Ligamentotaxis principal application everything related to it for 10 marks question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information to write a thorough 10-mark answer. Let me compile everything.
Ligamentotaxis — Principle and Applications
Definition and Principle
Ligamentotaxis (from Latin ligamentum = ligament + Greek taxis = arrangement/alignment) is the indirect reduction of fracture fragments by applying longitudinal traction/distraction across a joint or fracture site, using the intact soft tissue envelope — ligaments, joint capsule, periosteum, and annular/fascial attachments — as a biological traction harness to pull displaced fragments back toward anatomic position.
The concept was initially described by Vidal. The biomechanical basis is simple: when traction is applied across a zone of injury, the intact ligamentous and capsular structures become taut and exert a centripetal, corrective force on attached bony fragments, reducing displacement without direct surgical exposure of the fracture.
"Using the concept of ligamentotaxis initially described by Vidal, the structures of the soft tissue envelope surrounding the fracture are used to align fracture fragments by applying tension across the zone of injury." — Rockwood & Green's Fractures in Adults, 10th ed.
Mechanism
- Distraction is applied across the fracture site or adjacent joint
- Intact ligaments and joint capsule become taut
- Taut soft tissues exert a pulling force on bone fragments attached to them
- Displaced/comminuted fragments are drawn toward their anatomic position
- Fracture alignment is maintained as long as tension is sustained
- Simultaneously reduces soft tissue swelling and edema by reducing deformity
Key advantages of this mechanism:
- Minimally invasive — reduces fracture without exposing the zone of injury
- Preserves blood supply to comminuted fragments (no periosteal stripping)
- Reduces fracture hematoma disturbance, aiding biological healing
- Improves fracture visualization and aids disimpaction
Applications by Anatomical Region
1. Distal Radius Fractures
One of the most classic applications. An external fixator spanning the radiocarpal joint is applied with pins in the radius proximally and the 2nd metacarpal distally. Distraction tightens the extrinsic carpal ligaments, reducing and maintaining alignment of comminuted/osteoporotic distal radius fractures.
- The dorsal spanning (distraction) plate works on the same ligamentotaxis principle — it has been described as an "internal fixator" and is used for severely comminuted fractures, especially with osteoporotic bone
- Caution: Overdistraction must be avoided — excessive traction tightens carpal ligaments too much, reducing digital flexion and potentially contributing to CRPS (Complex Regional Pain Syndrome)
2. Tibial Pilon (Distal Tibial) Fractures
Highly comminuted pilon fractures are managed with dynamic distraction external fixation using ligamentotaxis:
- Pins placed in the distal tibial shaft and calcaneus
- A triangular or spanning frame across the ankle joint is constructed
- Distraction reduces the articular surface indirectly
- Allows early range of motion (ROM) while maintaining reduction
- Particularly indicated for severe comminution with compromised soft tissues
3. Tibial Plateau and Distal Femoral Fractures
Knee-bridging (spanning) external fixators are used as damage control constructs:
- Medial and lateral bars connect proximal and distal pins across the knee joint
- Manual distraction followed by ligamentotaxis reduction is achieved
- Reduces swelling dramatically by restoring limb length
- Patient can undergo resuscitation, imaging, and other procedures while reduction is maintained
- Definitive fixation (ORIF/MIPO) is carried out once soft tissues recover (skin wrinkling sign)
4. PIP Joint Fracture-Dislocations (Hand)
For unstable volar base fractures of the middle phalanx:
- Static external fixation achieves reduction via ligamentotaxis but causes joint stiffness
- Dynamic traction devices were therefore developed — a K-wire through the middle phalanx shaft is connected to a hinge construct centered at the PIP joint axis
- Traction is maintained continuously to hold ligamentotaxis reduction, while active/passive motion is encouraged
- Devices include: dynamic distraction external fixation, force-couple constructs, wire-spring devices, and commercial hinged fixators (e.g., Compass PIP Hinge)
5. Thoracolumbar Spine Burst Fractures
Ligamentotaxis plays an important role in indirect spinal canal decompression:
- Pedicle screw-rod constructs are applied posteriorly across the injured level
- Rods are contoured to correct kyphosis; distraction is applied across adjacent pedicle screws
- This restores vertebral body height and simultaneously tensions the posterior longitudinal ligament (PLL) and annulus fibrosus
- The taut PLL/annulus pulls retropulsed bony fragments anteriorly, decompressing the spinal canal
- Ligamentotaxis can achieve up to 50% canal decompression
- Limitation: Ineffective if annular attachments are disrupted (e.g., fragment rotated 180°, posterior cortex facing anteriorly) or in subacute/chronic fractures where ligamentous laxity develops
6. Cervical Spine Fractures/Dislocations
Skull-based traction (Gardner-Wells tongs, halo) achieves ligamentotaxis at the cervical spine:
- Progressive weight application through skull causes distraction at the injury site
- Realignment of fracture fragments and dislocated facets occurs through ligamentotaxis
- Also provides pre-operative partial decompression of the spinal canal
7. Complex Femoral and Long Bone Fractures
The femoral distractor and universal distractor are intraoperative tools that apply distraction:
- Pins placed proximal and distal to the fracture
- Distraction restores length, corrects angulation and rotation via ligamentotaxis
- Facilitates intramedullary nailing by achieving and maintaining reduction
Devices Used to Apply Ligamentotaxis
| Device | Application |
|---|---|
| Spanning external fixator | Distal radius, tibial pilon, knee, ankle |
| Dorsal distraction plate | Comminuted distal radius |
| Femoral/Universal distractor | Intraoperative reduction aid |
| Dynamic distraction fixator | PIP joint fractures (with motion) |
| Skull traction (Gardner-Wells / Halo) | Cervical spine |
| Posterior pedicle screw-rod system | Thoracolumbar burst fractures |
| Fracture table traction | Femoral neck, shaft fractures |
Advantages of Ligamentotaxis
- Minimally invasive — avoids surgical dissection of the fracture zone
- Preserves periosteal blood supply to fracture fragments
- Reduces soft tissue swelling and edema quickly
- Enables damage control — rapid stabilization in polytrauma patients
- Facilitates indirect reduction of multiple comminuted fragments simultaneously
- Provides canal decompression in spine fractures without direct surgery
Limitations
- Requires intact soft tissue envelope — ineffective if ligaments/capsule are ruptured
- Timing-sensitive — delay of more than a few days leads to inability to disimpact metaphyseal fragments (fracture begins to "set")
- Risk of overdistraction — CRPS, joint stiffness, neurovascular injury
- Incomplete reduction of large/rotated fragments may still require direct open reduction
- Spinal ligamentotaxis: ineffective for fragments that have rotated 180° or where annular attachments are disrupted
Summary: Ligamentotaxis is a foundational orthopedic principle that harnesses the tensile strength of the intact soft tissue envelope to reduce and maintain fracture alignment through distraction. It is applied across the spectrum of orthopedic trauma — from distal radius and pilon fractures to PIP joint injuries, knee-bridging damage control fixation, and thoracolumbar spinal burst fractures — using external fixators, spanning plates, distractors, traction devices, and pedicle screw constructs.
Sources: Rockwood & Green's Fractures in Adults, 10th ed. (2025); Miller's Review of Orthopaedics, 9th ed.
Why no images
Loading Image
Loading Image
Searching Images
ligamentotaxis external fixator distal radius fracture reduction
Loading Image
Here is the complete answer with images:
Ligamentotaxis — Principle and Applications
Definition and Principle
Ligamentotaxis (Latin ligamentum + Greek taxis = arrangement) is the indirect reduction of fracture fragments by applying longitudinal traction/distraction across a joint or fracture site, using the intact soft tissue envelope — ligaments, joint capsule, periosteum, annular/fascial attachments — as a biological traction harness to pull displaced fragments back toward anatomic position.
First described by Vidal, the concept is:
"The structures of the soft tissue envelope surrounding the fracture are used to align fracture fragments by applying tension across the zone of injury." — Rockwood & Green's Fractures in Adults, 10th ed.
Mechanism
- Distraction applied across fracture site or adjacent joint
- Intact ligaments and joint capsule become taut
- Taut soft tissues exert a corrective pulling force on attached bony fragments
- Comminuted fragments drawn toward anatomic position
- Alignment maintained as long as tension is sustained
- Simultaneously reduces soft tissue swelling and edema
Applications by Region
1. Distal Radius Fractures
The most classic application. An external fixator with pins in the radius (proximal) and 2nd metacarpal (distal) distracts the radiocarpal joint, tightening extrinsic carpal ligaments to reduce comminuted/osteoporotic fractures.
X-ray: Bridging external fixator for distal radius fracture — ligamentotaxis in action (AP and lateral views)

The dorsal spanning (distraction) plate works on the same principle — described as an "internal fixator," used for severely comminuted/osteoporotic fractures.
Caution: Overdistraction overtightens carpal ligaments → digital stiffness and risk of CRPS.
2. Tibial Pilon & Periarticular Fractures — Damage Control External Fixation
Spanning external fixators are applied as damage control constructs for tibial plateau, distal femoral, and pilon fractures:
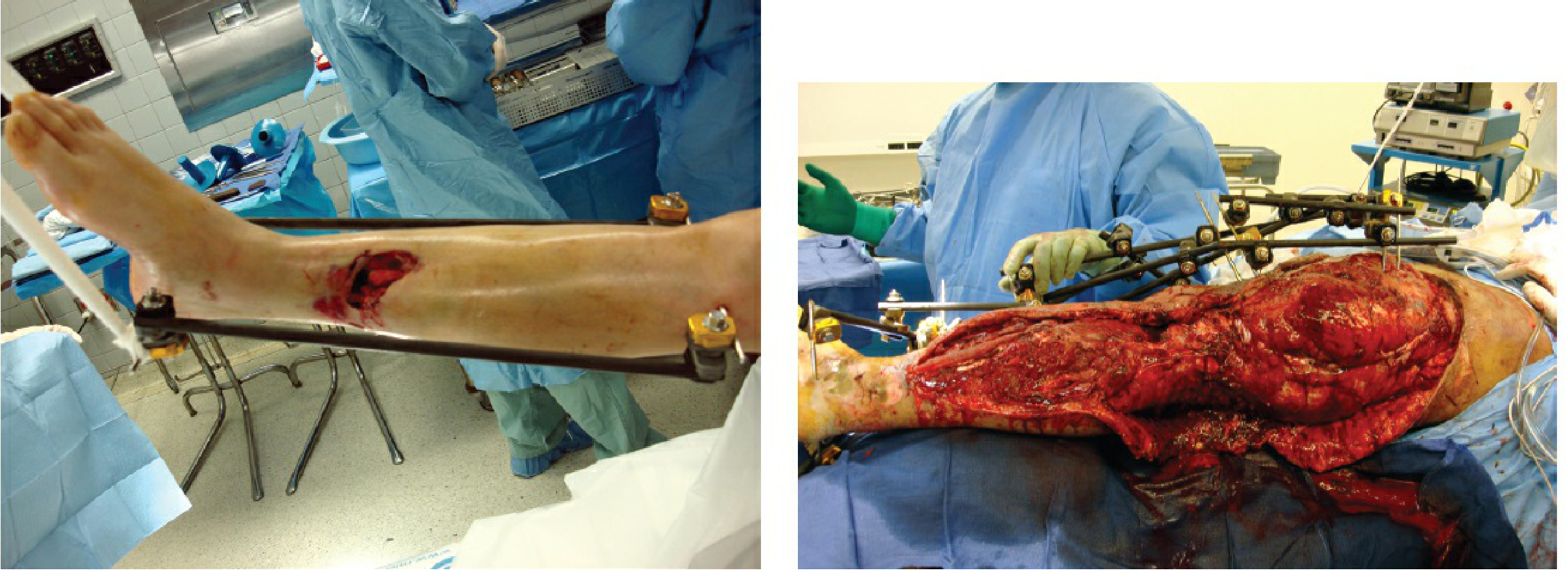
- Pins proximal and distal to the fracture zone; manual distraction → ligamentotaxis reduction
- Reduces swelling dramatically by restoring limb alignment
- Patient undergoes resuscitation/other procedures while reduction is maintained
- Definitive ORIF performed once soft tissues recover (skin wrinkling sign)
3. PIP Joint Fracture-Dislocations (Hand)
For unstable volar base fractures of the middle phalanx, dynamic traction devices allow simultaneous ligamentotaxis reduction AND joint motion:
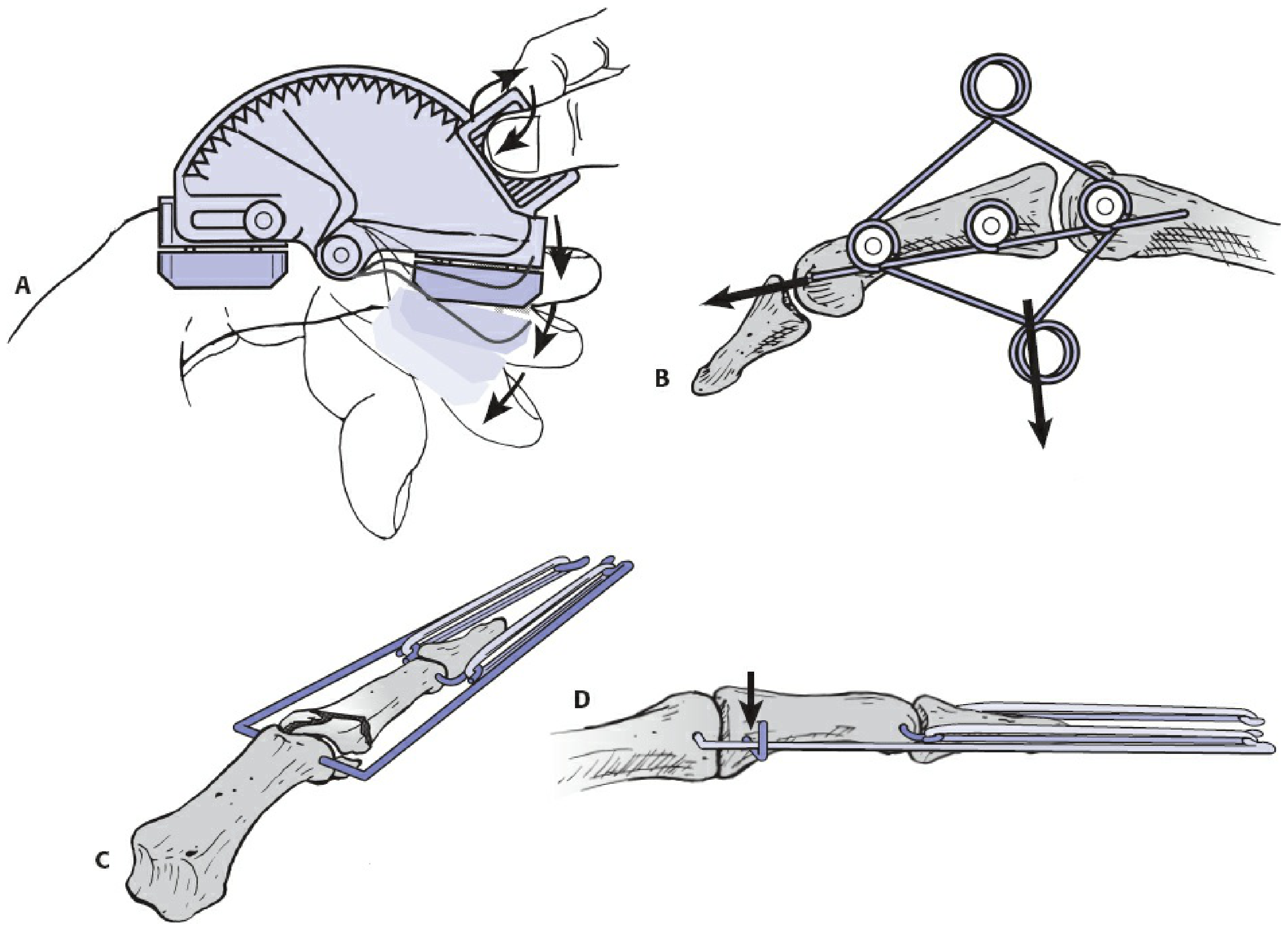
- Static external fixation achieves ligamentotaxis but causes stiffness
- Dynamic devices maintain traction continuously while permitting active/passive motion
- Types: hinged distraction fixators (Compass PIP Hinge), wire-spring, force-couple constructs
4. Thoracolumbar Spine Burst Fractures
Posterior pedicle screw-rod constructs achieve indirect spinal canal decompression via ligamentotaxis:
- Rods contoured to correct kyphosis; distraction applied across pedicle screws adjacent to injury
- Tensions the posterior longitudinal ligament (PLL) and annulus fibrosus
- Taut PLL/annulus pulls retropulsed fragments anteriorly → canal decompression
- Can achieve up to 50% canal decompression
- Limitation: Ineffective if annular attachments are disrupted (fragment rotated 180°)
5. Cervical Spine — Skull Traction
Gardner-Wells tongs / halo traction:
- Progressive weight causes distraction at injury site
- Realigns fracture fragments and dislocated facets through ligamentotaxis
- Provides pre-operative partial spinal canal decompression
Devices Used
| Device | Site |
|---|---|
| Spanning external fixator | Distal radius, pilon, knee, ankle |
| Dorsal distraction plate | Comminuted distal radius |
| Dynamic distraction fixator | PIP joint (with motion) |
| Femoral/Universal distractor | Intraoperative long bone reduction |
| Posterior pedicle screw-rod | Thoracolumbar burst fractures |
| Skull traction (Gardner-Wells/halo) | Cervical spine |
| Fracture table | Femoral neck/shaft |
Advantages
- Minimally invasive — avoids surgical exposure of fracture zone
- Preserves periosteal blood supply to comminuted fragments
- Rapidly reduces soft tissue swelling
- Enables damage control stabilization in polytrauma
- Simultaneously reduces multiple comminuted fragments
- Allows indirect spinal canal decompression
Limitations
- Requires intact soft tissue envelope — fails if ligaments/capsule are ruptured
- Time-sensitive — delay >few days → fragments begin to "set," disimpaction impossible
- Risk of overdistraction → stiffness, CRPS, neurovascular injury
- Large/rotated fragments may still need direct open reduction
- Spinal ligamentotaxis: ineffective for 180°-rotated retropulsed fragments
Sources: Rockwood & Green's Fractures in Adults, 10th ed. (2025); Miller's Review of Orthopaedics, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.