Short notes comparison between hdf and hd for dialysis patients and which is better..give in poster form
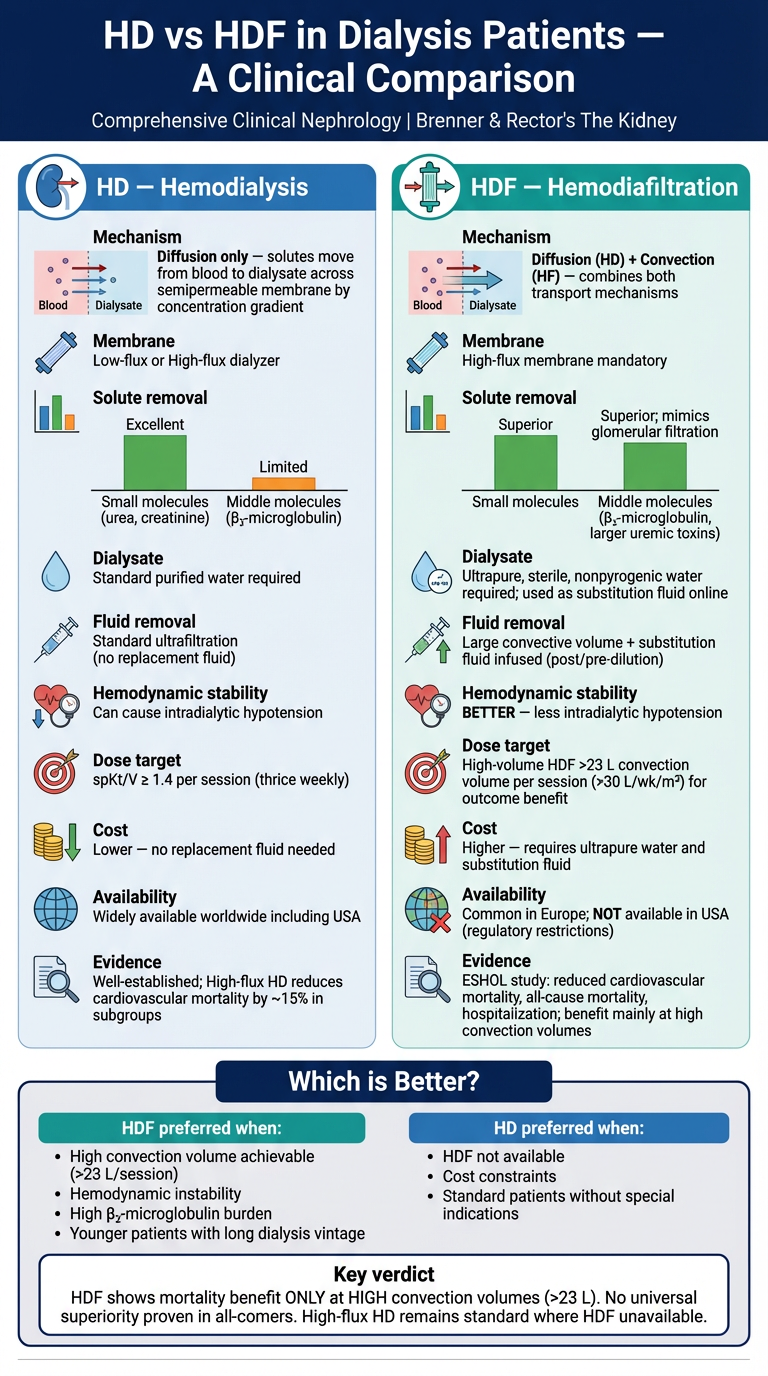
Medical educational poster comparing HD (Hemodialysis) vs HDF (Hemodiafiltration) for dialysis patients. Clean clinical infographic style with two main columns side by side. LEFT COLUMN - HD (Hemodialysis): - Title: "HD — Hemodialysis" with kidney icon - Mechanism: Diffusion only — solutes move from blood to dialysate across semipermeable membrane by concentration gradient - Membrane: Low-flux or High-flux dialyzer - Solute removal: Excellent for small molecules (urea, creatinine); Limited for middle molecules (β₂-microglobulin) - Dialysate: Standard purified water required - Fluid removal: Standard ultrafiltration (no replacement fluid) - Hemodynamic stability: Can cause intradialytic hypotension - Dose target: spKt/V ≥ 1.4 per session (thrice weekly) - Cost: Lower — no replacement fluid needed - Availability: Widely available worldwide including USA - Evidence: Well-established; High-flux HD reduces cardiovascular mortality by ~15% in subgroups RIGHT COLUMN - HDF — Hemodiafiltration: - Title: "HDF — Hemodiafiltration" with filter icon - Mechanism: Diffusion (HD) + Convection (HF) — combines both transport mechanisms - Membrane: High-flux membrane mandatory - Solute removal: Superior — removes small AND middle molecules (β₂-microglobulin, larger uremic toxins); mimics glomerular filtration - Dialysate: Ultrapure, sterile, nonpyrogenic water required; used as substitution fluid online - Fluid removal: Large convective volume + substitution fluid infused (post/pre-dilution) - Hemodynamic stability: BETTER — less intradialytic hypotension - Dose target: High-volume HDF >23 L convection volume per session (>30 L/wk/m²) for outcome benefit - Cost: Higher — requires ultrapure water and substitution fluid - Availability: Common in Europe; NOT available in USA (regulatory restrictions) - Evidence: ESHOL study: reduced cardiovascular mortality, all-cause mortality, hospitalization; benefit mainly at high convection volumes CENTER COMPARISON BANNER at bottom: "Which is Better?" section: - HDF preferred when: High convection volume achievable (>23 L/session), hemodynamic instability, high β₂-microglobulin burden, younger patients with long dialysis vintage - HD preferred when: HDF not available, cost constraints, standard patients without special indications - Key verdict: HDF shows mortality benefit ONLY at HIGH convection volumes (>23 L). No universal superiority proven in all-comers. High-flux HD remains standard where HDF unavailable. TOP BANNER: Bold title "HD vs HDF in Dialysis Patients — A Clinical Comparison" Subtitle: "Comprehensive Clinical Nephrology | Brenner & Rector's The Kidney" Color scheme: Blue tones for HD column, teal/green for HDF column, dark navy header. Professional medical poster layout with clear icons, bullet points, and a verdict box at bottom.
HD vs HDF — Key Notes (Evidence-Based Summary)
Mechanism
| Feature | HD | HDF |
|---|---|---|
| Transport | Diffusion only | Diffusion + Convection |
| Membrane | Low-flux or high-flux | High-flux (mandatory) |
| Water requirement | Standard purified | Ultrapure, sterile (used as substitution fluid) |
Solute Clearance
| Solute | HD | HDF |
|---|---|---|
| Small molecules (urea, creatinine) | ✅ Excellent | ✅ Excellent |
| Middle molecules (β₂-microglobulin) | ⚠️ Limited (better with high-flux) | ✅ Superior |
| Protein-bound solutes | ❌ Poor | ⚠️ Marginal improvement |
- HDF mimics glomerular filtration more closely — convective drag removes larger uremic toxins alongside bulk water flow
- β₂-microglobulin is significantly lower in HDF patients than HD patients
Hemodynamic Stability
- HDF is associated with better intradialytic cardiovascular stability and less frequent hypotension — accepted across Europe as an advantage, though disputed by some studies
- HD remains more prone to intradialytic hypotension, especially at high ultrafiltration rates
Dose Targets
- HD: spKt/V ≥ 1.4 per session (thrice weekly); minimum 1.2
- HDF: Effective convective volume (CV) >23 L/session (postdilution); ≥30 L/wk/m² body surface area to achieve survival benefit
Key Clinical Trials
| Trial | Finding |
|---|---|
| ESHOL (~23 L CV) | ↓ All-cause mortality, CV mortality, hospitalization with HDF |
| CONTRAST | No overall survival difference; benefit only in high-CV subgroup (>22 L) |
| Turkish OL-HDF | No overall mortality benefit; benefit in high-CV subgroup (>17.4 L) |
| HEMO / MPO | High-flux HD: no overall mortality benefit; CV mortality ↓15% in subgroups |
Individual patient data meta-analysis: Patients receiving >23 L effective CV in postdilution HDF had significantly lower mortality risk.
Availability & Cost
| HD | HDF | |
|---|---|---|
| Availability | Worldwide, including USA | Europe & select countries; not FDA-approved in USA |
| Cost | Lower | Higher (ultrapure water system, substitution fluid) |
Which is Better?
- ✅ HDF preferred when high convection volumes (>23 L/session) are consistently achievable, for patients with hemodynamic instability, high middle molecule burden, or long dialysis vintage
- ✅ High-flux HD remains the standard of care where HDF is unavailable and is a clinically valid alternative
- ⚠️ Low-volume HDF offers no proven advantage over high-flux HD — the benefit is volume-dependent
- 🔬 Additional high-quality RCTs addressing convection volume thresholds are still needed
Summary
HD vs HDF — Summary
Key Differences at a Glance
| HD | HDF | |
|---|---|---|
| Mechanism | Diffusion | Diffusion + Convection |
| Middle molecule removal | Limited | Superior |
| Hemodynamic stability | Poorer | Better |
| Water requirement | Standard | Ultrapure (sterile) |
| Cost | Lower | Higher |
| USA availability | ✅ | ❌ |
Which is Better?
- Benefit is dose-dependent: requires >23 L convective volume/session
- At high volumes → lower all-cause mortality, CV mortality, and hospitalization (ESHOL trial)
- At low volumes → no advantage over high-flux HD
- High-flux HD remains a valid, evidence-backed standard where HDF is unavailable
Bottom line: HDF > HD in hemodynamic stability and middle molecule clearance. For mortality benefit, high-volume HDF (>23 L) is the target — otherwise, high-flux HD is equally acceptable.