cells, sickle cells, fragmented cells - Reticulocyte count (elevated = haemolysis) DIAMOND DECISION (yellow): "Microcytic anaemia?" - YES arrow leads right → "Rule out Iron Deficiency First" (serum ferritin, iron studies) - NO arrow leads down After ruling out iron deficiency, merge back down STEP 2 BOX (blue): "Step 2: Specific Tests" - Haemoglobin electrophoresis / HPLC (key test!) → Identifies: HbS, HbC, HbE, HbA2 level, HbF level - Solubility test (for HbS/sickle cell) - Sickling test DIAMOND DECISION (yellow): "Abnormal Hb pattern?" - YES → leads to Classification Box - NO → Consider thalassaemia trait or normal STEP 3 BOX (orange): "Step 3: Classify the Disorder" Two branches: LEFT BRANCH - "Qualitative (structural variant)" • Sickle cell disease (HbSS) – HbS >90% • Sickle cell trait (HbAS) – HbS ~40% • HbC disease / HbE disease • HbS-beta thalassaemia compound RIGHT BRANCH - "Quantitative (thalassaemia)" • Beta-thalassaemia minor: ↑HbA2 (>3.5%) • Beta-thalassaemia major: HbA absent/reduced, ↑HbF • Alpha-thalassaemia: normal electrophoresis, HbH/Bart's on HPLC • Thalassaemia intermedia STEP 4 BOX (purple): "Step 4: Further Evaluation" - Molecular/DNA testing if diagnosis unclear or complex - Family studies / partner testing - Serum bilirubin, LDH, haptoglobin (haemolysis markers) - End-organ assessment (liver, spleen, heart) FINAL BOX (green): "Step 5: Management" - Trait/carrier: genetic counselling - Sickle cell disease: hydroxyurea, folic acid, vaccination, pain management, exchange transfusion - Thalassaemia major: regular transfusions + iron chelation, BMT - Prenatal screening if couple at risk Style: clean white background, clear bold text, pastel colored boxes, simple straight arrows, professional medical education style. Easy to read at a glance.
-
Clinical Suspicion - Pallor, jaundice, splenomegaly, chronic anaemia, family history, frontal bossing
-
Initial Investigations - FBC (look for low MCV/MCH), peripheral blood smear (target cells, sickle cells), reticulocyte count
-
Key Diagnostic Test: Hb Electrophoresis / HPLC - This is the cornerstone test. It identifies HbS, HbC, HbE, HbA2 and HbF levels. Always rule out iron deficiency first if microcytic anaemia is present.
-
Classify the Disorder:
- Qualitative (structural): Sickle cell disease, HbC, HbE, compound heterozygotes
- Quantitative (thalassaemia): Beta-thal minor (raised HbA2 >3.5%), Beta-thal major (absent HbA, raised HbF), Alpha-thal (normal electrophoresis, HbH on HPLC)
-
Management:
- Carriers: genetic counselling + partner screening
- Sickle cell disease: hydroxyurea, folic acid, vaccinations
- Thalassaemia major: transfusions + iron chelation, consider BMT
Make the flowchart decision making on finding the type of heamoglobinopathy in peadiatrics
A detailed, clean, professional medical decision-making flowchart titled "Paediatric Haemoglobinopathy: Finding the Type" on a white background. The flowchart uses a top-down structure with clearly labeled decision diamonds (yellow), process boxes (light blue), and outcome/diagnosis boxes (green for benign/carrier, red/orange for significant disease). Use bold black text, clear arrows with labels YES/NO or specific values. Layout and content: TOP ENTRY BOX (grey): "Child with suspected haemoglobinopathy" → subtext: "Pallor, jaundice, splenomegaly, haemolytic anaemia, family history, at-risk ethnicity (African, South Asian, Mediterranean, Middle Eastern), or newborn screening result" ↓ Arrow BLUE BOX: "STEP 1: Full Blood Count (FBC) + Blood Film" • Check: Hb level, MCV, MCH, RBC count • Blood film: target cells, sickle cells, nucleated RBCs, hypochromia, anisocytosis ↓ Arrow YELLOW DIAMOND: "Is MCV/MCH low? (MCV <70 fL, MCH <27 pg)" YES arrow → RIGHT BLUE BOX: "Exclude Iron Deficiency First" • Serum ferritin, iron studies • Treat if deficient, recheck FBC in 6–8 weeks → YELLOW DIAMOND: "Still low MCV after iron?" YES → Proceed to HPLC NO → GREEN BOX: "Iron Deficiency Anaemia — Treat" NO arrow (normal MCV) → Straight down Both paths converge ↓ BLUE BOX: "STEP 2: HPLC (High Performance Liquid Chromatography) + Haemoglobin Electrophoresis" • Gold standard test • Note: In neonates — HbF predominates, HbA appears by age 3–6 months • Report all Hb fractions: HbA, HbA2, HbF, HbS, HbC, HbE, HbH, HbBart's ↓ Arrow YELLOW DIAMOND: "What does the HPLC show?" Four branches fanning out below: BRANCH 1 (left-most): "HbS present" → YELLOW DIAMOND: "HbA also present?" YES (HbA present ~55%, HbS ~40%) → GREEN BOX: "Sickle Cell TRAIT (HbAS) — Carrier. Usually asymptomatic. Genetic counselling." NO (HbS >85–90%, no HbA) → YELLOW DIAMOND: "Any other Hb?" HbS only + HbF → RED BOX: "Sickle Cell Disease (HbSS) — Sickle Cell Anaemia" HbS + HbC → ORANGE BOX: "HbSC Disease — Moderate severity" HbS + HbF + small HbA → ORANGE BOX: "HbS-Beta+ Thalassaemia — Variable severity" HbS + HbF only (no HbA) → RED BOX: "HbS-Beta0 Thalassaemia — Severe, similar to SCD" BRANCH 2: "HbA2 elevated (>3.5%)" → YELLOW DIAMOND: "HbA present?" YES, Hb normal/mildly low → GREEN BOX: "Beta-Thalassaemia TRAIT (Minor) — Carrier. Asymptomatic/mild anaemia." NO HbA, high HbF (>90%) → RED BOX: "Beta-Thalassaemia MAJOR (Cooley's anaemia) — Severe, transfusion-dependent" Some HbA, raised HbF, moderate anaemia → ORANGE BOX: "Beta-Thalassaemia INTERMEDIA — Moderate, may not need transfusions" BRANCH 3: "Normal HPLC but low MCV/MCH, normal HbA2" → BLUE BOX: "Suspect ALPHA-Thalassaemia" → DNA/molecular testing or MCV <70 in family → YELLOW DIAMOND: "How many alpha genes deleted?" 1 gene → GREEN BOX: "Silent Carrier — Normal" 2 genes → GREEN BOX: "Alpha-Thal Trait — Mild microcytosis, asymptomatic" 3 genes (HbH on HPLC) → ORANGE BOX: "HbH Disease — Moderate haemolytic anaemia" 4 genes → RED BOX: "Hb Barts (Hydrops Fetalis) — Fatal without intervention" BRANCH 4 (right-most): "HbE or HbC present" → YELLOW DIAMOND: "Homozygous or compound?" HbEE or HbCC → ORANGE BOX: "Mild haemolytic anaemia — moderate disease" HbE/Beta-Thal → RED BOX: "HbE-Beta Thalassaemia — Severe (common in SE Asia)" Heterozygous HbE or HbC → GREEN BOX: "HbE or HbC Trait — Carrier, mild or no symptoms" BOTTOM SECTION — all paths lead down to: PURPLE BOX: "STEP 3: Confirmatory Tests if needed" • Molecular/DNA testing for alpha-thal or complex cases • Parental testing (to confirm inheritance pattern) • Osmotic fragility test • Reticulocyte count, bilirubin, LDH (haemolysis markers) • Bone marrow (only if diagnosis unclear) ↓ Arrow FINAL GREEN BOX: "STEP 4: Classify & Act" • Carrier/Trait → Genetic counselling, partner screening, reassurance • Mild disease (HbSC, HbH, Intermedia) → Monitor, folic acid, avoid triggers • Severe disease (HbSS, Beta-Thal Major, HbE/Beta-Thal) → Haematology referral, transfusion programme, hydroxyurea, iron chelation, consider HSCT Style: Clean white background, professional medical education style, pastel-colored boxes (light blue for process, yellow for decisions, green for benign outcomes, orange for moderate, red for severe), bold black labels, neat connecting arrows with clear YES/NO labels. Adequate spacing so all text is clearly readable.