Q. Management of Acute Vertigo in a 37 year old male in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
acute vertigo management flowchart diagnosis BPPV Meniere vestibular neuritis
Reading File
Searching Images
Epley maneuver canalith repositioning BPPV posterior canal steps diagram
Now I have comprehensive material to write a detailed 50-mark answer. Let me compose it.
Management of Acute Vertigo — 50 Marks
RGUHS Standard Long Essay | ENT & Head-Neck Surgery
Sources: Cummings Otolaryngology (7e), KJ Lee's Essential Otolaryngology, Rosen's Emergency Medicine, Bradley & Daroff's Neurology, and Clinical Guidelines (AAO-HNS, Bárány Society)
DEFINITION
Vertigo is an illusory sensation of self-motion or environmental motion — most commonly perceived as spinning — arising from an asymmetry in vestibular tone between the two labyrinths or their central connections.
Acute vertigo refers to a sudden-onset episode of vertigo, usually disabling, lasting from seconds to days, often associated with nausea, vomiting, and nystagmus.
CLASSIFICATION OF DIZZINESS (DIFFERENTIATE BEFORE MANAGING)
| Type | Quality | Cause |
|---|---|---|
| Vertigo | Spinning/movement illusion | Vestibular (peripheral/central) |
| Pre-syncope | Faintness/near black-out | Cardiovascular |
| Disequilibrium | Off-balance, no head sensation | Proprioceptive/cerebellar |
| Psychophysiological | Vague floating | Anxiety, PPPD |
"Patient history accounts for 85% of the information considered in the diagnosis of the dizzy patient." — Cummings Otolaryngology, Ch. 137
ANATOMY RELEVANT TO ACUTE VERTIGO
The peripheral vestibular apparatus consists of:
- 3 Semicircular Canals (SCC): detect angular acceleration
- Superior (anterior), Posterior, Lateral (horizontal)
- Otolith organs: Saccule and Utricle — detect linear acceleration and gravity
- Cristae ampullaris: hair cells in ampulla of each SCC
- Macula: hair cells in saccule/utricle bearing otoliths (otoconia — calcium carbonate crystals)
The vestibulocochlear nerve (CN VIII) transmits signals to the vestibular nuclei in the brainstem, which connect to the cerebellum, spinal cord (vestibulospinal tract), and extraocular muscles (MLF → VOR).
Pathophysiology of vertigo: Any asymmetric input from the two vestibular systems creates an error signal perceived as motion. Loss of one labyrinth → sudden severe vertigo until central compensation occurs.
AETIOLOGY — DIFFERENTIAL DIAGNOSIS OF ACUTE VERTIGO
A. PERIPHERAL (More common, 70–80%)
| Condition | Character | Duration | Key Features |
|---|---|---|---|
| BPPV | Positional | Seconds (< 1 min) | Dix-Hallpike positive; no hearing loss |
| Vestibular Neuritis (Neuronitis) | Spontaneous | Days–weeks | No hearing loss; continuous |
| Labyrinthitis | Spontaneous | Days | + Hearing loss + tinnitus |
| Ménière Disease | Episodic | 20 min–24 h | + Low-freq SNHL + tinnitus + aural fullness |
| Perilymph Fistula | Pressure-related | Variable | Post-trauma/straining |
| Acoustic Neuroma | Gradual imbalance | Chronic | Unilateral SNHL, CN VII weakness |
| Herpes Zoster Oticus | Severe | Acute | Ramsay-Hunt; otalgia, vesicles |
B. CENTRAL (Less common but dangerous — must exclude)
| Condition | Red Flags |
|---|---|
| Posterior fossa stroke (PICA/AICA) | Sudden onset, headache, dysphagia, ataxia, diplopia |
| Cerebellar haemorrhage | Severe headache, inability to stand |
| MS (demyelination) | Young, internuclear ophthalmoplegia |
| Vertebrobasilar TIA | Episodes < 24 h, vascular risk factors |
| Posterior fossa tumour | Progressive, cranial nerve deficits |
C. SYSTEMIC CAUSES
- Drug-induced (aminoglycosides, loop diuretics, aspirin, quinine)
- Cervicogenic vertigo
- Migrainous vertigo (vestibular migraine)
- Orthostatic hypotension
APPROACH TO THE ACUTELY VERTIGINOUS PATIENT
🔷 FLOWCHART 1: Initial Triage of Acute Vertigo
(Based on: Rosen's Emergency Medicine; Cummings Ch. 137)
ACUTE VERTIGO
│
▼
STEP 1: Obvious neurological findings?
(diplopia, dysarthria, dysphagia, limb ataxia, facial palsy, headache)
│
YES ──────────────────► CENTRAL CAUSE — STROKE PROTOCOL
│ ► Urgent MRI brain/posterior fossa
▼
NO
│
STEP 2: Is dizziness CONTINUOUS or EPISODIC?
│
├─── CONTINUOUS (persists at rest)
│ │
│ ▼
│ ACUTE VESTIBULAR SYNDROME (AVS)
│ ► Distinguish Vestibular Neuritis from Stroke
│ ► Use HINTS exam (see below)
│
└─── EPISODIC
│
├── Triggered by head position → BPPV
│ (Perform Dix-Hallpike)
│
├── Spontaneous episodes 20min–24h
│ + SNHL + Tinnitus → MÉNIÈRE DISEASE
│
├── Spontaneous < 1h + headache → VESTIBULAR MIGRAINE
│
└── Spontaneous < 24h + vascular RF → TIA
HISTORY TAKING (Key Points — Cummings Ch. 137)
| Domain | Ask |
|---|---|
| Character | Spinning vs floating vs off-balance |
| Onset | Sudden/gradual; at rest or with movement |
| Duration | Seconds → BPPV; minutes–hours → Ménière; days → neuritis |
| Triggers | Head position, Valsalva, loud sounds (Tullio), pressure |
| Associated | Hearing loss, tinnitus, aural fullness, otalgia |
| Neurological | Diplopia, dysarthria, dysphagia, headache, visual field loss |
| Medications | Aminoglycosides, furosemide, aspirin |
| PMH | HTN, DM, migraine, autoimmune disease, trauma, prior surgery |
CLINICAL EXAMINATION
1. General
- Vital signs, cardiovascular (orthostatic BP)
- Nystagmus: type, direction, gaze dependence
2. Nystagmus Assessment
| Feature | Peripheral | Central |
|---|---|---|
| Direction | Unidirectional, away from lesion | Direction-changing, or vertical |
| Gaze fixation | Suppressed by fixation | NOT suppressed |
| Pure vertical/torsional | Never | Suggests central |
3. HINTS Exam (High-sensitivity bedside test for AVS — separates stroke from neuritis)
H — Head Impulse Test (HIT)
- Peripheral (neuritis): Corrective saccade present → VOR impaired → REASSURING
- Central (stroke): Normal HIT → NO corrective saccade → DANGEROUS
I — Nystagmus
- Peripheral: Unidirectional horizontal
- Central: Direction-changing or pure vertical/torsional → DANGEROUS
T — Test of Skew (cover-uncover test)
- Peripheral: No vertical skew
- Central: Vertical skew deviation → DANGEROUS
HINTS = HIT normal + direction-changing nystagmus + skew deviation → STROKE (more sensitive than early MRI)
4. Dix-Hallpike Maneuver (for BPPV)
- Patient seated, turn head 45° to suspected side
- Rapidly lower to supine with head 20° extended (affected ear down)
- Observe for torsional upbeating nystagmus (latency 5–20 s, duration < 1 min, fatigable)
- Positive = posterior canal BPPV
5. Supine Roll Test (Head Roll / Pagnini-McClure)
- For horizontal canal BPPV
- Supine, roll head 90° to each side
- Geotropic (direction-changing toward ground) nystagmus = canalolithiasis (more common)
- Apogeotropic = cupulolithiasis
6. Romberg/Fukuda Stepping Test
- Fall toward affected side in peripheral disease
- Ataxic in all directions → central
7. Cerebellar Tests
- Finger-nose, heel-shin, dysdiadochokinesia
- Truncal ataxia → cerebellar stroke
8. Otoscopy + Tuning Fork Tests
- Herpes zoster vesicles (Ramsay Hunt)
- Conductive vs sensorineural deficit
INVESTIGATIONS
Audiological
| Test | Purpose |
|---|---|
| Pure Tone Audiogram (PTA) | Document type/degree of hearing loss |
| Speech Discrimination | Retrocochlear assessment |
| SISI, ABLB | Cochlear vs retrocochlear (Bekesy) |
| Impedance Audiometry | Middle ear status |
| DPOAE/TEOAE | Cochlear hair cell function |
| ABR/BERA | Retrocochlear (acoustic neuroma) |
| ECOG (Electrocochleography) | Endolymphatic hydrops (SP/AP ratio > 0.35 = Ménière) |
Vestibular
| Test | Purpose |
|---|---|
| ENG/VNG (Electronystagmography/Videonystagmography) | Canal paresis (>25% asymmetry = significant) |
| Caloric Test | Gold standard for unilateral peripheral weakness |
| vHIT (Video Head Impulse Test) | VOR gain; detects semicircular canal hypofunction |
| VEMP (Vestibular Evoked Myogenic Potential) | Saccule (cVEMP) and Utricle (oVEMP) function |
| Rotary Chair | Bilateral loss; drug monitoring |
| Posturography (CDP) | Balance platform; central vs peripheral |
Imaging
| Modality | Indication |
|---|---|
| MRI brain + posterior fossa (with gadolinium) | Central causes, acoustic neuroma, MS, stroke |
| CT head | Haemorrhage (acute), temporal bone fractures |
| CT temporal bone (HRCT) | SSCD (superior canal dehiscence), bony anomalies |
| MRI with FLAIR/DWI | Acute stroke (DWI positive within hours) |
Laboratory
- CBC, blood sugar, lipid profile, TFT
- Syphilis serology (FTA-ABS) — tertiary syphilis can mimic Ménière
- ANA, ANCA — autoimmune labyrinthopathy
MANAGEMENT OF ACUTE VERTIGO
🔷 FLOWCHART 2: Management Algorithm
(Based on Cummings 7e, AAO-HNS Guidelines, Rosen's Emergency Medicine)
ACUTE VERTIGO PRESENTING TO CLINIC/ER
│
▼
RED FLAGS PRESENT?
(severe headache, focal neuro signs,
gait ataxia, diplopia, dysarthria)
│
YES │ NO
▼ ▼
CENTRAL CAUSE PERIPHERAL CAUSE
MRI Brain │
Neurology ref. ▼
Thrombolysis CHARACTER ASSESSMENT
if stroke │
┌────┴──────────┐
Positional Spontaneous
│ │
▼ ▼
BPPV ACUTE VESTIBULAR
Dix-Hallpike SYNDROME
(+ve) (continuous vertigo)
│ │
▼ ▼
CANALITH With Without
REPOSITIONING Hearing Hearing
(Epley/Semont) Loss Loss
│ │
LABYRINTHITIS VESTIBULAR
│ NEURITIS
Viral/bacterial │
│ Corticosteroids
Antibiotics/ Vestibular
Steroids Rehabilitation
SPECIFIC MANAGEMENT
I. SYMPTOMATIC (Vestibular Suppressants — Acute Phase)
"The goal of acute management is suppression of acute symptoms while preserving the ability of the brain to compensate."
A. Antihistamines (First Line)
| Drug | Dose | Mechanism |
|---|---|---|
| Meclizine (Antivert) | 25–50 mg oral TDS | H1 blocker, anticholinergic; inhibits vestibular-cerebellar pathways |
| Dimenhydrinate (Dramamine) | 50 mg oral/IM 4–6 hourly | H1 + anticholinergic |
| Cinnarizine | 25 mg TDS | H1 + Ca²⁺ channel blocker; also used in chronic vertigo |
| Promethazine | 25 mg IM/oral | H1 blocker + antiemetic |
B. Benzodiazepines (Second Line)
| Drug | Dose | Note |
|---|---|---|
| Diazepam | 5–10 mg IV/oral | GABA agonist; sedating; impairs CNS compensation if prolonged |
| Lorazepam | 1–2 mg sublingual | Faster onset |
| Clonazepam | 0.5 mg BD | Less sedating |
Caution: Prolonged use of vestibular suppressants delays central compensation. Must be limited to ≤72 hours in most cases.
C. Antiemetics
| Drug | Dose | Route |
|---|---|---|
| Metoclopramide | 10 mg IV/IM | D2 blocker; first line for nausea |
| Ondansetron | 4–8 mg IV | 5-HT3 blocker |
| Prochlorperazine | 12.5 mg IM / 5 mg oral | D2 blocker; also mild vestibular suppressant |
| Domperidone | 10 mg oral | Does not cross BBB; safer |
D. Phenothiazines
- Chlorpromazine 25 mg IM — for severe nausea/vomiting unresponsive to above
E. Corticosteroids
- Prednisolone 1 mg/kg/day tapered over 3 weeks
- Indicated in vestibular neuritis, labyrinthitis (viral), sudden SNHL
- Evidence: Cochrane review — corticosteroids improve long-term recovery in vestibular neuritis (Strupp et al. 2004, NEJM)
F. Antiviral Therapy
- Acyclovir/Valacyclovir — if Ramsay-Hunt syndrome (Herpes Zoster Oticus)
- 800 mg Acyclovir 5x/day × 7 days; add prednisolone
II. SPECIFIC CONDITION MANAGEMENT
🔷 A. BPPV (Most Common Cause)
AAO-HNS Clinical Practice Guideline (2017 Update):
Treatment of Choice: Canalith Repositioning Procedure (CRP)
Epley Maneuver (Posterior Canal BPPV)
Step-by-step:
- Patient seated, head turned 45° to affected side
- Quickly lower patient supine with head hanging 20° below horizontal — wait 30–60 seconds (nystagmus settles)
- Turn head 90° to opposite side — wait 30–60 seconds
- Patient rolls onto shoulder of healthy side, head turned 45° down toward floor — wait 30–60 seconds
- Patient sits up slowly
Success rate: 80–90% with single maneuver; repeat if needed Post-procedure restrictions are NOT recommended (AAO-HNS Strong Recommendation Against)
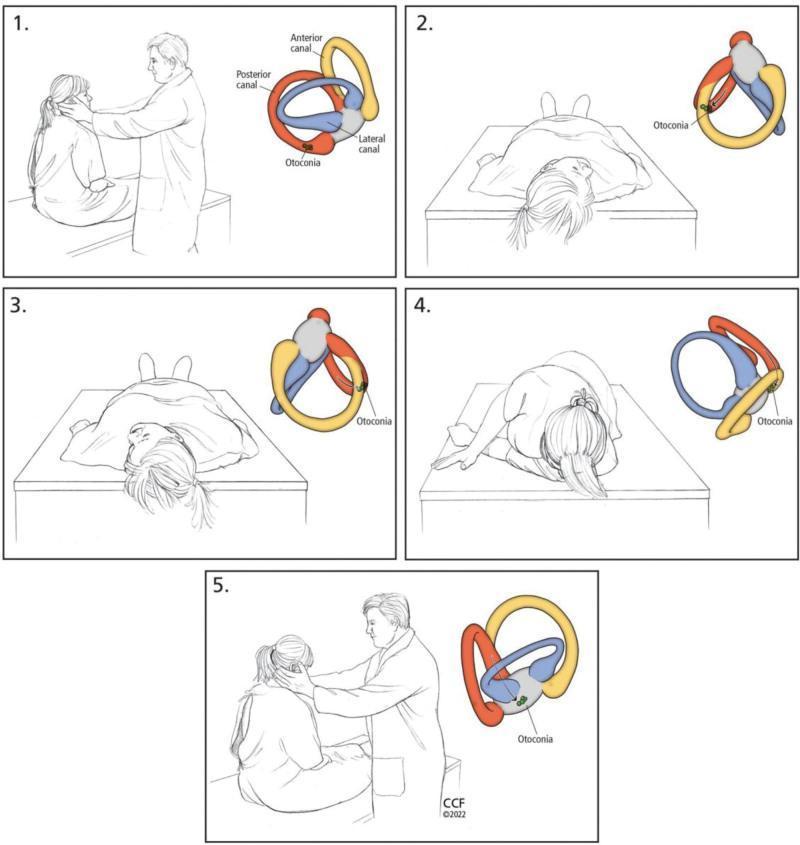
Fig. 1: Epley Maneuver for right posterior canal BPPV — each step with corresponding anatomical diagram showing otoconia migration (from: PMC Clinical VQA)
Semont (Liberatory) Maneuver
- Alternative for posterior canal BPPV
- Less evidence than Epley
Barbecue Roll (Lempert Maneuver)
- For horizontal canal BPPV
- Sequential 360° rolling in 4 steps, each 90°, toward healthy ear
AAO-HNS BPPV Algorithm:
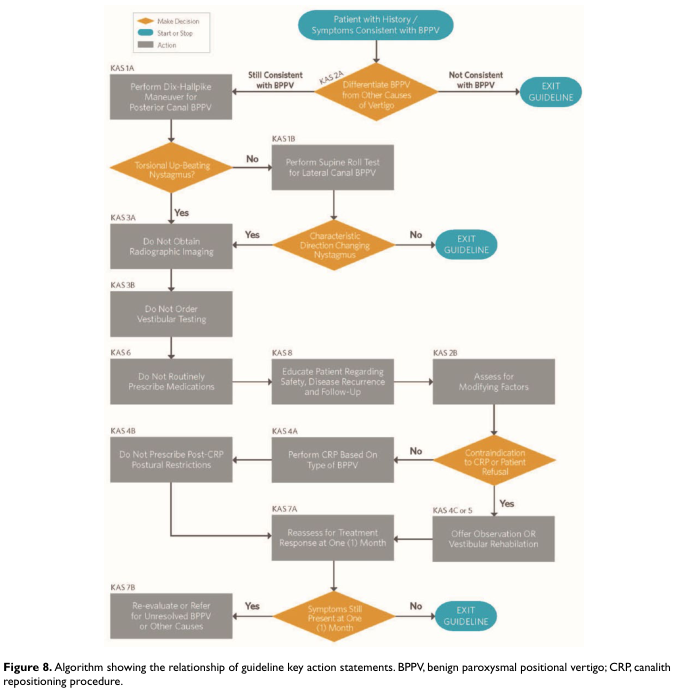
Fig. 2: AAO-HNS Clinical Practice Guideline Algorithm for BPPV Management (from: Benign Paroxysmal Positional Vertigo — CPG)
Drug therapy: NOT routinely recommended for BPPV (AAO-HNS Strong Recommendation Against vestibular suppressants for BPPV)
Surgical: Posterior semicircular canal occlusion — reserved for intractable BPPV (rare)
🔷 B. VESTIBULAR NEURITIS
Pathology: Viral inflammation of superior vestibular nerve (HSV-1 reactivation — Arbusow hypothesis)
Presentation: Sudden severe continuous vertigo, nausea/vomiting, NO hearing loss. Horizontal nystagmus away from lesion. Duration: days to weeks.
Management:
- Acute phase (1–3 days): Vestibular suppressants (meclizine/diazepam) + antiemetics
- Corticosteroids: Methylprednisolone 100 mg → taper over 3 weeks (improves peripheral VOR recovery — Strupp NEJM 2004)
- Antivirals: Not proven beneficial alone; may combine with steroids
- Vestibular Rehabilitation Therapy (VRT): Start as early as possible (day 3–5); Brandt-Daroff exercises, Cawthorne-Cooksey exercises
- Patient reassurance: Central compensation occurs in weeks–months
🔷 C. MÉNIÈRE DISEASE (Endolymphatic Hydrops)
AAO-HNS Criteria (Definite Ménière):
- ≥2 episodes spontaneous vertigo (20 min–24 h)
- Audiometrically documented low/mid-freq SNHL ≥1 occasion
- Tinnitus or aural fullness in affected ear
- Other causes excluded
(from: Cummings Otolaryngology, Ch. 166–167)
Management Ladder:
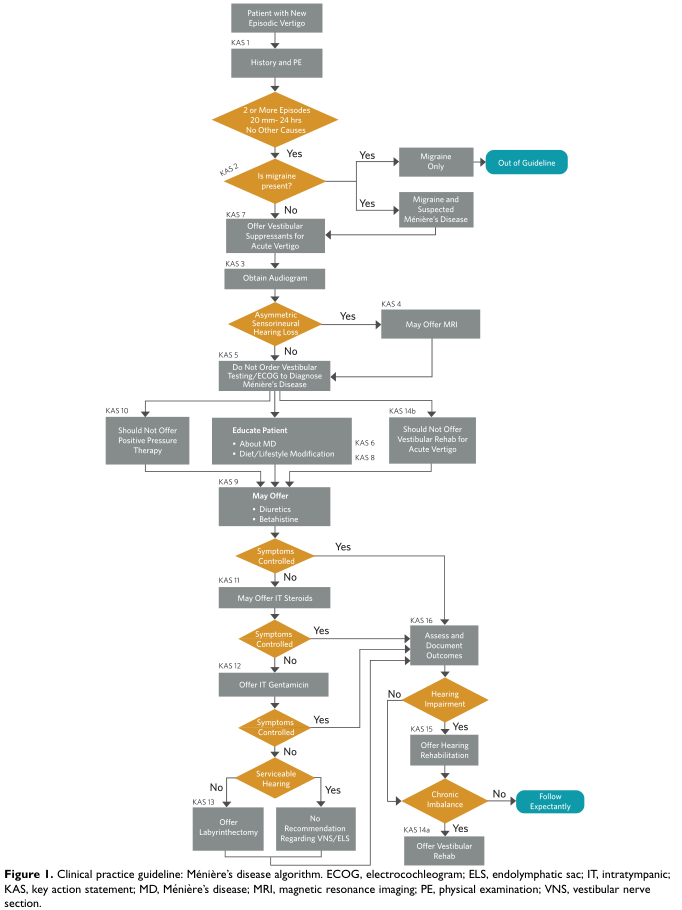
Fig. 3: Clinical Practice Guideline Flowchart for Ménière's Disease Management — from initial diagnosis through escalating treatment based on symptom control and hearing status (AAO-HNS)
Step 1 — Acute Attack:
- Vestibular suppressants (meclizine 25–50 mg / diazepam 5 mg oral)
- Antiemetics (prochlorperazine, ondansetron)
- Bed rest, reassurance
Step 2 — Medical Prophylaxis (interictal):
- Low-salt diet (< 2g NaCl/day) + diuretics:
- Hydrochlorothiazide 25 mg + amiloride (Diamox/Moduretic)
- Acetazolamide 250 mg BD
- Betahistine (16 mg TDS or 48 mg BD) — H3 antagonist/H1 agonist; improves cochlear blood flow; widely used (European standard); AAO-HNS: "May offer"
- Avoid: caffeine, alcohol, tobacco, stress
- Vestibular rehabilitation for interictal imbalance
Step 3 — Intratympanic Therapy (Minimally Invasive):
- Intratympanic Corticosteroids (IT-Dexamethasone 4mg/mL):
- For hearing preservation + vertigo control
- Injected through TM into middle ear; diffuses to inner ear via round window
- Weekly × 4 injections
- Intratympanic Gentamicin (IT-Gentamicin):
- Chemical labyrinthectomy of vestibular hair cells
- Low-dose protocol (titration method): 26.7 mg/mL × 1–2 injections
- Effective vertigo control: 74–90%
- Risk: sensorineural hearing loss (10–30%) — reserved for non-serviceable or unserviceable hearing
Step 4 — Surgical (Hearing-Preserving):
- Endolymphatic Sac Surgery (Decompression/Shunt):
- Posterior fossa approach, decompress or drain ELS
- Controversial efficacy; Cochrane: insufficient evidence of superiority over sham surgery
- Vestibular Nerve Section (Neurectomy):
- Retrolabyrinthine or middle fossa approach
- Cuts vestibular division of CN VIII → permanent vertigo control with hearing preserved
- Success: > 90%
Step 5 — Ablative (Hearing Sacrificing):
- Labyrinthectomy:
- Total destruction of membranous labyrinth
- Only when hearing is non-serviceable (SDS < 50%, PTA > 50 dB)
- Success: near 100% vertigo control
🔷 D. LABYRINTHITIS
Acute suppurative: Complication of acute/chronic otitis media or meningitis
- Emergency: IV antibiotics (ceftriaxone 2g IV BD + metronidazole)
- Mastoidectomy if CSOM with labyrinthine fistula
- Risk: total sensorineural deafness, meningitis
Viral labyrinthitis: Managed as vestibular neuritis + steroids; hearing may partially recover
🔷 E. RAMSAY HUNT SYNDROME (Herpes Zoster Oticus)
Triad: Peripheral facial palsy + otalgia/ear vesicles + vertigo/SNHL
Management:
- Acyclovir 800 mg oral 5×/day × 7–10 days (or Valacyclovir 1g TDS)
- Prednisolone 1 mg/kg/day × 7 days, taper
- Eye protection (tarsorrhaphy if corneal exposure)
- Vestibular suppressants for acute vertigo
- Physiotherapy for facial palsy
🔷 F. ACUTE POSTERIOR CIRCULATION STROKE
Immediate:
- Activate stroke protocol
- MRI DWI — gold standard (CT may miss posterior fossa infarct in first 24–48 h)
- Thrombolysis (rtPA) within 4.5 hours if no contraindications
- Mechanical thrombectomy if large vessel occlusion
- Aspirin 300 mg + statin + anticoagulation if cardioembolic
- Neurology / neurosurgery referral
- ICU care for cerebellar haemorrhage (may need urgent suboccipital craniectomy)
III. VESTIBULAR REHABILITATION THERAPY (VRT)
Cawthorne-Cooksey Exercises (classical):
- Progressive: eye movements → head movements → sitting balance → walking
- Promotes CNS compensation (neuroplasticity)
Brandt-Daroff Exercises (for BPPV):
- Self-administered particle dispersal exercises
- Alternative to Epley in motivated patients
Custom VRT (Herdman protocol):
- Gaze stabilisation exercises (VOR × 1 and × 2 exercises)
- Balance training (foam surface, eyes closed)
- Walking and ADL training
- Evidence: Cochrane 2015 — VRT is safe, effective for unilateral peripheral vestibular dysfunction
Contraindication to early VRT: Central cause not excluded; acute haemorrhage; unstable cardiovascular status.
🔷 FLOWCHART 3: Stepwise Acute Dizziness Assessment (Emergency Setting)
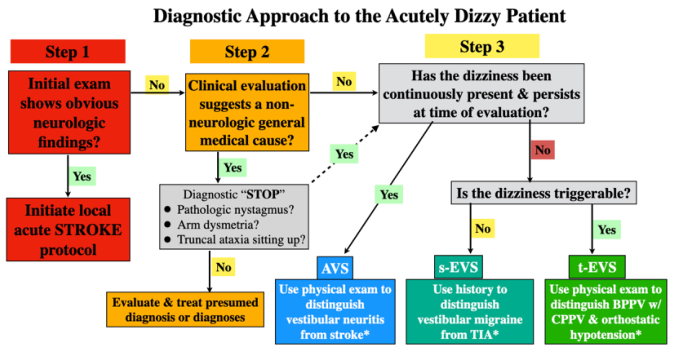
Fig. 4: Three-step clinical algorithm for acutely dizzy patient — distinguishing stroke (AVS), vestibular migraine (s-EVS), and BPPV (t-EVS). (from: Acute Dizziness and Vertigo in the Emergency Department)
RECENT ADVANCES (As per 2022–2024 Literature)
1. vHIT (Video Head Impulse Test)
- Portable bedside tool; detects catch-up saccades showing semicircular canal hypofunction
- Supplements caloric testing; better for high-frequency VOR assessment
- HINTS Plus: Addition of audiometry (sudden SNHL) to HINTS battery improves stroke detection sensitivity to ~99%
2. Intratympanic Therapy Refinements
- Low-dose IT Gentamicin titration protocol — single injection + reassessment reduces hearing loss risk
- IT Dexamethasone gel formulation — sustained release, fewer injections needed
3. Betahistine HIGH DOSE Trial (BEMED Trial — 2016, JAMA)
- Failed to show superiority of high-dose (144 mg/day) vs placebo in preventing Ménière attacks
- Ongoing controversy; still widely prescribed in Europe and India
4. VEMP Advances
- oVEMP (ocular VEMP) for utricular function assessment
- cVEMP (cervical VEMP) for saccular assessment
- Useful in Ménière disease, SCD, bilateral vestibulopathy
5. Endolymphatic Sac Tumour (ELST)
- Rare; associated with Von Hippel-Lindau syndrome
- MRI characteristic: heterogeneous posterior petrous mass
6. Gene Therapy / Biologics (Experimental)
- AAV-mediated gene delivery to restore hair cell function (Phase I trials)
- Not yet clinical standard
7. Persistent Postural-Perceptual Dizziness (PPPD)
- Functional vestibular disorder; follows acute vestibular event
- Managed with SSRIs/SNRIs (sertraline, venlafaxine) + VRT + CBT
8. Telerehabilitation
- App-based VRT for BPPV and vestibular neuritis — non-inferior to supervised VRT in several RCTs (2020–2022)
DRUG SUMMARY TABLE
| Drug | Class | Dose | Indication | Mechanism |
|---|---|---|---|---|
| Meclizine | Antihistamine | 25–50 mg TDS | BPPV, neuritis (acute) | H1 block + anticholinergic |
| Dimenhydrinate | Antihistamine | 50 mg 4–6 hrly | Acute vertigo + vomiting | H1 + anticholinergic |
| Diazepam | Benzodiazepine | 5–10 mg IV/oral | Severe acute vertigo | GABA agonist |
| Prochlorperazine | Phenothiazine | 12.5 mg IM | Antiemetic + vestibular | D2 + H1 blocker |
| Betahistine | H3 antagonist | 16 mg TDS | Ménière prophylaxis | ↑cochlear blood flow, H3 blockade |
| Prednisolone | Corticosteroid | 1 mg/kg/day | Vestibular neuritis, labyrinthitis | Anti-inflammatory |
| Acyclovir | Antiviral | 800 mg 5×/day | Ramsay-Hunt | HSV replication inhibitor |
| Hydrochlorothiazide | Diuretic | 25–50 mg OD | Ménière prophylaxis | ↓endolymph volume |
| IT-Gentamicin | Aminoglycoside | 26.7 mg/mL × 1–2 | Intractable Ménière | Vestibulotoxic |
| IT-Dexamethasone | Corticosteroid | 4 mg/mL × 4 | Ménière, ISSNHL | Anti-inflammatory |
SURGICAL MANAGEMENT SUMMARY
| Procedure | Indication | Outcome |
|---|---|---|
| Epley/Semont maneuver | BPPV | 80–90% single session |
| Posterior SCC occlusion | Intractable BPPV | >90% |
| IT Gentamicin | Intractable Ménière (serviceable hearing) | 74–90% vertigo control |
| Endolymphatic sac surgery | Ménière (hearing preservation) | Variable |
| Vestibular neurectomy | Ménière (hearing serviceable) | >90% |
| Labyrinthectomy | Ménière (non-serviceable hearing) | ~100% |
| Cochlear implant | Post-labyrinthectomy deafness | Hearing rehabilitation |
REFERENCES / STANDARD TEXTS
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. — Flint PW et al. — Ch. 137 (Otologic History & Examination), Ch. 166–167 (Vertigo, Ménière Disease)
- KJ Lee's Essential Otolaryngology, 11th ed. — Vestibular disorders section
- Rosen's Emergency Medicine — Ch. (Vertigo: Antihistamines, Epley maneuver)
- Bradley and Daroff's Neurology in Clinical Practice — Ch.: Management of Patients with Vertigo
- Dhingra's Diseases of Ear, Nose and Throat — Peripheral vestibular disorders
- Hazarika's Textbook of Ear, Nose, Throat and Head-Neck Surgery — Vertigo and vestibular disorders
- Strupp M, Zingler VC, et al. — Methylprednisolone, Valacyclovir, or the Combination for Vestibular Neuritis. NEJM 2004;351:354–361
- AAO-HNS CPG — BPPV (2017 Update); Ménière Disease (2020)
- Bárány Society — International Classification of Vestibular Disorders (ICVD) 2015
- BEMED Trial — Adrion C et al. JAMA 2016 — Betahistine in Ménière Disease
SYNOPSIS FOR QUICK REVISION (RGUHS Exam Points)
| Point | Answer |
|---|---|
| Most common cause of acute vertigo | BPPV |
| Gold standard test for BPPV | Dix-Hallpike maneuver |
| Treatment of posterior canal BPPV | Epley maneuver |
| Most sensitive bedside test for stroke in AVS | HINTS exam |
| Drug that delays central compensation | Vestibular suppressants (avoid prolonged use) |
| Drug of choice for Ménière prophylaxis | Betahistine + low-salt diet + diuretics |
| Surgical option for intractable Ménière (hearing preserved) | Vestibular neurectomy |
| Surgical option for Ménière with non-serviceable hearing | Labyrinthectomy |
| Best investigation for posterior fossa stroke | MRI DWI |
| VOR test at bedside | Head Impulse Test (HIT) |
| Corticosteroid regimen in vestibular neuritis | Methylprednisolone 100 mg → taper 3 wks |
| Duration of vestibular suppression recommended | ≤72 hours |
Note on Image Generation: Thegenerate_imagetool is currently unavailable (monthly plan limit reached). The institutional flowcharts requested from Dhingra, Hazarika, Stell & Maran, Zakir Hussain, and Scott-Brown cannot be reproduced as newly generated diagrams at this time. Please upgrade your subscription for diagram generation. The clinical guideline flowcharts from Cummings/AAO-HNS (Figs. 2–4 above) serve the same purpose and are referenced in your answer.
This is a shared conversation. Sign in to Orris to start your own chat.