mechanics and pathomechanics of lumbo sacral spine.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Searching the Web
lumbosacral spine mechanics pathomechanics biomechanics clinical
Now I have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Mechanics and Pathomechanics of the Lumbosacral Spine
1. Functional Anatomy of the Motion Segment
The functional unit (motion segment) consists of two adjacent vertebrae and the intervening soft tissues. Six degrees of freedom exist about all three axes. Movements include flexion/extension, lateral bending, and axial rotation - and these frequently occur in combination ("coupled motion").
Structural Components
| Structure | Role |
|---|---|
| Vertebral body | Transmits compressive loads; strength correlates with bone mineral content |
| Intervertebral disc | Shock absorption, load distribution, movement |
| Facet (zygapophysial) joints | Guide motion, resist torsion under axial loading |
| Ligaments | Passive restraints at end-range motion |
| Paraspinal muscles | Active dynamic stabilizers |
2. The Intervertebral Disc
The disc has two distinct zones with complementary mechanical roles:
- Annulus fibrosus - outer ring of collagen surrounding fibrocartilage arranged in a lamellar (concentric laminar) configuration. Fibers in alternate lamellae run at roughly 30 degrees in opposite directions. This arrangement limits rotation and resists tensile and shear stresses. Tensile stresses are highest here.
- Nucleus pulposus - central gelatinous mass, highly hydrated (up to 80% water in youth). Absorbs compressive loads and distributes them uniformly as hydrostatic pressure to the annulus and end plates. Compressive stresses are highest here.
The disc demonstrates viscoelastic behavior:
- Creep: deforms progressively under a sustained load (explains why we are slightly shorter at the end of the day)
- Hysteresis: absorbs energy during repeated axial loading (acts as a shock absorber), but this capacity decreases with repeated loading
Intradiscal pressure varies with posture:
- Lowest when lying supine
- Higher when standing
- Highest when sitting
- Increases further with bending and torsional stresses
- Loads are lowest when carried objects are close to the body
3. Lumbar Facet (Zygapophysial) Joints
The orientation of facets determines the direction and range of motion at each spinal level:
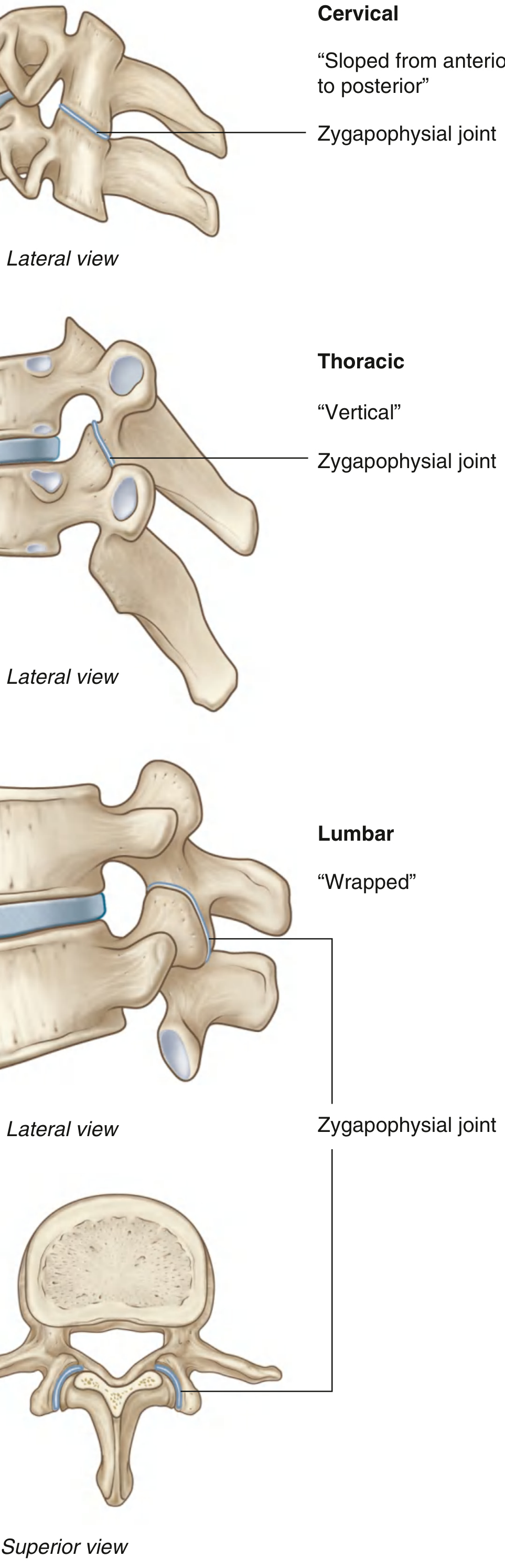
Lumbar facet orientation:
- 90 degrees to the transverse plane
- 50 degrees to the frontal plane ("wrapped" configuration)
- They progressively tilt upward (transverse) and inward (frontal) from L1 to L5
- This orientation permits flexion/extension and some lateral bending but severely limits axial rotation
At the lumbosacral joint (L5-S1): the facets have a more oblique orientation, allowing comparatively more rotation than the levels above. This joint also provides the most flexion/extension of any lumbar segment.
Torsional load resistance in the lumbar spine:
- Facets contribute 40%
- Disc contributes 40%
- Ligamentous structures contribute 20%
4. Range of Motion - Lumbar Spine
| Motion | Range per Segment | Notes |
|---|---|---|
| Flexion/Extension | 15-20° per level | Increases inferiorly; most occurs at L4-S1 |
| Lateral bending | 2-5° per level (lumbar) | Coupled with contralateral rotation |
| Axial rotation | 3-6° per level | Severely limited by facet orientation; most at L5-S1 |
Instant center of rotation lies within the disc annulus for lumbar segments.
The lumbosacral joint (L5-S1) accounts for approximately 70% of all lumbar flexion and offers more flexion/extension range than any other lumbar segment.
Coupled motion is a key concept - in the lumbar spine, lateral bending is coupled with contralateral rotation of the vertebral body (spinous processes deviate toward the concave side). Axial rotation couples strongly with lateral bending throughout the spine.
5. Sagittal Alignment
- Normal lumbar lordosis: 20-80 degrees (average ~60 degrees)
- Lordosis is created primarily by disc height and shape (wedge-shaped discs), not the vertebral bodies themselves
- Most lordosis occurs between L4 and S1
- The sacral base angle is approximately 30 degrees to the horizontal; the lumbosacral angle is approximately 140 degrees
Loss of disc space height leads directly to loss of lumbar lordosis.
Lumbar lordosis serves two mechanical functions:
- Shifts load posteriorly to the facets under extension loading
- Acts as a spring to absorb and distribute compressive forces
6. Ligamentous Support
Anterior supporting structures:
- Anterior longitudinal ligament (ALL) - strong, broad; resists hyperextension and anterior disc herniation
- Posterior longitudinal ligament (PLL) - narrower, weaker posteriorly; resists flexion and posterior disc herniation (but its weakness posterolaterally is why most disc herniations occur in that direction)
Posterior supporting structures:
- Ligamentum flavum (yellow ligament) - high elastin content; resists flexion; thickens with degeneration and contributes to canal stenosis
- Interspinous and supraspinous ligaments - resist flexion
- Capsular ligaments of facets - resist flexion; cervical disc injury commonly compromises these
7. Pathomechanics
A. Disc Herniation
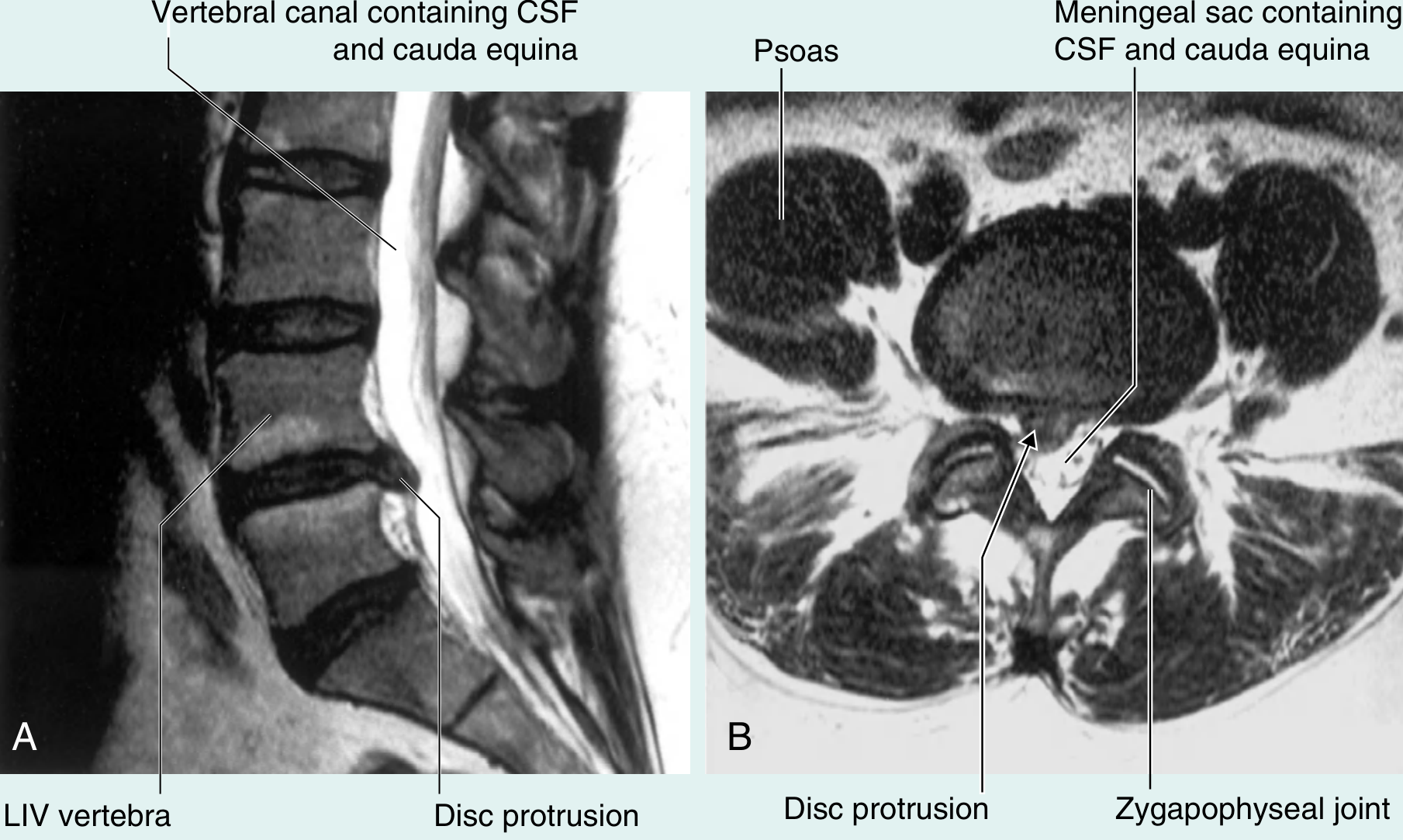
The sequence of events:
- Repeated torsional loading (shear forces) separates the nucleus pulposus from the annulus and end plate
- A tear develops in the annulus fibrosus (begins in the innermost lamellae and extends outward)
- Nuclear material is forced through the annular tear, particularly posterolaterally (the PLL is thinner and weaker here)
- The herniated material compresses adjacent nerve roots or the dural sac
90% of disc herniations occur at L4-L5 or L5-S1 - these levels carry the greatest mechanical load and have the most motion.
Clinical patterns:
- L4-L5 herniation - typically compresses the L5 nerve root (foot drop, weak dorsiflexion)
- L5-S1 herniation - typically compresses the S1 nerve root (diminished ankle jerk, weak plantarflexion)
- Central large herniation - can compress the cauda equina (cauda equina syndrome - a surgical emergency)
Flexion postures increase intradiscal pressure and potentiate herniation; extension reduces it. This is why patients with disc herniation are more comfortable standing or lying than sitting.
B. Lumbar Spinal Stenosis
Pathomechanical chain:
- Disc degeneration causes loss of disc height
- Loss of height shifts load toward facet joints (normally facets bear ~20% of axial load; with disc degeneration this increases)
- Facet joint arthropathy, osteophyte formation, and hypertrophy of ligamentum flavum follow
- Central canal, lateral recess, or foraminal stenosis results
- Neurogenic claudication: symptoms (buttock/leg pain, heaviness, paresthesias) reproduced by extension (canal narrows in extension) and relieved by flexion (canal widens) or sitting
C. Spondylolysis and Spondylolisthesis
- Spondylolysis is a stress fracture of the pars interarticularis (isthmus of the neural arch between superior and inferior facets)
- Mechanism: repetitive hyperextension with axial loading (e.g., gymnastics, fast bowling, weight lifting) - the L5 pars is the most vulnerable
- Fatigue loading (repetitive minor stresses) leads to pars fractures; this is distinct from acute traumatic fracture
- If bilateral spondylolysis disrupts the posterior arch, the anterior vertebral body can slip forward = spondylolisthesis
- Most common at L5-S1; forward slip (anterolisthesis) of L5 on S1
Grades of spondylolisthesis (Meyerding):
- Grade I: 0-25% slip
- Grade II: 25-50% slip
- Grade III: 50-75% slip
- Grade IV: 75-100% slip
D. Instability and Flatback Syndrome
- Iatrogenic flatback syndrome results from distraction forces applied to the lumbar spine (e.g., over-distraction during fusion instrumentation)
- Loss of normal lordosis increases anterior moment arm, increasing compressive load on discs and facets
- Translation in the lumbar spine: normal is < 2 mm; > 4 mm suggests clinical instability
E. Osteoporotic Fractures
- Vertebral body strength correlates with bone mineral content
- Osteoporosis causes loss of horizontal trabeculae (vertical trabeculae remain intact), dramatically reducing compressive strength
- Compression fractures typically occur at the vertebral end plate (the weakest zone mechanically)
- Load concentration at the anterior vertebral body in flexion makes anterior wedge fractures most common in the thoracolumbar junction (T12-L1)
F. Degenerative Disc Disease - Mechanical Cascade
The classic three-stage degenerative cascade (Kirkaldy-Willis):
- Dysfunction phase - disc dehydration and early annular tears; minor segmental hypermobility
- Instability phase - progressive disc collapse, facet capsule laxity, segmental instability with aberrant motion
- Stabilization/restabilization phase - osteophyte bridging, disc fibrosis, and spontaneous stabilization (often associated with reduced pain)
8. Summary Table: Key Mechanical Principles
| Principle | Detail |
|---|---|
| Primary lumbar motion | Flexion/extension (75%+ of trunk motion) |
| Most mobile lumbar segment | L5-S1 (lumbosacral) |
| Lordosis created by | Disc wedging (not vertebral body shape) |
| Disc pressure minimum | Supine |
| Disc pressure maximum | Sitting, especially with forward lean |
| Torsion resistance | Facets 40%, disc 40%, ligaments 20% |
| Facet orientation (lumbar) | 90° transverse / 50° frontal - limits rotation |
| Most common herniation level | L4-L5 and L5-S1 |
| Spondylolysis mechanism | Repetitive hyperextension - pars interarticularis fatigue fracture |
| Stenosis worsened by | Extension (canal narrows) |
| Stenosis relieved by | Flexion (canal widens) |
Sources: Miller's Review of Orthopaedics 9th Ed. | Gray's Anatomy for Students | Campbell's Operative Orthopaedics 15th Ed. | Gray's Anatomy for Students | Institute of Motion Spine Biomechanics; Springer Biomechanics of the Lumbar Spine
mechanics and pathomechanics of soft tissue
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
soft tissue mechanics pathomechanics collagen viscoelastic stress strain tendon ligament muscle cartilage clinical
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive textbook data from Miller's Review of Orthopaedics, Firestein & Kelley's Rheumatology, and supporting Stanford biomechanics data. Let me compile the full answer.
Mechanics and Pathomechanics of Soft Tissue
Soft tissues include muscle, tendon, ligament, articular cartilage, and the intervertebral disc. Each has a distinct composition, mechanical behavior, and failure pattern.
1. Fundamental Mechanical Concepts
Kinematics vs. Kinetics
- Kinematics = study of motion without regard to forces (position, displacement, velocity, acceleration)
- Kinetics = study of forces that cause motion (torques, loads, moments)
- In human movement, most motion is a combination of translation (rectilinear or curvilinear) and rotation, described as general motion
Degrees of Freedom
- A rigid body in 3-D space has 6 degrees of freedom: 3 translations (x, y, z) and 3 rotations (about each axis)
- Joint motion in clinical practice is usually simplified to describe the dominant angular displacement (flexion/extension, abduction/adduction, rotation)
Core Mechanical Concepts for Soft Tissue
| Term | Definition | Clinical significance |
|---|---|---|
| Stress | Force per unit area (N/m²) | Determines if tissue is overloaded |
| Strain | Deformation / original length (dimensionless %) | Quantifies how much tissue elongates |
| Stiffness | Force needed to produce a unit deformation | Slope of the linear region of load-deformation curve |
| Elastic modulus | Stress needed to produce unit strain | Intrinsic material property; 1.0-2.0 GPa for tendon/ligament |
| Creep | Progressive deformation under a constant load | Occurs in disc, tendon, ligament, cartilage |
| Stress relaxation | Decreasing stress when held at constant length | Basis for static stretching techniques |
| Hysteresis | Energy lost between loading and unloading curves | Energy is dissipated as heat |
2. Tendon
Structure and Composition
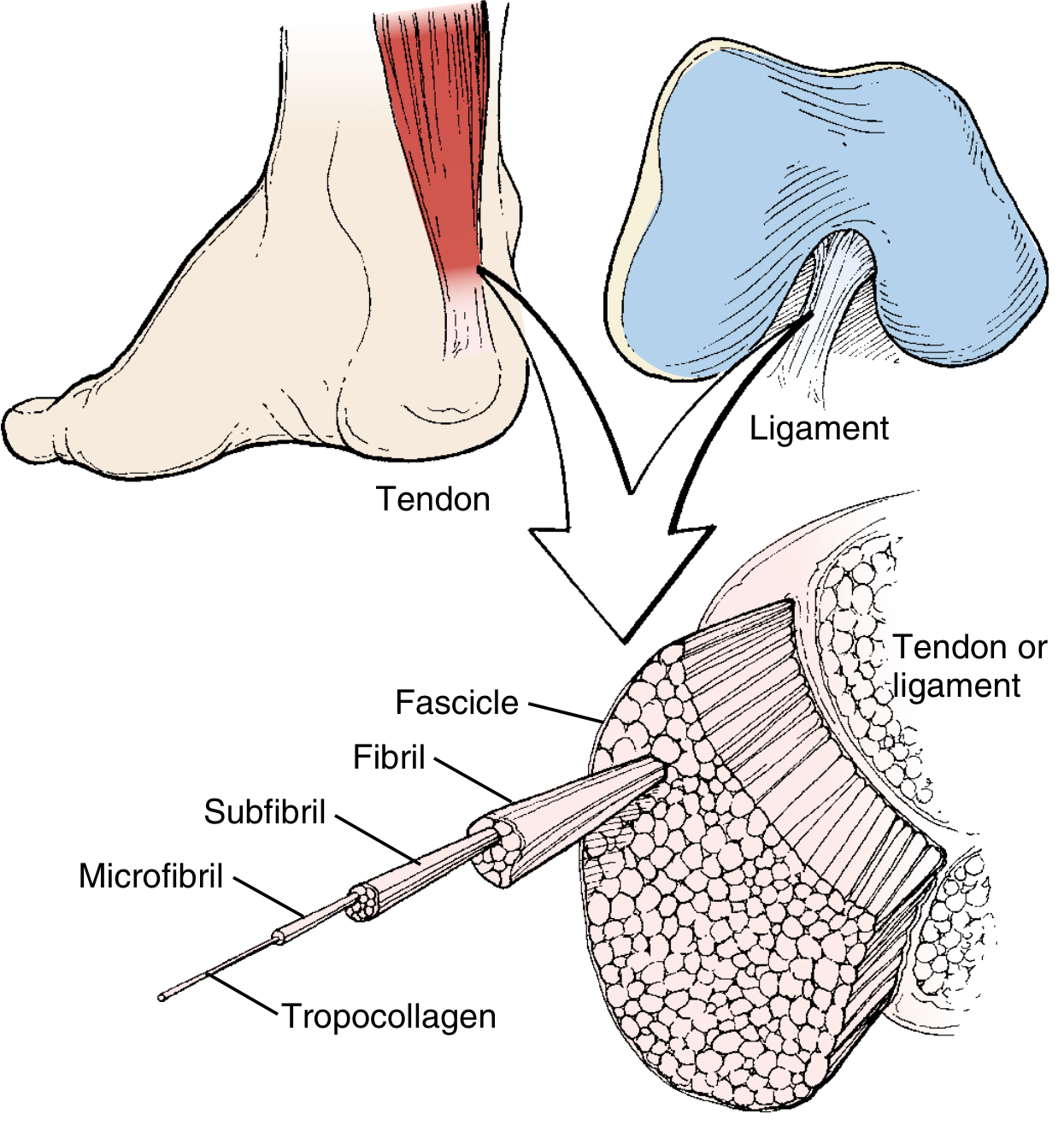
Collagen is organized in a strict hierarchy:
Tropocollagen → Microfibrils → Fibrils → Fascicles → Tendon
(each level surrounded by endotenon; entire tendon covered by epitenon/paratenon)
| Component | % of Dry Weight | Role |
|---|---|---|
| Type I collagen | 85% of dry weight (75% total) | Primary tensile load-bearer |
| Type III collagen | up to 5% | Present in endotenon; predominates after injury/repair |
| Elastin | 1-2% | Allows return to original shape; responsible for the "toe region" |
| Proteoglycans (decorin) | up to 5% | Regulates fibril diameter; cross-links collagen; anti-fibrotic (inhibits TGF-β1) |
| Aggrecan | at compression zones | Water retention at sites of tendon bending |
| Water | 50-60% total weight | Essential for viscoelastic behavior |
Tenocytes (fibroblasts) are the primary cells. They:
- Detect strain through deflection of cell cilia
- Synthesize ECM, collagen, and proteoglycans
- Produce type III collagen in response to rupture
- Produce MMPs (matrix metalloproteinases) for remodeling
Mechanical Properties
Tendons are:
- Anisotropic - properties vary with direction of load (strongest along fiber axis)
- Viscoelastic - properties vary with rate of load application
Stress-strain curve of tendon (4 regions):
Stress
| Failure
| /
| Linear /
| /region /
| / /
| Toe / /
| region / /
|_________/___________/_____ Strain
| 0-2% 2-4% 4-8%+
- Toe region (0-2% strain) - collagen fibers are normally "crimped" (wavy). Load straightens the crimp. Nonlinear, low stiffness. Elastin is responsible for this region. Normal physiologic loading occurs here.
- Linear region (2-4% strain) - collagen fibers are fully recruited and bear load. Stiffness is high and constant. Molecular cross-links are stressed.
- Yield/Plastic region (4-8% strain) - irreversible micro-failure begins. Fibers rupture progressively. Tissue does not return to original length on unloading.
- Failure region (>8% strain) - catastrophic rupture. Ultimate tensile strength of tendon: 50-100 MPa.
Ultimate tensile strain: 10-15%
Tendon Junctions
Myotendinous junction (MTJ):
- Actin microfilaments from the last Z-line link via sarcolemma to tendon collagen fibrils
- Site of maximum stress concentration during eccentric loading
- Most common site of muscle strains and tears
Bone-tendon (enthesis) junction - two types:
| Type | Mechanism | Location | Layers |
|---|---|---|---|
| Direct (fibrocartilaginous) | Gradual transition; 4 layers | High-load sites (rotator cuff, Achilles) | Tendon → Fibrocartilage → Mineralized fibrocartilage → Bone |
| Indirect | Sharpey fibers into periosteum | Most insertions | Superficial fibers into periosteum |
Tendon Blood Supply and Vulnerability
- Paratenon-covered tendons (Achilles, patellar): higher vascularity, better healing
- Sheathed tendons (digital flexors): blood supply via vincula; some nutrition from synovial diffusion
- Critical hypovascular zone: Achilles tendon is hypovascular 4-6 cm proximal to the calcaneal insertion - this is the site of most Achilles ruptures
Tendon Healing (3 Stages)
| Stage | Timing | Key Events | Collagen |
|---|---|---|---|
| Inflammation | Days 1-7 | Hematoma formation → resorption; tenocytes invade | Type III collagen begins |
| Proliferation | Weeks 2-6 | Maximal cellularity, maximal Type III production; weakest stage | Predominantly Type III |
| Remodeling/Maturation | 6 weeks onward | Decreased cellularity; Type III → Type I conversion | Type I predominates |
Post-repair strength:
- Weakest at 7-10 days post-repair
- Maximum strength at 6 months = two-thirds of original strength
- Early controlled motion and mechanical loading have beneficial effects on tenocyte function
- Immobilization decreases strength at the tendon-bone interface
3. Ligament
Structure and Composition
Ligaments are structurally similar to tendons but with key differences:
| Feature | Tendon | Ligament |
|---|---|---|
| Primary function | Transmits muscle force to bone | Stabilizes joints; prevents displacement |
| Collagen content | 75% dry weight (85% type I) | 70% dry weight type I (also III, V, VI) |
| Type III collagen | Up to 5% (endotenon) | More, especially midsubstance |
| Proteoglycans | Less | More (hence more water, more viscoelastic) |
| Fiber organization | Highly parallel, organized | Less organized, more cross-linked, intertwined |
| Vascularity | Variable (paratenon vs sheathed) | Uniform microvascularity via epiligamentous plexus |
| Additional function | - | Contains mechanoreceptors for proprioception |
Important addition: Ligaments contain both mechanoreceptors and free nerve endings. Loss of these during injury contributes to proprioceptive deficits and joint instability beyond mechanical laxity.
Ligament Injury Patterns
- Ligaments "break, not bend" - they do not plastically deform; they fail at their yield point
- Adults: midsubstance tears are more common
- Children: avulsion injuries are more common - failure typically occurs between unmineralized and mineralized fibrocartilage at the enthesis
Injury grading:
| Grade | Description | Instability |
|---|---|---|
| I (mild) | Microscopic tears; no elongation | None |
| II (moderate) | Partial macroscopic tear; some elongation | Mild-moderate |
| III (severe/complete) | Total rupture | Significant |
Ligament Healing (3 Stages)
| Stage | Timing | Events |
|---|---|---|
| Inflammatory | Days 0-7 | PMNs, then macrophages; Type III collagen and growth factors |
| Proliferative | Weeks 1-3 | Type III → Type I replacement begins; macrophages = weakest point |
| Remodeling/Maturation | Weeks 3-52+ | Scar remodeling; never fully recapitulates native collagen architecture |
Factors impairing ligament healing:
- Intraarticular injury (ACL heals poorly vs. MCL)
- Old age, smoking, NSAID use, diabetes mellitus, alcohol use
- Local corticosteroid injections
Factors improving healing (experimental):
- Extraarticular injury
- IL-10, IL-1 receptor antagonists
- Mesenchymal stem cells
- Collagen-PRP hydrogel scaffolds
4. Muscle
Structure
- Endomysium surrounds individual myofibers
- Perimysium surrounds muscle fascicles (groups of hundreds of fibers)
- Epimysium surrounds the entire muscle
- Sarcomere is the contractile unit (from Z-line to Z-line)
Sarcomere band structure:
| Band | Contents |
|---|---|
| A band | Actin + Myosin (overlap zone) |
| I band | Actin only |
| H band | Myosin only |
| M line | Interconnects thick (myosin) filaments |
| Z line | Anchors thin (actin) filaments |
Types of Muscle Contraction
| Type | Definition | Example | Notes |
|---|---|---|---|
| Isotonic concentric | Muscle shortens; tension constant | Biceps curl (up phase) | Generates force while shortening |
| Isotonic eccentric | Muscle lengthens during contraction; external force > internal force | Biceps curl (down phase) | Most efficient for strengthening; highest injury risk |
| Isometric | Length unchanged; tension generated | Pushing a wall | Static strength measurement |
| Isokinetic | Maximal contraction at constant velocity | Cybex machine | Best for maximizing strength |
Muscle Fiber Types
| Property | Type I (Slow-Twitch) | Type IIA (Fast Oxidative) | Type IIB (Fast Glycolytic) |
|---|---|---|---|
| Color | Red | White | White |
| Speed | Slow | Fast | Fast |
| Strength | Low | High | High |
| Fatigability | Resistant | Fatigable | Most fatigable |
| Aerobic capacity | High | Medium | Low |
| Motor unit size | Small | Larger | Largest |
Neuromuscular Stretch Receptors
- Muscle spindles (intrafusal fibers): detect muscle length; transmit to CNS; control muscle stiffness via the gamma motor system
- Golgi tendon organs (GTOs): at the myotendinous junction; detect tension; inhibit contraction to prevent excessive tendon lengthening (autogenic inhibition)
Pathomechanics: Muscle Strains
- Most common sports injury
- Occur primarily at the myotendinous junction (maximum stress concentration)
- Most common in two-joint muscles (hamstring, gastrocnemius, rectus femoris) with higher type II fiber content
- Precipitated by rapid eccentric contraction (highest force generation at longest length = maximum injury risk)
Mechanism of eccentric injury:
When a muscle is forced to lengthen while actively contracting (e.g., hamstring in late swing phase), the force-velocity relationship dictates that force exceeds the muscle's capacity, causing structural failure at the weakest point - the MTJ.
Healing cascade:
- Inflammation → fibrosis mediated by TGF-β
- Satellite cells act as stem cells - primary mechanism of muscle fiber regeneration
- Defect can also heal by bridging scar tissue (less functional)
Prevention: Pre-activation (stretching + warm-up) allows muscles to absorb twice the energy before failure.
Delayed Onset Muscle Soreness (DOMS)
- Occurs 24-72 hours after unaccustomed eccentric exercise
- Most common in type IIB fibers
- Mechanism: edema and inflammation in connective tissue; neutrophilic response; changes in the I-band of the sarcomere
- Treatment: NSAIDs relieve DOMS in a dose-dependent manner; other modalities (ice, ultrasound, electrical stimulation) have not been shown to affect DOMS
Immobilization Effects
- Atrophy results from disuse or altered recruitment
- Single-joint muscles atrophy faster than multi-joint muscles
- Sarcomeres at the myotendinous junction are especially affected
- Immobilization in lengthened positions decreases contractures and maintains strength better
- Electrical stimulation can offset atrophic effects
5. Articular Cartilage
Composition and Mechanical Role
| Component | % Wet Weight | Mechanical Function |
|---|---|---|
| Water | 60-80% | Provides hydraulic pressurization; enables load distribution |
| Type II collagen | ~15% wet weight | Tensile framework; restricts proteoglycan swelling |
| Proteoglycans (aggrecan) | ~10% wet weight | Highly hydrophilic; creates osmotic swelling pressure; compressive stiffness |
Articular cartilage functions as a biphasic material - the fluid phase (water) and solid phase (collagen-proteoglycan matrix) interact to distribute and absorb loads.
Mechanical Behavior
Cartilage is viscoelastic - under rapid loading, the fluid cannot escape quickly, making it very stiff. Under sustained loading, fluid gradually exudes (creep), allowing the tissue to deform.
Zones of articular cartilage (superficial to deep):
| Zone | Collagen orientation | Function |
|---|---|---|
| Superficial (tangential) | Parallel to surface | Resists shear forces |
| Transitional (middle) | Random | Transitional |
| Deep (radial) | Perpendicular to surface | Resists compressive forces |
| Calcified | Perpendicular | Anchors to subchondral bone |
Pathomechanics: Osteoarthritis
The degenerative cascade in cartilage:
- Proteoglycan loss → increased water content initially (cartilage appears "soft")
- Collagen framework disruption → fibrillation of the surface (earliest visible change)
- Loss of hydraulic pressurization → direct collagen-collagen contact; abrasive wear
- Chondrocyte death → reduced matrix synthesis; failure of repair mechanisms
- Aging effect: decreased water content of cartilage, reduced proteoglycan core proteins → reduced resiliency during joint loading
Key pathomechanical principle: Cartilage has no blood supply and very limited regenerative capacity. Once the collagen framework is disrupted beyond a critical threshold, repair does not restore normal mechanical properties.
6. Properties Comparison Summary
| Property | Tendon | Ligament | Muscle | Articular Cartilage |
|---|---|---|---|---|
| Primary collagen | Type I (85%) | Type I (70%) | Type I (endomysium/perimysium) | Type II |
| Tensile strength | 50-100 MPa | 50-100 MPa | Variable | 9-40 MPa |
| Ultimate strain | 10-15% | 10-15% | >50% (sarcomere) | 60-120% |
| Viscoelastic? | Yes | Yes | Yes (passive) | Yes |
| Primary cell | Tenocyte | Fibroblast | Myocyte + Satellite cells | Chondrocyte |
| Vascularity | Variable (zone-dependent) | Moderate | Rich | Avascular |
| Regeneration | Partial (scar) | Partial (scar) | Yes (satellite cells) | Minimal |
7. Key Pathomechanical Principles - Clinical Summary
| Principle | Implication |
|---|---|
| Viscoelasticity | Static stretching achieves creep elongation; warm-up reduces stiffness and injury risk |
| Toe region safety | Normal physiologic activity (0-2% strain) is self-protective; pathology occurs in linear/failure zones |
| Eccentric loading = highest risk | Hamstring strains, Achilles rupture, MTJ tears most common with rapid eccentric loads |
| Type III → Type I collagen transition | Healing tissue is weaker at 2-6 weeks; premature loading during proliferative phase risks re-rupture |
| ACL vs. MCL healing | Intraarticular ligaments heal poorly (ACL) due to synovial fluid inhibition; extraarticular (MCL) heal well conservatively |
| Avascular zones = rupture sites | Achilles (4-6 cm from calcaneus), supraspinatus, patellar tendon - hypovascular zones are most vulnerable |
| Cartilage degradation irreversibility | Loss of proteoglycans precedes and predicts irreversible collagen damage in OA |
| Immobilization paradox | Rest reduces inflammatory damage initially but prolonged immobilization causes atrophy, adhesions, and reduced mechanical properties in all soft tissues |
Sources: Miller's Review of Orthopaedics 9th Ed. | Firestein & Kelley's Textbook of Rheumatology | Bailey and Love's Short Practice of Surgery 28th Ed. | Stanford Biomechanics of Soft Tissue | Musculoskeletal Key - Ligament/Tendon Mechanics
This is a shared conversation. Sign in to Orris to start your own chat.