Q. Discuss the indications, pre-operative preparation, technique and complications of auditory brain-stem implantation.in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Searching Images
auditory brainstem implant ABI electrode cochlear nucleus fourth ventricle surgical technique
I now have all the material needed. Let me compile the comprehensive 50-mark answer.
AUDITORY BRAINSTEM IMPLANTATION (ABI)
A Comprehensive Discussion — 50 Marks
References: Cummings Otolaryngology (6e), Scott-Brown's Otorhinolaryngology, Stell & Maran, Dhingra, KJ Lee's Essential Otolaryngology, Hazarika, and recent literature
1. DEFINITION & CONCEPT
An Auditory Brainstem Implant (ABI) is a central neural auditory prosthesis that electrically stimulates the cochlear nucleus (CN) complex within the lateral recess of the fourth ventricle, thereby bypassing the entire peripheral auditory system — including the cochlea and auditory (cochlear) nerve. It is the next step beyond cochlear implantation for patients in whom peripheral stimulation is impossible.
"The ABI consists of a multielectrode surface array placed over the cochlear nucleus within the lateral recess of the fourth ventricle." — Cummings Otolaryngology, p. 3119
2. HISTORICAL BACKGROUND
| Year | Milestone |
|---|---|
| 1979 | First successful ABI by William House at the House Ear Institute, Los Angeles — platinum ball electrode pair in a 51-year-old NF2 patient |
| 1981 | Re-implantation with improved Dacron mesh electrode pads (1.7 × 2.0 mm platinum pads, 3.0 mm apart) to prevent migration |
| 1992 | Multichannel ABI introduced |
| 2000 | FDA approved multichannel ABI in NF2 patients ≥12 years |
| Early 2000s | Colletti extended ABI to non-tumor adults and children |
| 2013 | FDA-approved Investigational Device Exemption (IDE) for children with cochlear aplasia, ossification, or cochlear nerve aplasia |
| Present | >1000 ABI procedures performed worldwide |
3. ANATOMY OF TARGET SITE
The cochlear nucleus complex (CNC) lies within the dorsolateral brainstem at the pontomedullary junction. It is composed of:
- Dorsal Cochlear Nucleus (DCN)
- Anteroventral Cochlear Nucleus (AVCN)
- Posteroventral Cochlear Nucleus (PVCN)
The electrode is placed on the dorsal surface of the cochlear nucleus, accessible through the lateral recess of the fourth ventricle via the foramen of Luschka.
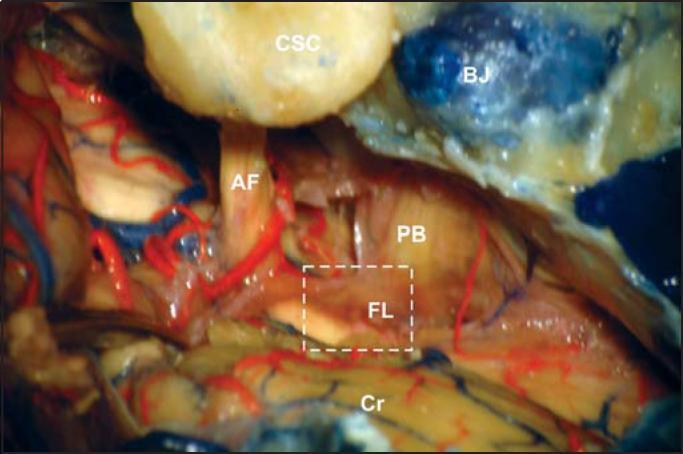
Key anatomical landmarks for electrode placement:
- Cranial nerves IX, X, XI (lower cranial nerves — inferolateral guide)
- Cranial nerves VII & VIII (acoustic-facial bundle — superior border)
- Foramen of Luschka (entry point into lateral recess)
- Anterior inferior cerebellar artery (AICA) — to be preserved
4. DEVICE HARDWARE
All ABIs share the same basic components as cochlear implants:
┌──────────────────────────────────────────────────────────────┐
│ ABI SYSTEM COMPONENTS │
├─────────────────────┬────────────────────────────────────────┤
│ EXTERNAL │ INTERNAL (implanted) │
├─────────────────────┼────────────────────────────────────────┤
│ Microphone │ Receiver/Stimulator (titanium housing) │
│ Speech Processor │ Electrode array (Dacron mesh paddle) │
│ Transmitter coil │ 12–21 active electrode contacts │
│ Battery │ Ground electrode (separate) │
└─────────────────────┴────────────────────────────────────────┘
- Electrode array: Flat paddle, 3 × 8 mm, 12–21 platinum disk electrodes on silicone + Dacron mesh backing
- The mesh allows suture fixation to prevent electrode migration
- Commercially available devices: Cochlear Corporation (Nucleus ABI), MED-EL (MAESTRO ABI), Oticon Medical (Digisonic SP ABI)
- Penetrating ABI (pABI): Experimental — intraneural penetrating electrodes to stimulate tonotopic layers within CN (not yet FDA approved)
5. INDICATIONS
5A. ESTABLISHED (FDA-APPROVED) INDICATIONS
Primary indication:
Neurofibromatosis Type 2 (NF2) — patients ≥12 years undergoing first- or second-side vestibular schwannoma removal
NF2 patients develop bilateral vestibular schwannomas that either cause cochlear nerve dysfunction directly or the nerve is sacrificed during surgery.
Algorithm for NF2 hearing rehabilitation:
NF2 Patient with Hearing Loss
│
▼
Cochlear nerve intact?
┌──────┴──────┐
YES NO
│ │
▼ ▼
Cochlear ABI at time of
Implant schwannoma
first removal
│
▼
Cochlear nerve
preserved but
non-functional?
│
▼
ABI (next step)
5B. EXPANDED (NON-NF2) INDICATIONS
| Category | Specific Conditions |
|---|---|
| Cochlear nerve absence/aplasia | Bilateral cochlear nerve aplasia or deficiency (congenital) |
| Cochlear ossification | Complete bilateral labyrinthine ossification (post-meningitis — especially streptococcal) unresponsive to cochlear implant |
| Cochlear malformations | Cochlear aplasia, common cavity deformity, Michel deformity |
| Traumatic | Bilateral temporal bone fractures with cochlear nerve avulsion |
| Cochlear implant failure | Patients with failed CI who have cochlear nerve dysfunction |
| Pediatric | Congenitally deaf children not candidates for CI during critical developmental window |
| CPA tumors (non-NF2) | Bilateral acoustic neuromas in non-NF2 setting, meningiomas, epidermoids of CPA |
Contraindications:
- Functioning cochlear nerve (CI preferred — superior outcomes)
- Unstable NF2 with multiple cranial tumors (high surgical risk)
- Severe medical co-morbidities
- Brainstem invasion by tumor at CN level
- Inability to cooperate with post-operative mapping/rehabilitation
- Patient/family with unrealistic expectations
6. CANDIDACY CRITERIA & SELECTION
CANDIDACY EVALUATION FLOWCHART
════════════════════════════════════════════════════════════
Patient referred for ABI
│
┌───────────▼───────────┐
│ Comprehensive │
│ Audiological │
│ Assessment │
└───────────┬───────────┘
│
┌───────────────▼───────────────┐
│ CI candidacy evaluation: │
│ - MRI cochlea/CN │
│ - CT temporal bones │
│ - EABR / ECAP testing │
└───────────────┬───────────────┘
│
CI possible and CN intact?
┌─────────┴──────────┐
YES NO
│ │
CI preferred ABI candidacy
│ │
▼ ┌─────▼─────────────────┐
CI trial 6 mos │ Multidisciplinary team│
│ │ - Neurotologist │
Adequate benefit? │ - Neurosurgeon │
┌────────┴───────┐ │ - Audiologist │
YES NO │ - Speech therapist │
│ │ │ - Psychologist │
Continue CI │ │ - Radiologist │
└─────┴─────────────────┘
│
ABI confirmed: Pre-op workup
════════════════════════════════════════════════════════════
7. PRE-OPERATIVE PREPARATION
7A. HISTORY AND PHYSICAL EXAMINATION
- Detailed otological and neurological history
- Family history of NF2
- Prior ear surgeries, radiation history
- Systemic co-morbidities (cardiovascular, coagulation disorders)
- Psychological assessment and counseling
7B. AUDIOLOGICAL ASSESSMENT
- Pure Tone Audiometry (PTA) — baseline bilateral thresholds
- Speech Audiometry — speech discrimination scores
- Auditory Brainstem Response (ABR) — wave V absent → cochlear nerve non-functional
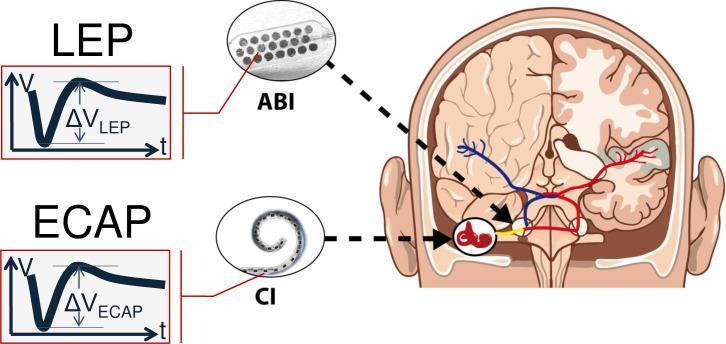
- Electrically Evoked Auditory Brainstem Response (EABR) — promontory stimulation to assess central pathway integrity (CN and beyond)
- Otoacoustic Emissions (OAE)
- Aided audiometry with best hearing aids
If EABR is present at promontory stimulation but no auditory nerve function, this confirms central (CN) pathways are intact → ABI will likely yield benefit
7C. IMAGING
| Investigation | Purpose |
|---|---|
| MRI with contrast (brain + IAC) | Define tumor size, CN anatomy, brainstem morphology, cochlear nerve presence |
| HRCT Temporal Bones | Cochlear anatomy, ossification, surgical planning |
| MRI Cochlear Nerve Protocol (3D CISS/FIESTA) | Specific CN visualization |
| MRI Cochlear Nucleus | Rule out brainstem invasion by tumor at CN level |
7D. MEDICAL & SURGICAL PREPARATION
- Coagulation profile (PT, aPTT, platelet count), CBC, blood group
- Cardiac evaluation — ECG, echocardiogram if needed
- Anaesthetic fitness — neurological co-morbidities
- Anti-epileptic medications — review pre-operatively
- Steroid protocol — perioperative dexamethasone to reduce brainstem edema
- Antibiotic prophylaxis — standard craniotomy regimen
- Shaving and scalp preparation — retrosigmoid region
- Informed consent — detailed counseling on realistic outcomes, risks of non-auditory stimulation, CSF leak, cranial nerve palsies
7E. PRE-OPERATIVE COUNSELING (Critical)
Patients and families must understand:
- ABI provides sound awareness not normal hearing in most cases
- Outcomes are highly variable and inferior to cochlear implants
- ABI aids lip-reading and environmental awareness
- Extensive post-operative rehabilitation and mapping sessions are required
- NF2 patients may have additional CNS burdens affecting outcomes
7F. TEAM PREPARATION
- Intraoperative neurophysiology monitoring team (electrophysiologist)
- Neurosurgeon + Otologist — dual surgical team
- Manufacturer representative — for device programming
- Equipment: ABI device, intraoperative electrophysiology unit, operating microscope, neurophysiologic monitoring (CMAP for CN IX, X; BAEP)
8. SURGICAL TECHNIQUE
8A. APPROACHES TO THE COCHLEAR NUCLEUS
Three main surgical approaches are used:
| Approach | Advantages | Disadvantages | When Used |
|---|---|---|---|
| Translabyrinthine (TL) | Gold standard for NF2; direct access to CPA; excellent CN identification | Destroys residual hearing | NF2 patients with non-serviceable hearing |
| Retrosigmoid (RS) | Hearing preservation possible; familiar to neurosurgeons | Less direct access to lateral recess; higher cerebellar retraction | Non-NF2 adults, bilateral cases, pediatric |
| Middle Fossa | Hearing preservation | Limited access to CN | Rarely used for ABI |
8B. STEP-BY-STEP OPERATIVE TECHNIQUE (Translabyrinthine Approach)
Patient Positioning:
- Supine with head turned 30–45° away from operative side
- Alternatively: lateral decubitus (park bench) position
- Head fixed in Mayfield/Gardner-Wells tongs
- Neurophysiology monitoring electrodes applied (EEG, CMAP for CN IX, X, XI)
Incision and Exposure:
- C-shaped retroauricular incision
- Cortical mastoidectomy
- Complete labyrinthectomy → removal of cochlea, vestibule, semicircular canals
- Identify and skeletonize the sigmoid sinus
- Expose the posterior fossa dura posterior to sigmoid sinus
- Identify jugular bulb, posterior semicircular canal, and the internal auditory canal (IAC)
- Dural incision — L-shaped or T-shaped opening of posterior fossa dura
CPA Exposure:
8. Gentle cerebellar retraction with cottonoid pledgets
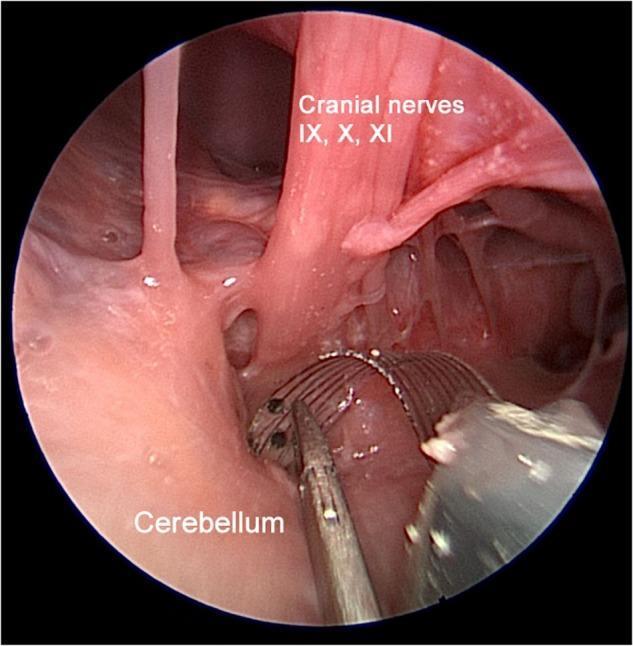
9. Identify the lower cranial nerves (IX, X, XI) — key landmark
10. Identify the facial nerve (VII) and vestibulocochlear nerve (VIII) — acoustic-facial bundle
11. Identify the foramen of Luschka — opening of the lateral recess of fourth ventricle, located between the acoustic-facial bundle above and the lower cranial nerves below
12. Tumor removal (in NF2) — careful dissection to preserve brainstem
13. Identify the cochlear nucleus — lies within the dorsal lateral pontine surface just medial to CN VIII entry zone
Electrode Placement (Critical Step):
ELECTRODE PLACEMENT SEQUENCE
════════════════════════════════════════════
1. Remove any CSF, blood, and cottonoids
from the lateral recess
│
▼
2. Gently open the foramen of Luschka with
a fine hook or suction irrigator
│
▼
3. Insert electrode paddle into lateral
recess with smooth forceps or stylet
│
▼
4. INTRAOPERATIVE ELECTROPHYSIOLOGY:
- Electrically Evoked Auditory Brainstem
Response (EABR) — confirm cochlear
nucleus stimulation
- EABR waves III and V must be present
- Test for non-auditory stimulation
(check for facial twitch, shoulder
elevation → CN IX, X, XI activation)
│
▼
5. Optimize electrode position until EABR
is maximal and non-auditory stimulation
is minimized
│
▼
6. Secure electrode array:
- Dacron mesh sutured to dura/fibrous
tissue at lateral recess with 4-0
Prolene or titanium clips
- Tie-down suture through mesh holes
════════════════════════════════════════════
Receiver/Stimulator Placement:
14. Create a bony well in the skull (posterior to the mastoid) using a cutting bur — 5–6 mm depth, size of receiver package
15. Place receiver/stimulator in the bony well and suture to periosteum via titanium screws or mesh
16. Route electrode cable under posterior scalp flap through a bony channel to the mastoid and into the CPA
Closure:
17. Fill the mastoid and middle ear cavity with abdominal fat graft
18. Muscle and fascial closure in layers
19. Skin closure
8C. INTRAOPERATIVE ELECTROPHYSIOLOGY — EABR CRITERIA
| EABR finding | Significance |
|---|---|
| Clear waves III and V | Electrode correctly on CN; central pathways intact |
| No response | Electrode not on CN; reposition needed |
| Only wave I/II | Peripheral nerve stimulation — not CN |
| Facial/shoulder movement at low current | Non-auditory stimulation of adjacent CN IX/X/XI |
9. POST-OPERATIVE MANAGEMENT
Immediate (0–2 weeks):
- ICU monitoring for 24–48 hours
- Neurological observations — level of consciousness, cranial nerve function
- Head of bed elevated 30–45°
- Monitor for CSF leak, wound dehiscence
- Corticosteroids (dexamethasone) — prevent brainstem edema
- Antiemetics — post-craniotomy nausea
- Pain management
- Early ambulation
Device Activation (4–6 weeks post-op):
- Initial programming (mapping) session by audiologist
- Electrical thresholds (T-levels) and comfort levels (C-levels) established per electrode
- Non-auditory stimulation channels identified and deactivated
- Multiple sessions over months required to optimize MAP
Rehabilitation:
- Auditory training
- Speech reading support
- Communication therapy
- Regular audiological follow-up
10. OUTCOMES
Performance Levels (Variable spectrum):
ABI PERFORMANCE SPECTRUM
═══════════════════════════════════════════════════════════
POOR MODERATE GOOD
←───────────────────────────────────────────────────────→
Environmental Enhanced Open-set
sound awareness lipreading speech
only recognition
(~20–30%) (~40–50%) (~10–20%)
═══════════════════════════════════════════════════════════
NF2 Adults: Most achieve enhanced lip-reading and environmental awareness; <10% achieve open-set speech recognition without visual cues. Mean CAP scores ~2–3.
Non-NF2 Children (Colletti's series): Up to 70–80% achieve open-set speech recognition — outcomes approach cochlear implant performance in some. This is because non-tumor children lack the central auditory pathway damage seen in NF2.
Pediatric ABI: Best results when implanted <3.5 years (during critical period of auditory pathway development).
11. COMPLICATIONS
11A. INTRAOPERATIVE
| Complication | Mechanism | Prevention |
|---|---|---|
| Brainstem injury | Retraction, ischemia | Gentle retraction, bipolar hemostasis |
| Lower cranial nerve palsy (IX, X, XI) | Direct trauma | Careful anatomy, neurophysiologic monitoring |
| Facial nerve injury | Translabyrinthine dissection | Facial nerve monitoring (EMG) |
| AICA injury | Vascular injury | Meticulous dissection |
| Air embolism | Venous sinus injury | Head position, Valsalva testing |
| Electrode misplacement | CN not identified | Intraoperative EABR |
11B. EARLY POST-OPERATIVE
| Complication | Incidence | Management |
|---|---|---|
| CSF leak | 5–15% | Pressure dressing, lumbar drain, revision closure |
| Meningitis | 1–3% | Antibiotics, CSF analysis |
| Wound infection/dehiscence | 1–5% | Antibiotics, surgical debridement |
| Headache | Common | Analgesics, CSF leak rule-out |
| Dysphagia/dysphonia | CN IX/X injury | Swallowing therapy, nasogastric feeding |
| Balance disturbance | Cerebellar/labyrinthine | Vestibular rehabilitation |
11C. DELAYED / DEVICE-RELATED
| Complication | Description |
|---|---|
| Non-auditory stimulation | Most common functional complication — tingling, dizziness, pain, shoulder movement → caused by current spread to adjacent CN IX, X, XI; managed by switching off offending channels |
| Electrode migration | Paddle slips out of lateral recess → loss of benefit; prevented by Dacron mesh fixation |
| Device failure | Hardware malfunction requiring re-implantation |
| Meningitis (late) | Device-related → bacterial seeding |
| Extrusion | Rare — implant body erosion through skin |
| No auditory benefit | 10–30% get no useful hearing — central pathway limitations |
Complication Summary Table (Cummings):
MOST COMMON ABI COMPLICATIONS
══════════════════════════════════════════════
1. Non-auditory stimulation ← MOST COMMON
(facial twitch, parasthesia)
2. CSF leak
3. Electrode migration
4. Lower cranial nerve dysfunction
5. No auditory benefit
══════════════════════════════════════════════
12. SPECIAL CONSIDERATIONS IN PEDIATRIC ABI
From Cummings Otolaryngology (Block 37, pp. 3119–3210):
- Retrosigmoid approach preferred in children (avoids labyrinth, allows bilateral future access)
- Cochlear nucleus is proportionally smaller — electrode placement technically demanding
- Imaging critical — MRI for CN aplasia vs. hypoplasia vs. cochlear aplasia
- Outcomes superior to NF2 adults — up to 80% gain open-set speech in non-tumor children
- Age at implantation critical: best outcomes if implanted <2–3.5 years (critical period)
- Must coordinate with neurosurgeon experienced in pediatric posterior fossa surgery
13. RECENT ADVANCES
| Advance | Details |
|---|---|
| Penetrating ABI (pABI) | Intraneural penetrating electrode arrays to stimulate tonotopic layers within CN — improved frequency resolution; in clinical trials |
| Flexible Electrode Arrays | Polyimide-substrate conformable arrays that better match CN curvature — improved electrode-tissue interface and tonotopic stimulation |
| Expanded indications | ABI in cochlear nerve deficiency (CND) — previously thought to be CI territory |
| Simultaneous CI + ABI | In NF2 — translabyrinthine schwannoma removal with simultaneous ABI placement; or cochlear implantation in preserved nerve ear alongside ABI in other |
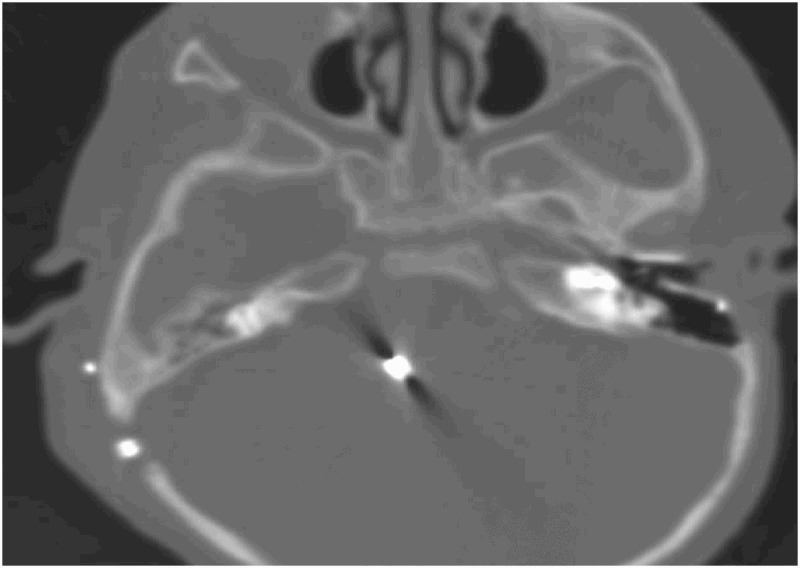
| Intraoperative imaging | Intraoperative CT/MRI to confirm electrode placement |
| Speech coding improvements | Fine structure processing, spectral coding strategies improve frequency discrimination |
| Central auditory midbrain implant (AMI) | Stimulation of inferior colliculus — investigated in patients where CN is destroyed; fewer active channels but promising early results |
| Machine learning mapping | AI-assisted audiological programming for faster, more precise fitting sessions |
| Bilateral ABI | Growing evidence for bilateral simultaneous ABI in suitable NF2 patients |
14. COMPARISON: ABI vs. COCHLEAR IMPLANT
| Feature | Cochlear Implant (CI) | ABI |
|---|---|---|
| Site of stimulation | Cochlea (spiral ganglion) | Cochlear nucleus (brainstem) |
| Prerequisite | Intact cochlear nerve | CN functional, CI not possible |
| Audiological outcomes | Excellent (80–90% open-set speech) | Variable (10–30% open-set speech) |
| Speech recognition | High | Low–moderate in NF2; better in non-NF2 children |
| Surgical approach | Cochleostomy via mastoid | Retrosigmoid or translabyrinthine craniotomy |
| Risk | Low (cochlear surgery) | Higher (posterior cranial fossa) |
| First choice | Yes, if cochlear nerve intact | Only if CI not possible |
15. COMPREHENSIVE FLOWCHART SUMMARY
COMPLETE ABI MANAGEMENT FLOWCHART
═══════════════════════════════════════════════════════════════════
INDICATION CONFIRMED (NF2 or non-NF2 non-CI candidate)
│
┌────────────────▼────────────────┐
│ PRE-OPERATIVE WORKUP │
│ • Audiometry / EABR │
│ • MRI (CN anatomy, brainstem) │
│ • HRCT (temporal bone) │
│ • Multidisciplinary assessment │
│ • Counselling & consent │
└────────────────┬────────────────┘
│
┌────────────────▼────────────────┐
│ SURGICAL APPROACH │
│ NF2 → Translabyrinthine (TL) │
│ Non-NF2/Child → Retrosigmoid │
└────────────────┬────────────────┘
│
┌────────────────▼────────────────┐
│ INTRAOPERATIVE STEPS │
│ 1. CPA exposure │
│ 2. Tumour removal (NF2) │
│ 3. Identify foramen of Luschka │
│ 4. Electrode placement in │
│ lateral recess (CN surface) │
│ 5. EABR confirmation │
│ (waves III + V present) │
│ 6. Adjust if non-auditory stim │
│ 7. Secure with Dacron suture │
│ 8. Receiver in bony well │
└────────────────┬────────────────┘
│
┌────────────────▼────────────────┐
│ POST-OPERATIVE CARE │
│ • ICU 24–48h │
│ • Steroids, antibiotics │
│ • CSF leak surveillance │
└────────────────┬────────────────┘
│
┌────────────────▼────────────────┐
│ DEVICE ACTIVATION (4–6 weeks) │
│ • Audiological mapping (T & C │
│ levels per electrode) │
│ • Non-auditory channels OFF │
│ • Multiple mapping sessions │
└────────────────┬────────────────┘
│
┌────────────────▼────────────────┐
│ REHABILITATION │
│ • Auditory training │
│ • Lipreading support │
│ • Speech therapy │
│ • Long-term follow-up │
└─────────────────────────────────┘
═══════════════════════════════════════════════════════════════════
16. KEY EXAMINATION POINTS (RGUHS 50-mark focus)
- ABI = central neural prosthesis stimulating cochlear nucleus directly
- Primary indication = NF2 ≥12 years (FDA-approved); CI always preferred if nerve intact
- Target = lateral recess of fourth ventricle via foramen of Luschka
- EABR intraoperatively = mandatory to confirm correct placement (look for waves III and V)
- Non-auditory stimulation = most common complication (CN IX/X/XI current spread)
- CSF leak = most common surgical complication
- Translabyrinthine = approach of choice for NF2; Retrosigmoid for non-NF2/pediatric
- Outcomes in non-NF2 children are superior to NF2 adults (intact central pathways)
- Recent advances: penetrating ABI, flexible arrays, AMI (auditory midbrain implant)
- Device components: microphone → speech processor → transmitter coil → receiver/stimulator → 12–21 electrode paddle on Dacron mesh
Primary References:
- Cummings Otolaryngology Head and Neck Surgery (6e), Chapter 163 — Auditory Brainstem Implantation, pp. 3119–3210 (Choudhury, Deep, Wilkinson, Roland)
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery — Volume 3, Cochlear Implants chapter
- KJ Lee's Essential Otolaryngology (10e)
- Dhingra PL — Diseases of Ear, Nose and Throat
- Hazarika P — Textbook of Ear, Nose and Throat
- Brackmann DE et al., Otolaryngol Head Neck Surg 1993 — original ABI surgical technique
- Colletti V et al., Laryngol Otol 2000 — Retrosigmoid approach for ABI
- Otto SR et al., Arch Otolaryngol 2004 — ABI in adolescents
- Lenarz M et al., Otol Neurotol 2002 — subjective outcomes
This is a shared conversation. Sign in to Orris to start your own chat.