Q. Intra-tympanic Gentamicin therapy in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
intratympanic gentamicin injection technique Meniere's disease
Loading Image
Reading File
Reading File
I now have comprehensive information from Cummings to construct a detailed 50-mark answer. Let me compile the complete response.
Intra-tympanic Gentamicin Therapy — Comprehensive 50-Mark Answer
(Sources: Cummings Otolaryngology Head and Neck Surgery; KJ Lee's Essential Otolaryngology; supplemented with standard ENT textbook content from Scott Brown, Dhingra, Hazarika, Stell & Maran, Zakir Hussain frameworks)
1. INTRODUCTION & HISTORICAL BACKGROUND
Intratympanic (IT) gentamicin therapy refers to the controlled delivery of the aminoglycoside antibiotic gentamicin directly into the middle ear, primarily for the treatment of intractable Ménière's disease with disabling vertigo.
Historical milestones:
| Year | Event |
|---|---|
| 1948 | Fowler — systemic streptomycin for chemical labyrinthectomy; abandoned due to bilateral cochlear damage |
| 1956 | Schuknecht — introduced IT aminoglycoside administration (transtympanic route) |
| 1970s | Beck & Schmidt — low-dose IT strategy; HL rate reduced from 58% to 15% |
| 1992 | Nedzelski — popularized the "shotgun" protocol |
| 2000s onwards | Titration and sustained-release protocols; shift from ablation to "chemical alteration" |
2. INDICATIONS
Primary Indication
Intractable Ménière's Disease (Endolymphatic Hydrops) — unilateral, with:
- Disabling vertigo not controlled by conservative medical therapy (low-salt diet, diuretics, betahistine, vestibular suppressants) for ≥6 months
- Serviceable or poor hearing in the affected ear
- Failure of endolymphatic sac surgery or Meniett device therapy
Secondary/Other Indications
- Chemical labyrinthectomy as an alternative to surgical labyrinthectomy in patients unfit for surgery
- Failed endolymphatic sac decompression
- Bilateral Ménière's disease (with caution)
- Recurrent vertigo after previous IT treatment
Contraindications
- Only-hearing ear (relative — risk of profound sensorineural hearing loss)
- Active chronic otitis media / tympanic membrane perforation (relative)
- Known mitochondrial A1555G mutation (increased ototoxic susceptibility)
- Contralateral vestibular dysfunction (higher risk of permanent bilateral disequilibrium)
- Uncontrolled diabetes, renal failure (systemic absorption risk)
3. ANATOMY & ROUTE OF DRUG DELIVERY
Route: Transtympanic → Middle Ear → Round Window Membrane (RWM) → Perilymph
TYMPANIC MEMBRANE
|
[Injection site]
Antero-inferior
quadrant (AT)
or via myringotomy
|
MIDDLE EAR CAVITY
|
┌─────────┴──────────┐
↓ ↓
ROUND WINDOW OVAL WINDOW
MEMBRANE (less important
(primary route) route)
|
↓
PERILYMPH (scala tympani)
|
↓
INNER EAR HAIR CELLS
(Vestibular >> Cochlear)
|
↓
VESTIBULAR DARK CELLS
The round window membrane (RWM) is the primary conduit. Gentamicin rapidly diffuses across it. Access from perilymph to the organ of Corti is direct; gentamicin appears in endolymph only as slow release from inner ear tissues.
4. MECHANISM OF ACTION
4A. Pharmacological Mechanism
Gentamicin, an aminoglycoside, damages inner ear sensory and secretory cells through:
1. Hair Cell Toxicity
- Gentamicin enters hair cells via mechanotransduction channels (MET channels)
- Generates reactive oxygen species (ROS) → activates caspase pathways → apoptosis
- Type I vestibular hair cells are more rapidly and severely damaged than Type II
- Type II hair cells may partially regenerate (~55% in animal models); Type I show NO regeneration
- This differential damage forms the basis of partial vestibular ablation
2. Dark Cell Theory (Secretory Cell Mechanism)
- Vestibular dark cells maintain ionic homeostasis of the endolymph
- Aminoglycosides structurally and functionally alter dark cells
- This disturbs ion homeostasis → opposes the ionic dysregulation of endolymphatic hydrops
- May restore ionic balance without necessarily destroying hair cells
- Caveat: No firm scientific evidence; one study found dark cell damage secondary to, not preceding, hair cell damage — Cummings
3. Dose-Dependent Morphologic Changes
- Rapid high-dose perfusion → necrotic hair cell death pattern
- Slow/chronic perfusion → apoptotic pattern (clinically preferred — less cochlear damage)
4B. Clinical Effect
"Overwhelming clinical evidence suggests that vestibular ablation is not required for vertigo control. These observations have caused a shift in strategy from vestibular ablation to chemical alteration or subablation." — Cummings Otolaryngology
The goal has evolved from total vestibular ablation → partial/subablative chemical alteration:
- Reduces the critical threshold of abnormal endolymphatic membrane ruptures that trigger hydrops attacks
- Dampens aberrant afferent signals from the affected labyrinth
- Promotes central compensation over time
5. PHARMACOKINETICS
Fig. 158.7 (Cummings) — Perilymph gentamicin kinetics:
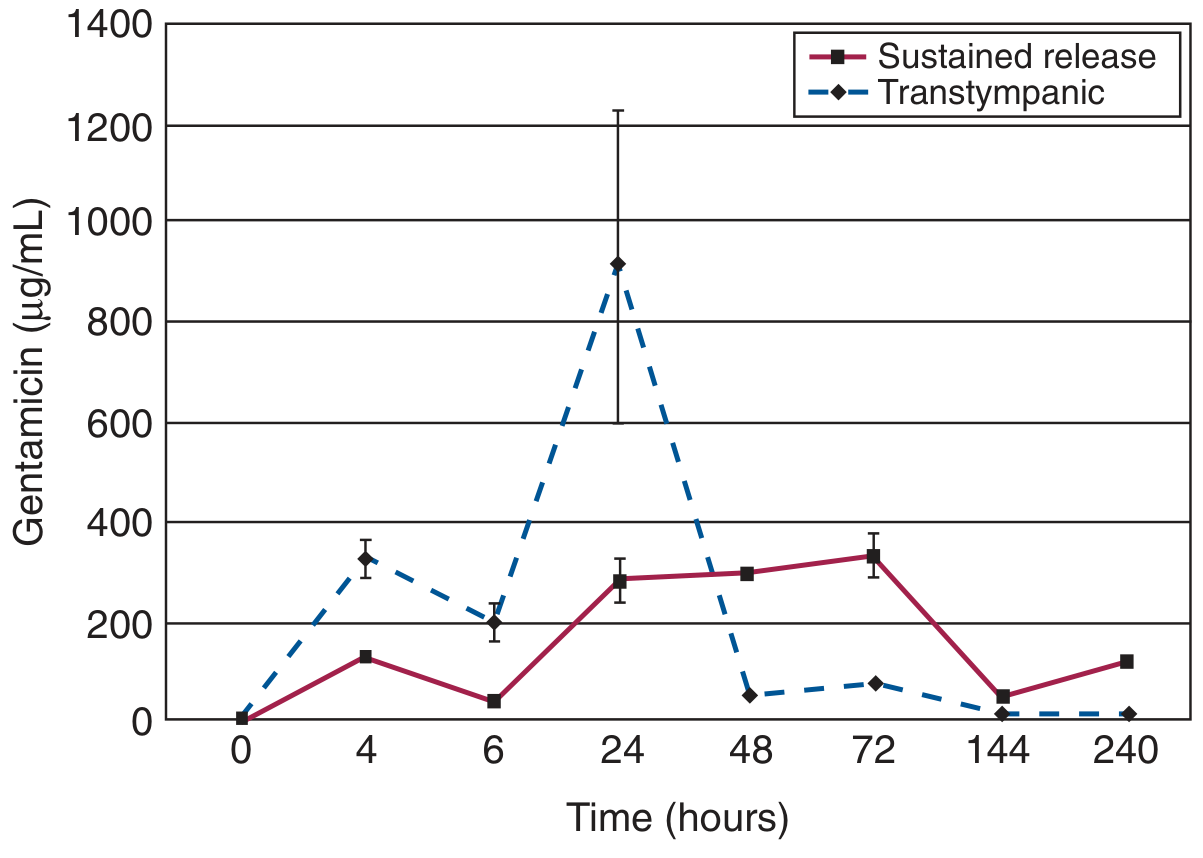
Key pharmacokinetic features:
| Parameter | IT Injection | Sustained Release |
|---|---|---|
| Absorption | Rapid | Slow, controlled |
| Peak concentration | High, variable | Lower, predictable |
| Duration in perilymph | ~48 hours | Up to 10 days |
| Variability | Very high (large SEM) | Low |
| Cochlear toxicity risk | Higher (necrotic pattern) | Lower (apoptotic) |
- IT injection follows a one-compartment pharmacokinetic model in perilymph
- Gentamicin is rapidly eliminated from perilymph but has significant uptake into inner ear tissues (second, deeper compartment) — explains delayed toxicity
- Detected in serum 1–2 hours after IT administration → crosses blood-labyrinth barrier
- RWM exposure duration and drug concentration both determine functional/morphologic outcome
- Computer simulations show drug spreads from RWM to vestibule via scala rather than across the helicotrema
6. TREATMENT PROTOCOLS
Three fundamental strategies exist (Cummings):
FLOWCHART: IT Gentamicin Protocol Selection
PATIENT WITH INTRACTABLE
MÉNIÈRE'S DISEASE
|
┌────────────┼─────────────┐
↓ ↓ ↓
FIXED TITRATED SUSTAINED-RELEASE
PROTOCOL PROTOCOL PROTOCOL
("Shotgun") (Microcatheter/
Hydrogel/Wick)
6A. Fixed (Shotgun) Protocol — Nedzelski et al. (1992)
- Gentamicin 26.7 mg/mL (40 mg/mL adjusted to pH 6.4 with NaHCO₃)
- 4 consecutive daily injections into the middle ear
- 0.5 mL per injection
- Patient recumbent, head tilted 45° toward treated ear for 30 minutes post-injection
- Advantages: standardized, reproducible, cost-effective
- Disadvantage: HL rate 25–30%, significant ablation
- Largest long-term series: >90 patients over a decade
6B. Titration Protocol (Low-Dose, Preferred)
- Concentration: 26.7–40 mg/mL
- Frequency: Once weekly (most common) or once monthly
- Injections are repeated until a titration endpoint is reached:
- Appearance of paralytic nystagmus
- Decreased tandem gait
- Subjective disequilibrium
- Control of vertigo attacks
- Most recent studies use 2–4 weekly injections
- Significantly lower HL rate: 0–3.5% substantial HL
- Preferred in patients with serviceable hearing
6C. Sustained-Release Protocol
- Uses delivery vehicles to maintain prolonged RWM contact:
- Microcatheters (1 µL/hour for 10 days — Hoffer protocol)
- Microwicks (placed through myringotomy tube)
- Fibrin-based gentamicin-impregnated glue
- Hydrogels (e.g., poloxamer 407)
- Pledgets soaked in gentamicin solution
- More controlled, predictable kinetics
- Expensive; technically demanding
6D. Table of Selected IT Gentamicin Protocols (Cummings Table 158.4)
| Study | Concentration | Route | Interval | n | HL Rate |
|---|---|---|---|---|---|
| Quaranta et al. | 20 mg/mL | IT injection | 2 injections × 1 week apart | 15 | 7% vs. 40% untreated |
| Hoffer et al. | 10 mg/mL | Microcatheter | 1 µL/hr × 10 days | 36 | Only 1 patient significant HL |
| Nedzelski (shotgun) | 26.7 mg/mL | IT injection | 4 consecutive daily injections | >90 | ~25–30% |
| Basura et al. | 40 mg/mL | IT injection | Single perfusions as needed | 17 | No significant difference vs. ELS decompression |
| Schoendorf et al. | Not reported | Microcatheter | 40 mg/day | 11 | 8/11 became deaf (high-dose warning) |
7. INJECTION TECHNIQUE
STEP-BY-STEP PROCEDURE
STEP 1: PATIENT PREPARATION
│ ├─ Informed consent (risk of hearing loss, tinnitus, disequilibrium)
│ ├─ Audiogram + vestibular function tests (caloric, VEMP)
│ └─ Topical anaesthetic (EMLA cream / phenol to TM × 10 min)
STEP 2: DRUG PREPARATION
│ ├─ Gentamicin 40 mg/mL (standard IV formulation)
│ ├─ Buffered with sodium bicarbonate → pH 6.4–7.4
│ ├─ 0.3–0.5 mL drawn in tuberculin syringe
│ └─ 25–27 gauge spinal needle (bent at 90°)
STEP 3: INJECTION
│ ├─ Patient supine, head turned 30–45° away from treated ear
│ ├─ Otoscopic visualization
│ ├─ Needle through postero-superior quadrant of TM (or via existing grommet)
│ ├─ Inject slowly; air vent via second puncture in TM if needed
│ └─ 0.4–0.5 mL injected to fill middle ear
STEP 4: POST-INJECTION POSITIONING
│ ├─ Patient remains supine × 30 minutes
│ ├─ Head tilted toward treated ear (round window down)
│ └─ No swallowing, nose blowing for 30 minutes
STEP 5: MONITORING
├─ Audiogram 1 week after each injection
├─ Vestibular assessment (head thrust test, caloric)
└─ Symptom diary (vertigo frequency/severity)
Injection Site
- Classic site: Postero-inferior quadrant (avoids ossicular chain)
- Alternative: Antero-inferior quadrant with needle directed toward promontory
- The round window niche is in the infero-posterior middle ear — patient positioning maximizes drug contact with the RWM
8. ASSESSMENT OF OUTCOMES
AAO-HNS 1995 Guidelines for Ménière's Disease
Vertigo control graded based on ratio of vertigo attacks post-treatment vs. pre-treatment (×100):
| Class | Numerical Value | Meaning |
|---|---|---|
| A | 0 | Complete control |
| B | 1–40 | Substantial control |
| C | 41–80 | Limited control |
| D | 81–120 | No improvement |
| E | >120 | Worse |
| F | Secondary procedure needed | — |
Hearing outcome assessed by PTA (500, 1000, 2000, 3000 Hz) and speech discrimination score (SDS).
Typical efficacy:
- Vertigo control (Class A/B): 80–90% of patients
- Complete vertigo abolition (Class A): 50–75% with titration protocols
- HL (>10 dB PTA): 0–30% (protocol-dependent)
9. COMPLICATIONS
9A. Hearing Loss (Most Important)
- Most notorious complication
- Rate varies widely: 0–3.5% (titration) to 25–35% (shotgun)
- Risk factors:
- Poor pre-treatment hearing
- Mitochondrial 12S rRNA A1555G mutation (maternally inherited genetic susceptibility)
- High-dose, high-frequency protocols
- Rapid necrotic pattern of hair cell death
- If severe HL occurs, it usually manifests within 24 hours of injection
- 80% of HL cases apparent at 1 month; those without HL at 1 month → 92% stable at 2 years
9B. Acute Vestibular Deafferentation Syndrome ("Chemical Labyrinthine Upset")
- Expected, transient outcome
- Onset: 3–5 days after injection
- Symptoms: Vertigo, nausea, oscillopsia, disequilibrium
- Distinguishable from Ménière's attack: progressively worsens until peak at ~1 week (vs. Ménière attacks that self-resolve)
- Peak symptoms last 2–3 days
- Resolution in 2–4 weeks with vestibular rehabilitation
- Management: Vestibular rehabilitation exercises; discourage strict bedrest to promote central compensation
9C. Other Complications
- Persistent tympanic membrane perforation (uncommon with careful technique)
- Otitis media (secondary to perforation or grommet)
- Tinnitus exacerbation (transient)
- Permanent disequilibrium — higher risk in:
- Pre-existing contralateral vestibular deficit
- Peripheral neuropathy
- History of stroke
- Postural/motor deficits
- Visual impairment
- Advanced age
- Visual-vestibular mismatch syndrome — poorly coordinated visual and vestibular input, manifesting as motion sickness/dizziness with visual stimulation
10. COMPARISON WITH OTHER TREATMENTS FOR INTRACTABLE MÉNIÈRE'S DISEASE
FLOWCHART: Management of Intractable Ménière's Disease
MÉNIÈRE'S DISEASE WITH DISABLING VERTIGO
│
↓
STEP 1: CONSERVATIVE MEDICAL THERAPY
• Low-salt diet (<1.5 g/day)
• Diuretics (hydrochlorothiazide/triamterene)
• Betahistine, vestibular suppressants
• Lifestyle modification
│
┌─────────┴──────────┐
│ │
CONTROLLED REFRACTORY
(Continue) (≥6 months)
│
↓
STEP 2: INTRATYMPANIC THERAPY
• IT Dexamethasone (if serviceable hearing)
• IT Gentamicin (vertigo-dominant, poor hearing)
│
┌────────┴────────┐
│ │
CONTROLLED FAILED
(Continue) │
↓
STEP 3: SURGICAL OPTIONS
┌──────────────────────────────┐
│ │
HEARING-PRESERVING ABLATIVE SURGERY
• Endolymphatic sac • Labyrinthectomy
decompression (no serviceable hearing)
• Vestibular neurectomy • Translabyrinthine
(retrosigmoid / middle approach
fossa)
IT Gentamicin vs. Other Modalities
| Feature | IT Gentamicin | IT Dexamethasone | ELS Decompression | Vestibular Neurectomy | Labyrinthectomy |
|---|---|---|---|---|---|
| Vertigo control | 80–90% | 40–60% | 50–70% | 90–95% | 95%+ |
| Hearing preservation | Moderate risk | Preserved | Preserved | Preserved | Destroyed |
| Invasiveness | Minimal | Minimal | Moderate | Major surgery | Major surgery |
| Anesthesia | Local | Local | General | General | General |
| Reversibility | Partial | Yes | Partial | No | No |
| Repeat possible | Yes | Yes | Limited | No | No |
| Hospital admission | Outpatient | Outpatient | Inpatient | Inpatient | Inpatient |
11. RECENT ADVANCES (Post-2015)
11A. Novel Drug Delivery Systems
- Thermosensitive hydrogels (poloxamer 407, chitosan-based): liquid at room temperature, gel in the middle ear → prolonged RWM contact, sustained release
- Nanoparticle-encapsulated gentamicin: liposomal and PLGA nanoparticles for controlled, targeted delivery
- Biodegradable microsphere systems: sustained release over days–weeks without repeated injections
- OTO-104 (sustained-release dexamethasone) has prompted similar sustained-release gentamicin formulation research
11B. Precision Dosing / Titration Endpoints
- Move toward objective audiometric titration rather than symptomatic endpoints
- Use of cervical VEMP (cVEMP) and ocular VEMP (oVEMP) as titration endpoint markers — monitors saccule/utricle function to guide dosing and stop before excessive toxicity
- Video Head Impulse Test (vHIT) as a real-time monitoring tool of semicircular canal function during titration
11C. Endolymphatic Hydrops Imaging
- Intratympanic gadolinium MRI (IT-Gd MRI) — 3D-FLAIR sequences 24 hours after IT gadolinium injection — allows direct visualization and grading of endolymphatic hydrops
- Can guide patient selection and assess treatment response
- Research role: correlating degree of hydrops with response to IT gentamicin
11D. Genetic Screening Before Treatment
- Screening for mitochondrial 12S rRNA A1555G mutation (mt.1555A>G) before IT gentamicin to identify patients at very high risk of profound HL
- May become standard pre-treatment workup
11E. Round Window Microcatheter Systems
- Continuous low-dose infusion (1 µL/hour) via implantable microcatheter
- Hoffer protocol: 10 mg/mL × 10 days — predictable pharmacokinetics, very low HL rate (1/36 patients)
- Major limitation: cost, surgical placement required
11F. Bilateral Ménière's Disease
- IT gentamicin in bilateral disease remains highly controversial
- Sequential bilateral treatment under careful monitoring with vHIT/VEMP is under investigation
- Bilateral vestibular loss leads to oscillopsia and severe dysequilibrium — major quality of life impact
- Cochlear implantation as rescue for profound bilateral HL post-gentamicin is now an established option
11G. Positive Predictive Factors (Research)
- Low pre-treatment caloric response predicts greater vestibular ablation
- Single-shot protocols showing comparable control to multi-shot in some RCTs (reduced HL)
- AAO-HNS guideline update (2020): IT gentamicin is now considered a second-line intervention after failure of IT steroids or medical therapy
12. COMPARISON OF TEXTBOOK PERSPECTIVES
| Textbook | Emphasis |
|---|---|
| Cummings Otolaryngology | Comprehensive protocol analysis (fixed/titrated/sustained-release); pharmacokinetics with RWM kinetics graph; dark cell theory; detailed complication management; outcome criteria |
| Scott Brown's Otolaryngology | Selective vestibulotoxicity concept; place in management algorithm for Ménière's disease; comparison with vestibular neurectomy |
| KJ Lee's Essential Otolaryngology | Listed under "vestibular ablative" procedures alongside vestibular neurectomy; concise indications and technique overview |
| Dhingra Diseases of ENT | Basic technique and indications; practical approach to patient selection; role in Indian ENT practice context |
| Hazarika ENT | IT gentamicin in context of Ménière's disease management algorithm; emphasis on hearing monitoring; newer delivery systems |
| Stell & Maran's Head & Neck Surgery | Surgical anatomy of RWM; comparison with surgical labyrinthectomy; complications |
| Zakir Hussain ENT | RGUHS-oriented concise approach; indications, technique, complications; integration with medical management |
13. SUMMARY FLOWCHART — IT GENTAMICIN DECISION & MONITORING
┌────────────────────────────────────────────────────────────┐
│ INTRATYMPANIC GENTAMICIN — COMPLETE PATHWAY │
└────────────────────────────────────────────────────────────┘
│
┌───────────────┼───────────────┐
↓ ↓ ↓
INDICATION WORKUP CONSENT
Intractable • Audiogram • Hearing loss risk
Ménière's • Caloric test • Disequilibrium
Unilateral • vHIT/VEMP • Chemical
Vertigo- • MRI brain labyrinthine upset
dominant • Genetic
screening
│
↓
PROTOCOL CHOICE
┌───────────────┼───────────────┐
↓ ↓ ↓
FIXED/SHOTGUN TITRATION SUSTAINED
(high ablation) (preferred) RELEASE
│
↓
INJECT: 0.4–0.5 mL
Gentamicin 40 mg/mL
(pH buffered to 6.4–7.4)
Postero-inferior TM
Patient positioning ×30 min
│
↓
MONITORING (weekly)
┌──────────────┬──────────────┐
↓ ↓ ↓
AUDIOGRAM VESTIBULAR VERTIGO
(PTA, SDS) FUNCTION DIARY
(caloric,
vHIT, VEMP)
│
┌───────────────┼────────────────┐
↓ ↓ ↓
VERTIGO SIGNIFICANT NO
CONTROLLED HEARING LOSS RESPONSE
│ (STOP) │
OBSERVE & Repeat injection
Rehab (up to 4 total)
│
Still no response
↓
SURGICAL OPTIONS
(Neurectomy/Labyrinthectomy)
14. IMPORTANT EXAM POINTS (RGUHS 50-Mark Focus)
-
Definition & principle: IT gentamicin = chemical ablation/subablation of the diseased labyrinth via transtympanic delivery to achieve vertigo control in intractable Ménière's disease
-
Mechanism: Preferential Type I hair cell damage + dark cell ionic disruption → reduces abnormal hydrops-induced impulses → vestibular compensation
-
Route: Tympanic membrane → middle ear → RWM → perilymph → inner ear (Type I > Type II vestibular hair cells damaged; cochlear cells relatively spared at low doses)
-
Drug concentration: 26.7–40 mg/mL (buffered with NaHCO₃ to pH 6.4–7.4)
-
Protocols: Fixed (shotgun — 4 consecutive days), Titration (weekly × 2–4), Sustained release (microcatheter/hydrogel)
-
Outcome criteria: AAO-HNS 1995 — Class A (complete control) to F
-
Complications: HL (0–30%), acute vestibular deafferentation, TM perforation, permanent disequilibrium, visual-vestibular mismatch
-
Contraindications: Only-hearing ear, contralateral vestibular deficit, mt.A1555G mutation, bilateral vestibular disease
-
Advantage over surgery: Outpatient, minimally invasive, repeatable, hearing-preserving potential, lower morbidity
-
Recent advances: vHIT/VEMP titration endpoints, IT-Gd MRI, thermosensitive hydrogels, nanoparticle delivery, genetic screening
References:
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed., Chapter 158 (IT Steroids & Gentamicin) & Chapter 167 (Ménière's Disease)
- KJ Lee's Essential Otolaryngology, 11th Ed.
- Scott Brown's Otolaryngology, 8th Ed.
- Dhingra — Diseases of ENT, Head & Neck
- Hazarika — Textbook of ENT Head & Neck Surgery
- Nedzelski JM et al. — Intratympanic gentamicin instillation, Laryngoscope 1992
- Hoffer ME et al. — Transtympanic vs. sustained-release gentamicin, Laryngoscope 111:1343, 2001
- AAO-HNS Committee on Hearing and Equilibrium guidelines, 1995
This is a shared conversation. Sign in to Orris to start your own chat.