photodynamic therapy in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
"photodynamic therapy" AND "head and neck" AND "ENT"
"photodynamic therapy" AND "laryngeal" OR "oral cavity" AND carcinoma
"photodynamic therapy" AND "photosensitizer" AND "cancer"
"photodynamic therapy" AND "head neck cancer" AND photosensitizer
"photodynamic therapy" AND "squamous cell carcinoma" AND "larynx" OR "oral"
"photodynamic therapy" AND "recurrent respiratory papillomatosis" OR "laryngeal papilloma"
photodynamic therapy ENT head neck recent advances 2024 2025 nanoparticle mTHPC temoporfin second generation photosensitizer
PHOTODYNAMIC THERAPY (PDT) IN ENT - 50 MARKS
1. INTRODUCTION AND HISTORICAL BACKGROUND
- 1900: Von Tappeiner and Jesionek first described photosensitization
- 1972: Discovery of tumour-localizing properties of haematoporphyrins
- 1978: Dougherty introduced clinical PDT using haematoporphyrin derivatives
- 1986: FDA approved porfimer sodium (Photofrin) - first photosensitizer
- 1999: FDA approved ALA (Levulan) for actinic keratoses
- 2000s onward: Second- and third-generation photosensitizers developed
2. DEFINITION AND BASIC CONCEPT
"PDT is a subset of photochemotherapy where, in addition to an administered drug and the application of light, oxygen is required to complete the process."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1, p. 632
┌─────────────────────────────────────────────────┐
│ │
│ PHOTOSENSITIZER + LIGHT + OXYGEN = PDT EFFECT│
│ │
│ Remove ANY ONE component → No PDT effect │
│ │
└─────────────────────────────────────────────────┘
3. MECHANISM OF ACTION (PHOTOCHEMISTRY)
Step-by-Step Mechanism
FLOWCHART 1: MECHANISM OF PDT
Photosensitizer administered (IV / topical)
↓
Selective accumulation in tumour tissue
(Tumour retains PS longer than normal tissue)
↓
Drug-light interval (3–96 hours)
↓
Laser/light of specific wavelength applied
↓
PS absorbs photons → Excited Singlet State (S1)
↓
Intersystem crossing → Excited Triplet State (T1)
↓
┌──────────────┤
│ │
TYPE I Rxn TYPE II Rxn (dominant)
(radical) ↓
│ Triplet PS + Ground state O₂
│ ↓
│ SINGLET OXYGEN (¹O₂)
↓ ↓
Superoxide, Oxidative damage to:
Hydroxyl - Cell membranes
radicals - Mitochondria
- Nuclear membranes
↓
APOPTOSIS + NECROSIS
+ VASCULAR COLLAPSE
Key Photochemical Reactions
| Reaction Type | Mechanism | End Product |
|---|---|---|
| Type I | PS reacts directly with substrate | Radical species (H₂O₂, O₂⁻•, •OH) |
| Type II | PS energy transferred to O₂ | Singlet oxygen (¹O₂) - PRIMARY pathway |
4. PDT MECHANISM DIAGRAM
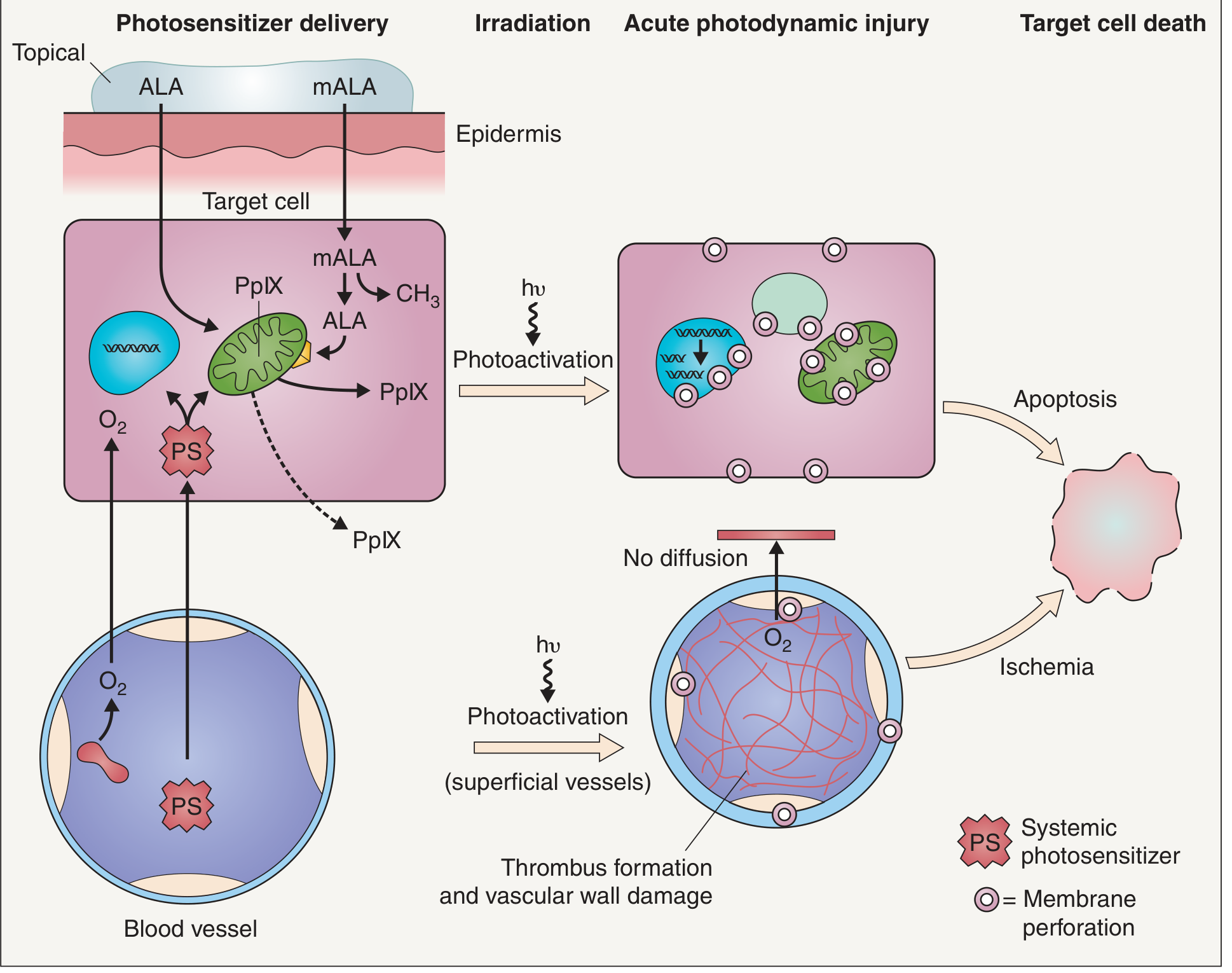
- Top pathway (direct cellular injury): Topical ALA/mALA diffuses into target epithelial cells → converted to Protoporphyrin IX (PpIX) in mitochondria → photoactivation (hν) → membrane perforation → apoptosis
- Bottom pathway (vascular injury): Systemic photosensitizer arrives via bloodstream into endothelial cells → photoactivation → thrombus formation and vascular wall damage → O₂ delivery ceases → ischemic necrosis
- Net result: Both direct apoptosis and ischemic necrosis cause irreversible target cell death
5. ALA/PpIX BIOSYNTHETIC PATHWAY
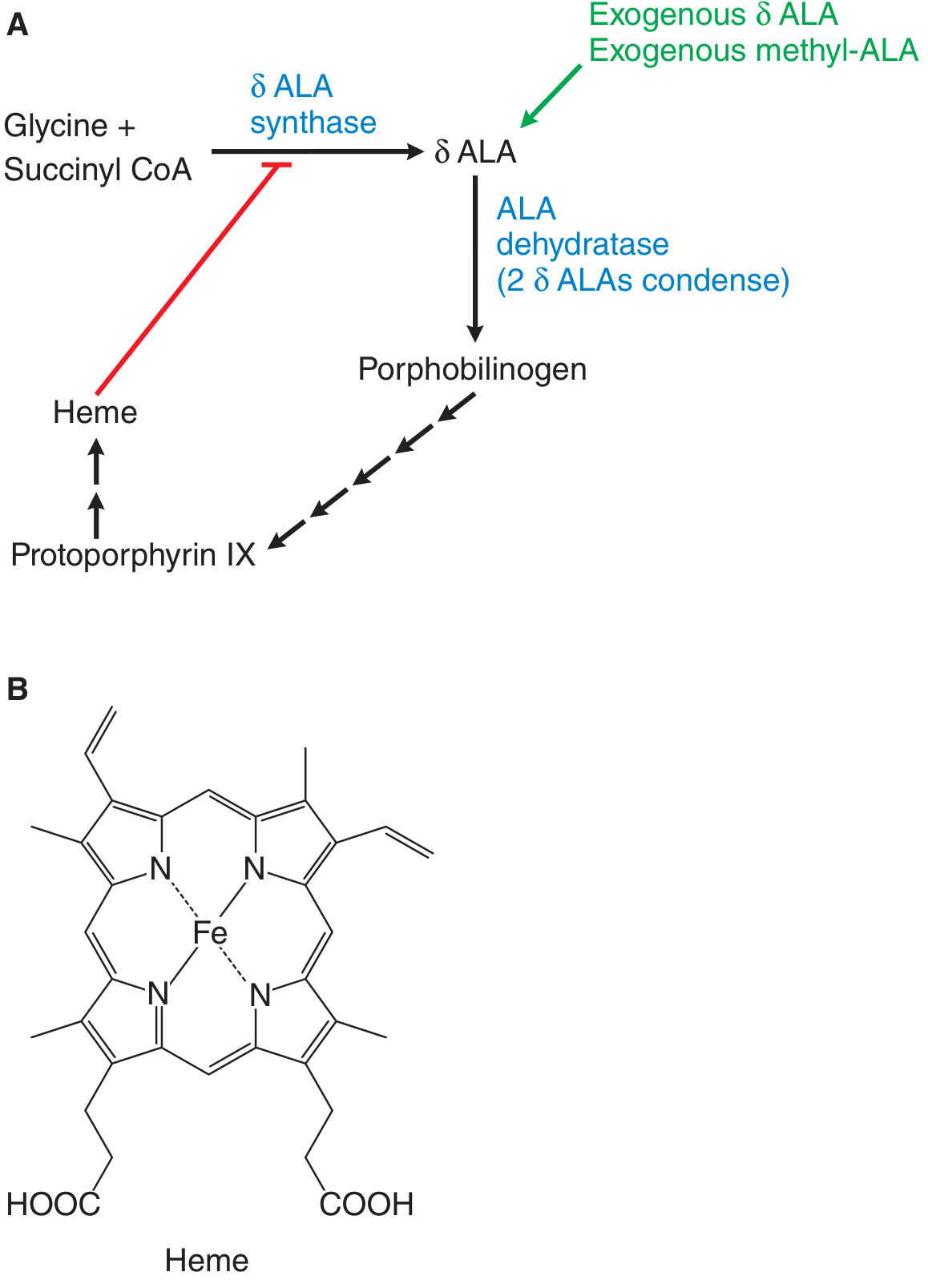
FLOWCHART 2: ALA BIOSYNTHETIC PATHWAY IN PDT
Normal pathway:
Glycine + Succinyl CoA → [δ-ALA synthase] → δ-ALA
↑
Heme (negative feedback)
PDT intervention (exogenous ALA bypasses this):
Exogenous δ-ALA (topical/IV) → bypasses feedback →
→ Porphobilinogen
→ (multiple steps)
→ Uroporphyrinogen III
→ Coproporphyrinogen III
→ Protoporphyrin IX (PpIX) ← ACTIVE PHOTOSENSITIZER
→ Heme (if ferrochelatase adds Fe²⁺)
In tumour cells: Ferrochelatase activity is REDUCED
→ PpIX accumulates preferentially in tumour tissue
→ Selective photosensitization
6. PHOTOSENSITIZERS
Generation Classification
FLOWCHART 3: GENERATIONS OF PHOTOSENSITIZERS
┌─────────────────────────────────────────────────────────────┐
│ PHOTOSENSITIZER GENERATIONS │
│ │
│ 1st GENERATION 2nd GENERATION 3rd GENERATION │
│ (1970s-1980s) (1990s-2000s) (2000s-present) │
│ │
│ • Haematoporphyrin • mTHPC/Foscan • Nanoparticle │
│ derivative (HpD) • Verteporfin conjugates │
│ • Porfimer sodium • ALA/5-ALA • Antibody- │
│ (Photofrin) • mALA targeted PS │
│ • DHE • Temoporfin • EGFR-targeted │
│ • Chlorins, • Liposomal PS │
│ Disadvantages: Phthalocyanines • Photoimmuno- │
│ - Long photosensitivity Advantages: therapy │
│ - Skin reactions - Shorter DLI │
│ - Mixed composition - Better tissue │
│ - Short wavelength penetration │
│ (630 nm) - Less │
│ - Less selective photosensitivity │
│ - Higher │
│ selectivity │
└─────────────────────────────────────────────────────────────┘
Commonly Used Photosensitizers in ENT
| Drug | Generation | Route | Dose | Drug-Light Interval | Light Wavelength |
|---|---|---|---|---|---|
| Porfimer sodium (Photofrin) | 1st | IV | 2 mg/kg | 40–50 hrs | 630 nm |
| DHE (Dihematoporphyrin ether) | 1st | IV | 4.25 mg/kg | 48–72 hrs | 630 nm |
| mTHPC / Foscan (Temoporfin) | 2nd | IV | 0.15 mg/kg | 96 hrs | 652 nm |
| ALA (Levulan, 5-ALA) | 2nd prodrug | Topical | 10-20% | 1-18 hrs | 635 nm |
| mALA (Metvix) | 2nd prodrug | Topical | 16.8% | 3 hrs | 630 nm |
| Verteporfin (Visudyne) | 2nd | IV | 6 mg/m² | 15 min | 689 nm |
7. PROCEDURE / TECHNIQUE
Steps of PDT in Head and Neck
FLOWCHART 4: PROCEDURE OF PDT
STEP 1: PATIENT SELECTION & ASSESSMENT
- Clinical staging of tumour
- Determine curative/palliative intent
- Assess tumour depth (PDT best for <1 cm depth)
- Rule out contraindications (porphyria, photosensitivity disorders)
↓
STEP 2: PHOTOSENSITIZER ADMINISTRATION
- For head/neck cancers: IV infusion (porfimer sodium or mTHPC)
- For superficial lesions: topical ALA or mALA
- Patient kept in dim light / photosensitivity precautions
↓
STEP 3: DRUG-LIGHT INTERVAL (DLI)
- Allows PS to accumulate selectively in tumour
- Duration varies: 15 min (verteporfin) to 96 hrs (mTHPC)
- Normal tissue clears PS faster than tumour tissue
↓
STEP 4: LIGHT DELIVERY
- Light source: Argon pump-dye laser, diode laser, LED
- Wavelength: matched to PS absorption peak
- Delivery: via rigid/flexible endoscope, optical fibres, surface illumination
- Dose (fluence): 50–200 J/cm²
- For hollow organs (oesophagus, larynx): cylindrical diffuser fibre
- For surface lesions: flat/microlens fibres
↓
STEP 5: TISSUE RESPONSE
- Immediate: vascular stasis, tumour oedema
- 24–72 hrs: inflammatory response, necrosis
- 1–4 weeks: tissue sloughing, healing
↓
STEP 6: POST-TREATMENT CARE
- Photosensitivity precautions: avoid sunlight 4–6 weeks (porfimer)
or 2 weeks (mTHPC/Foscan)
- Wound care, debridement if needed
- Endoscopic surveillance at 4–6 weeks
- Assessment of response: complete vs. partial
↓
STEP 7: REPEAT IF NEEDED
(PDT can be repeated unlike radiotherapy - major advantage)
8. APPLICATIONS IN ENT / HEAD AND NECK SURGERY
8.1 Oral Cavity and Oropharynx
"PDT has a potential role in the treatment of widespread premalignant and superficial oral carcinoma." - Cummings Otolaryngology, p. 1675
- Premalignant lesions: Leukoplakia, erythroplakia - excellent results with ALA-PDT
- Oral cavity SCC: Best results reported in oral cavity and oropharynx
- Karakullukcu et al. (170 patients with early-stage oral cavity/oropharynx neoplasms): 90% response rate, 70% complete cure rate
- Photofrin activated by 620 nm light; produces oxidizing free radicals via vascular disruption → tumour necrosis
8.2 Laryngeal Carcinoma
- PDT particularly suitable for early laryngeal cancers (T1, T2) due to:
- Excellent endoscopic access
- Organ preservation (voice preservation)
- Repeatable without radiation dose limits
- Biel treated 25 patients with early laryngeal SCC → complete response in all patients, including 17 who had previously failed radiotherapy
- Biel's meta-analysis (217 patients, multiple centres):
- Complete response: 194 (89%)
- Partial response: 23 (10.6%)
- No failure to respond: 0%
8.3 Nasopharyngeal Carcinoma
- Lofgren et al.: PDT in 5 patients with circumscribed nasopharyngeal carcinoma
- Drug activated with laser light under topical anaesthesia
- After 4 years: 3/5 patients had no evidence of disease
- Particularly useful for residual/recurrent disease after radiotherapy
8.4 Recurrent Respiratory Papillomatosis (RRP / Laryngeal Papillomatosis)
"PDT is based on the transfer of energy to a photosensitive drug such as dihematoporphyrin ether (DHE), which has a tendency to concentrate within papillomas." - Cummings Otolaryngology, RRP chapter
- IV DHE: 4.25 mg/kg before photoactivation
- Argon pump-dye laser for photoactivation
- Shows small but statistically significant decrease in RRP growth rate
- Best in patients with severe disease
- Parallel-arm RCT (23 patients, aged 4–60 years)
- Improvement in laryngeal disease noted
- However: relapse occurred over 3–5 years
- Poorly tolerated by ~25% of patients
- NOT FDA-approved in the USA
8.5 Oesophageal Cancer (relevant to ENT surgeons)
- Porfimer sodium PDT vs. Nd:YAG laser ablation (Phase II RCT, 218 patients):
- Equivalent improvement in dysphagia
- Fewer perforations with PDT (1% vs. 7%, p<0.05)
- Overholt & Panjehpour (55 patients with Barrett's oesophagus with dysplasia):
- Good response at 6 months
- 43/55 patients with high-grade dysplasia/adenocarcinoma showed endoscopic ablation
- Complication: oesophageal stricture in 53%
8.6 Sinonasal Tumours
- Inverted papilloma of the sinonasal cavity has been targeted with PDT
- Dilkes et al. used mTHPC and ALA for squamous carcinoma at multiple head and neck sites (mid-1990s)
- In nearly all cases, a visible response to PDT was identified
- Complications: local pain at photosensitizer injection site, post-treatment skin photosensitivity
8.7 Chronic Rhinosinusitis (CRS) / Biofilm
"PDT has been shown to effectively treat bacteria, fungi, and biofilms." - Cummings, CRS chapter
- Two studies examining PDT on Staphylococcus and Pseudomonas biofilms showed 99.9% reduction in bacteria after single exposure
- No human studies yet in CRS
- Currently: insufficient evidence, not recommended in routine CRS management
9. LIGHT SOURCES USED IN PDT
| Light Source | Wavelength | Application |
|---|---|---|
| Argon pump-dye laser | Tunable (630 nm for PDT) | Classic PDT, laryngeal |
| KTP laser | 532 nm | Superficial vascular lesions |
| Diode laser | 630–690 nm | Most common in modern PDT |
| LED (light-emitting diode) | Variable | Topical PDT, dermatology |
| Broadband (filtered lamps) | Visible spectrum | Dermatology PDT |
| Nd:YAG laser | 1064 nm | Comparison arm in RCTs |
| Daylight | Visible spectrum | D-PDT for actinic keratoses |
- For ENT/hollow organs: light delivered via optical fibres through flexible endoscopes
- Cylindrical diffuser fibres used for tubular organs (trachea, oesophagus, larynx)
- Surface illumination for oral cavity, skin
10. ADVANTAGES AND DISADVANTAGES
┌──────────────────────────────────┬─────────────────────────────────┐
│ ADVANTAGES │ DISADVANTAGES │
├──────────────────────────────────┼─────────────────────────────────┤
│ • Selective tumour destruction │ • Prolonged skin photosensitivity│
│ • Organ/function preservation │ (4-6 weeks with porfimer) │
│ • Can be repeated (unlike XRT) │ • Limited depth of penetration │
│ • Not affected by prior XRT, │ (<5-10 mm tissue depth) │
│ chemotherapy, or surgery │ • Not for bulky/deep tumours │
│ • Minimal systemic toxicity │ • Requires laser equipment │
│ • Good cosmetic outcome │ • Expensive │
│ • Outpatient procedure possible │ • Stricture formation │
│ (for topical lesions) │ (oesophageal) │
│ • Multiple treatments possible │ • Tumour not absolutely specific│
│ • Useful for field cancerization │ (normal tissue necrosis also) │
│ • Favourable functional results │ • Limited to endoscopically │
│ • Potential for palliation │ accessible tumours │
│ AND cure │ • Response rates ~50% for RRP │
└──────────────────────────────────┴─────────────────────────────────┘
11. CONTRAINDICATIONS
- Porphyria (cutanea tarda, variegate porphyria)
- Known hypersensitivity to photosensitizer
- Existing photosensitivity disorders
- Tumour invasion of major blood vessels (risk of fatal haemorrhage after necrosis)
- Tumour eroding into trachea (risk of tracheo-oesophageal fistula)
- Patients unable to protect themselves from light exposure
- Deep/bulky tumours (>1 cm depth - inadequate light penetration)
12. COMPLICATIONS
| Complication | Frequency | Management |
|---|---|---|
| Skin photosensitivity | Very common (all systemic PS) | Strict light avoidance 4-6 weeks |
| Skin erythema/blistering | Common | Topical steroids, wound care |
| Oesophageal stricture | 53% (PDT for Barrett's) | Dilatation |
| Mucosal oedema/pain | Common | Analgesics, steroids |
| Tissue necrosis (non-specific) | Documented | Not absolutely tumour-specific |
| Local pain at injection site | Common | Analgesics |
| Ocular discomfort | Common | Dark glasses |
13. PDT vs PUVA THERAPY (Comparison Table)
| Feature | PDT | PUVA Therapy |
|---|---|---|
| Routes of PS administration | Topical / Systemic (IV) | Topical / Systemic (PO) |
| Photosensitizer | ALA or mALA (prodrugs) | 8-methoxypsoralen |
| Active form | Protoporphyrin IX (PpIX) | 8-methoxypsoralen |
| PS activation | Visible light | Ultraviolet A |
| Photochemical reaction | Type II: converts O₂ to ¹O₂ | Type I: covalent adducts with DNA |
| Oxygen dependence | Yes (obligatory) | No |
| Cancer relationship | Treats keratinocyte carcinomas | Carcinogenic (long-term) |
| Long-term safety | Generally safe, treats photoaging | Skin cancer, photoaging |
14. OVERALL MANAGEMENT FLOWCHART FOR PDT IN HEAD AND NECK
FLOWCHART 5: PATIENT SELECTION AND MANAGEMENT FOR PDT IN H&N
Suspected Head & Neck Tumour / Premalignant Lesion
↓
Clinical Assessment + Imaging + Biopsy
↓
┌───────────────┴──────────────────┐
↓ ↓
Superficial / Early Stage Advanced / Deep Tumour
T1/T2, <5 mm depth T3/T4, >1 cm depth
↓ ↓
PDT SUITABLE PDT NOT PRIMARY CHOICE
↓ (Consider surgery/chemo-XRT)
Select Photosensitizer: However PDT may be used:
- Oral/OP: Porfimer, mTHPC - Palliatively
- RRP: DHE, mTHPC - As adjuvant
- Superficial: ALA/mALA - For recurrence
↓
Administer Photosensitizer
(IV infusion or topical)
↓
DRUG-LIGHT INTERVAL
(48–96 hrs for systemic; 1–4 hrs for ALA)
↓
Light Delivery via Endoscope/Fibre
- Appropriate wavelength
- Measured fluence (50–200 J/cm²)
↓
┌──────────────────────────────────┐
│ PHOTOSENSITIVITY PRECAUTIONS │
│ (4–6 weeks for porfimer; │
│ 2 weeks for mTHPC) │
└──────────────────────────────────┘
↓
Follow-up at 4–6 weeks
↓
┌──────────────────┬───────────────────┐
↓ ↓ ↓
Complete Partial No Response
Response Response ↓
↓ ↓ Consider alternative
Surveillance Repeat PDT (Surgery/XRT)
(advantage:
repeatable)
15. SPECIFIC CONSIDERATIONS BY TEXTBOOK AUTHORS
Scott-Brown's (Otorhinolaryngology H&N Surgery Vol 1, Chapter on Lasers and PDT):
- Emphasises the triad requirement: drug + light + oxygen
- The drug-light interval is 3–96 hours for head and neck PDT
- Tumour targeting arises from: (1) selective uptake by tumour due to PS structure and (2) accurate application of appropriate wavelength
- Skin phototoxicity and limited tissue penetration are the current PDT shortcomings
- Conclusion: "PDT has a significant place in the future management of head and neck cancer"
- Key trials: Karakullukcu (170 patients, 90% response), Biel (25 laryngeal, 100% response), Lofgren (5 NPC, 3/5 disease-free at 4 years)
Cummings Otolaryngology:
- Oral SCC: Photofrin + 620 nm light → oxidizing free radicals → vascular disruption → tumour necrosis
- Advantage: potential for multiple treatments with favourable functional and cosmetic results
- Disadvantage: prolonged skin photosensitivity up to 6 weeks
- Newer generation PS may be more specific and result in less photosensitization
- RRP: DHE (4.25 mg/kg) → statistically significant decrease in RRP growth, especially severe disease
Goodman & Gilman's Pharmacological Basis of Therapeutics:
- ALA and mALA are prodrugs converted to PpIX within living cells
- PpIX in presence of specific wavelengths and O₂ → reactive oxygen species → oxidize cell membranes, proteins, and mitochondrial structures → apoptosis
- Epidermis, sebaceous glands, and neoplastic cells accumulate more porphyrin → preferential targeting
- Half-life of accumulated porphyrins: ~30 hours → photosensitivity precautions for at least 48 hours after treatment
16. RECENT ADVANCES (2021-2026)
FLOWCHART 6: EVOLUTION OF PDT - RECENT ADVANCES
Classical PDT (1st Gen PS)
↓
2nd Gen PS (mTHPC, ALA, Verteporfin)
↓
3rd Gen / Targeted PDT
↓
┌─────────────────────────────────────────────┐
│ RECENT ADVANCES (2021-2026) │
├─────────────────────────────────────────────┤
│ 1. NANOPARTICLE-ENHANCED PDT │
│ • Liposomal drug delivery (2026) │
│ • Gold nanoparticle PS conjugates │
│ • Polymeric nanoparticles │
│ Advantages: deeper penetration, │
│ improved selectivity, reduced side effects│
│ │
│ 2. EGFR-TARGETED PDT (Ulfo et al. 2022) │
│ • Anti-EGFR antibody conjugated to PS │
│ • Highly relevant in HNSCC (EGFR+) │
│ • PMID: 35213974 │
│ │
│ 3. IMMUNOTHERAPY COMBINATION │
│ • PDT + PD-L1 checkpoint blockade │
│ • PDT-induced immunogenic cell death │
│ • Activates anti-tumour immunity │
│ • Synergistic with anti-PD-1/PD-L1 │
│ │
│ 4. DAYLIGHT PDT (D-PDT) │
│ • For actinic keratoses │
│ • Natural daylight as light source │
│ • Improved patient comfort vs pain │
│ │
│ 5. ANTIMICROBIAL PDT (aPDT) │
│ • Staphylococcus aureus biofilm (CRS) │
│ • 99.9% bacterial reduction in vitro │
│ • Pseudomonas aeruginosa biofilm │
│ • Methylene blue as PS │
│ │
│ 6. PHOTODYNAMIC DIAGNOSIS (PDD) │
│ • ALA-induced PpIX for tumour mapping │
│ • "Blue light cystoscopy" model │
│ • Application to laryngeal early lesions │
│ │
│ 7. MACHINE LEARNING INTEGRATION │
│ • AI-based dosimetry optimization │
│ • Predicting tumour response │
│ • Personalised light dosing │
│ │
│ 8. PDT + SURGERY COMBINATION for RRP │
│ • Pan Y et al., Am J Otolaryngol 2024 │
│ • Surgery + PDT vs surgery alone │
│ • Improved outcomes, reduced recurrence │
│ • PMID: 39142078 │
└─────────────────────────────────────────────┘
- Kolarikova et al., Med Res Rev 2023 - "Photodynamic therapy: Innovative approaches for antibacterial and anticancer treatments" - comprehensive review of antibacterial and anticancer PDT (PMID: 36757198)
- Aebisher et al., Int J Mol Sci 2024 - "Photodynamic Therapy: Past, Current, and Future" - latest state-of-the-art review (PMID: 39457108)
- Balakirski et al., J Dtsch Dermatol 2024 - "PDT in dermatology: established and new indications" (PMID: 39226531)
- Pan Y et al., Am J Otolaryngol 2024 - Surgery + PDT for RRP - improved outcomes (PMID: 39142078)
- Nano-enhanced PDT for HNSCC: Nanoplatform-Enhanced PDT - systematic bibliometric analysis [PMC 2025]
17. PDT IN CONTEXT OF RGUHS SYLLABUS
RGUHS Important Points to Remember:
- Three essentials of PDT: Photosensitizer + Light + Oxygen
- Primary mechanism: Type II photochemical reaction → Singlet oxygen (¹O₂)
- Best results in ENT: Early laryngeal and oral cavity SCC
- PDT for RRP: DHE (4.25 mg/kg) via argon pump-dye laser
- Photofrin (Porfimer sodium): First approved PS, 630 nm, 4-6 weeks photosensitivity
- mTHPC (Temoporfin/Foscan): Second generation, 652 nm, less photosensitivity
- ALA (5-ALA): Prodrug → PpIX via heme biosynthesis; used topically
- Biel's statistics: 89% complete response in 217 patients with H&N SCC
- Karakullukcu: 90% response rate, 70% cure in oral/oropharynx PDT
- Key advantage: PDT can be repeated unlike radiotherapy
18. SUMMARY TABLE
| Parameter | Detail |
|---|---|
| Definition | PS + Light + O₂ → Singlet oxygen → Selective tumour destruction |
| Primary photochemical reaction | Type II (dominant) |
| Active species | Singlet oxygen (¹O₂) |
| 1st gen PS (ENT) | Porfimer sodium (Photofrin), DHE |
| 2nd gen PS (ENT) | mTHPC (Foscan), ALA, mALA |
| Light sources | Argon pump-dye laser, diode laser, LED |
| Wavelength range | 630–695 nm (for standard ENT PS) |
| Drug-light interval | 3–96 hours (PS-dependent) |
| Photosensitivity duration | 2–6 weeks (systemic PS) |
| Best indication in ENT | Early laryngeal/oral SCC; RRP |
| Tissue penetration depth | 5–10 mm (major limitation) |
| Complete response in early H&N SCC | ~89% (Biel meta-analysis) |
| Recent advance | Nanoparticle PDT; EGFR-targeted PDT; PDT + immunotherapy |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1 & 2 (9781138094611, 9781138094634) - Chapters on Lasers & PDT, RRP
- Cummings Otolaryngology Head and Neck Surgery (9780323612173) - Chapters on Oral Cavity, Larynx, CRS, RRP
- Goodman & Gilman's Pharmacological Basis of Therapeutics (9781264258079) - Chapter 75
- Dermatology 2-Volume Set 5e (Griffiths, 9780702082252) - Chapter 135: PDT
- Fitzpatrick's Dermatology (9780071837781) - PDT chapters
- Kolarikova et al., Med Res Rev 2023 (PMID: 36757198)
- Aebisher et al., Int J Mol Sci 2024 (PMID: 39457108)
- Pan Y et al., Am J Otolaryngol 2024 (PMID: 39142078)