Sensenural hearing loss cause
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile the answer.
Sensorineural Hearing Loss (SNHL) — Causes
Sensorineural hearing loss results from damage to the mechanotransduction apparatus of the cochlea or disruption of the electrical conduction pathway from the inner ear to the brain. This accounts for ~90% of all hearing loss. Injury can involve hair cells, supporting cells, auditory neurons, or the central auditory pathway.
Structural Basis
| Site of Damage | Consequence |
|---|---|
| Cochlear hair cells (organ of Corti) | Most common — loss of mechano-electrical transduction |
| Cochlear division of CN VIII | Neural SNHL |
| Central auditory pathways / cortex | Central SNHL |
Causes — By Category
1. Noise-Induced (Acoustic Trauma)
- Prolonged or intense noise exposure damages hair cells
- Produces a characteristic "noise notch" at 4000–5000 Hz on audiogram
- Can also cause cochlear synaptopathy ("hidden hearing loss") — normal pure-tone audiometry but difficulty hearing in background noise, due to loss of auditory synapses rather than hair cells
2. Age-Related (Presbycusis)
- Progressive loss of sensory hair cells and nerve fibers starting at the basal turn of the cochlea (high-frequency region), progressing apically
- Most common cause of SNHL in older adults
- Presents as high-frequency hearing loss
3. Ototoxic Drugs
| Drug Class | Examples |
|---|---|
| Aminoglycoside antibiotics | Gentamicin, tobramycin, streptomycin |
| Loop diuretics | Furosemide, ethacrynic acid |
| Salicylates | High-dose aspirin |
| Antimalarials | Quinine and synthetic analogues |
| Chemotherapeutic agents | Cisplatin |
4. Infectious
- Viral labyrinthitis (mumps, CMV, herpes zoster — Ramsay Hunt syndrome)
- Meningitis (bacterial — direct spread to cochlea via CSF pathways)
- Chronic otitis media (may damage cochlea directly or via toxins)
- Infections of the membranous labyrinth
5. Vascular / Sudden SNHL
- Sudden SNHL — often idiopathic; presumed vascular or viral etiology; unilateral, acute onset; medical emergency
- Stroke — affecting central auditory pathways
6. Tumors
- Vestibular schwannoma (acoustic neuroma) — most important cause of unilateral SNHL; asymmetric SNHL is the hallmark
- Meningioma — cerebellopontine angle
- Endolymphatic sac tumor
- Other CNS tumors
7. Endolymphatic Hydrops — Ménière's Disease
- Fluctuating low-frequency SNHL, tinnitus, episodic vertigo, and aural fullness
- Due to excess endolymph causing distension of the membranous labyrinth
8. Congenital / Genetic
- Congenital inner ear malformations (Mondini deformity, enlarged vestibular aqueduct)
- Genetic mutations: > 100 genes implicated; connexin 26 (GJB2) mutations are the most common cause of congenital SNHL
- Can be syndromic (Usher, Waardenburg, Pendred, Alport) or non-syndromic
- Genetic predisposition may interact with environmental exposures
9. Autoimmune
- Immune-mediated SNHL — one of the few treatable causes of SNHL; bilateral, progressive, often responds to corticosteroids
10. Trauma
- Temporal bone fracture — transverse fractures typically cause SNHL; longitudinal may cause conductive
- Head trauma with perilymphatic fistula
11. Neurological / Demyelinating
- Multiple sclerosis — lesions in central auditory pathways
- Any CNS infection (encephalitis, meningitis)
12. Radiation Therapy
- Cochlear radiation damage following head/neck radiotherapy
Key Clinical Distinction: Asymmetric SNHL
Asymmetric SNHL has very few causes other than vestibular schwannoma. Ménière's disease is in the differential but can usually be distinguished clinically. Any asymmetric SNHL warrants MRI of the internal auditory canals. — Rosen's Emergency Medicine
Sources: Harrison's Principles of Internal Medicine 22E, p. 289 | Histology: A Text and Atlas (Gartner), p. 2476 | Cummings Otolaryngology Head and Neck Surgery
How to undestand audiogram
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Here is a comprehensive guide to reading and interpreting an audiogram.
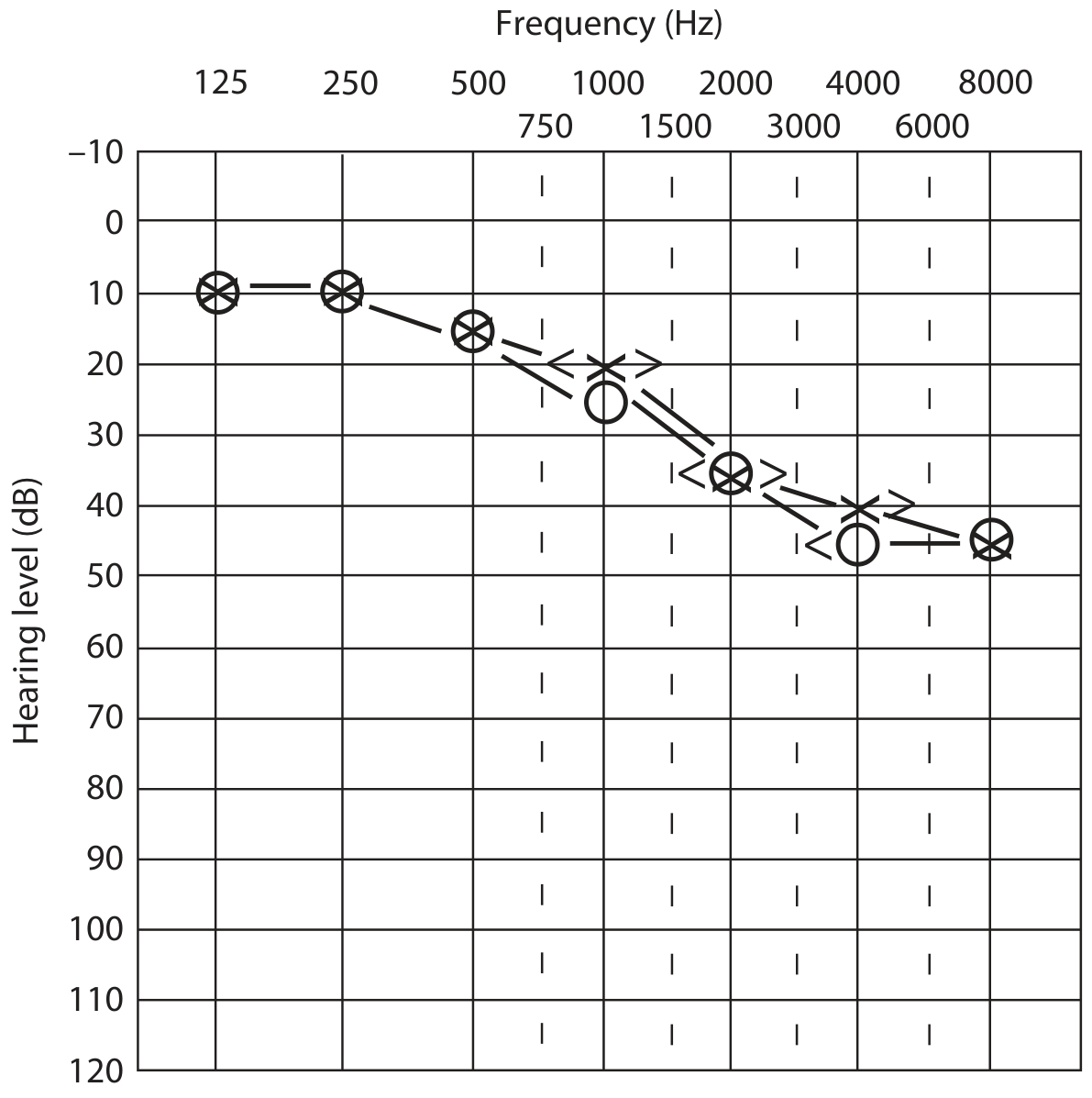
How to Understand an Audiogram
An audiogram is a graph that plots a person's hearing sensitivity to pure tones as a function of frequency. It is the foundation of audiometric assessment.
The Grid
| Axis | What it represents |
|---|---|
| Horizontal (X-axis) | Frequency in Hz — from low (125 Hz) to high (8000 Hz); left = low pitch, right = high pitch |
| Vertical (Y-axis) | Hearing level in dB HL — 0 at top (normal/quiet), increases downward (louder sound needed) |
Key point: Down = worse hearing. A point plotted lower on the graph means the patient needed a louder sound to hear it.
Severity of Hearing Loss
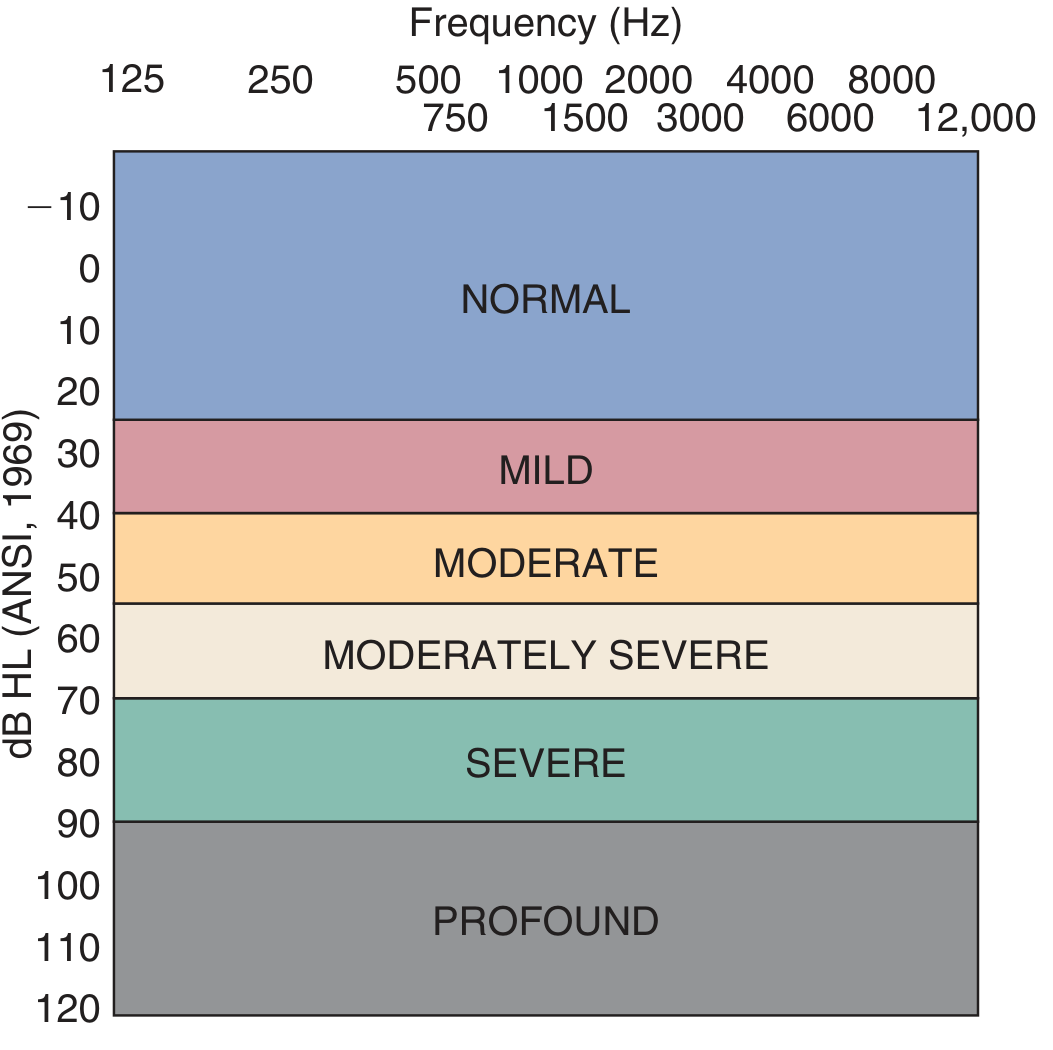
| dB HL Threshold | Degree |
|---|---|
| ≤ 25 dB | Normal (adults); ≤ 15 dB in children |
| 26–40 dB | Mild |
| 41–55 dB | Moderate |
| 56–70 dB | Moderately Severe |
| 71–90 dB | Severe |
| > 90 dB | Profound |
Symbols Used on an Audiogram
| Symbol | Meaning | Ear |
|---|---|---|
| O | Unmasked air conduction | Right |
| X | Unmasked air conduction | Left |
| Δ | Masked air conduction | Right |
| □ | Masked air conduction | Left |
| < | Unmasked bone conduction | Right |
| > | Unmasked bone conduction | Left |
| [ | Masked bone conduction | Right |
| ] | Masked bone conduction | Left |
By convention: Red = Right ear, Blue = Left ear.
Air Conduction vs. Bone Conduction
Air conduction (AC): Sound travels through the ear canal → tympanic membrane → ossicles → cochlea → auditory nerve. Tests the entire hearing system.
Bone conduction (BC): A vibrator on the mastoid process sends vibrations directly to the cochlea, bypassing the outer and middle ear. Tests the inner ear and auditory nerve only.
Air-bone gap (ABG): When AC thresholds are worse (lower on the graph) than BC thresholds, there is a gap. This means the outer or middle ear is not conducting sound efficiently but the cochlea is intact.
The Four Audiogram Patterns
1. Normal Hearing
Both AC and BC thresholds ≤ 25 dB HL across all frequencies.
2. Conductive Hearing Loss
- AC elevated (shifted down on graph)
- BC normal (at top of graph)
- Air-bone gap present
- Cause: outer or middle ear problem (e.g., otitis media, otosclerosis, cerumen)
3. Sensorineural Hearing Loss (SNHL)
- Both AC and BC equally elevated — they overlap, no air-bone gap
- Cause: cochlea, auditory nerve, or central auditory pathway
4. Mixed Hearing Loss
- Both AC and BC elevated, but AC is worse than BC
- Air-bone gap is present, but BC is also not normal
- Cause: conductive pathology superimposed on sensorineural pathology
Configuration (Shape) of the Audiogram
The shape gives clues about etiology:
| Configuration | Description | Classic Cause |
|---|---|---|
| Flat | Equal loss across all frequencies | Otosclerosis, some SNHL |
| Sloping / High-frequency | Normal low-freq, loss at high freq | Presbycusis, noise-induced |
| Falling | Progressive drop toward high freq | Age-related, ototoxicity |
| Notched | Dip at 4000 Hz, recovers at 8000 Hz | Noise-induced hearing loss |
| Rising | Worse at low frequencies | Ménière's disease |
| Saucer-shaped | Better at high and low, worse in mid | Various |
Pure-Tone Average (PTA)
The PTA is the average threshold at 500, 1000, and 2000 Hz — the speech frequencies. It summarizes the degree of hearing loss in a single number and should correlate with the patient's speech perception ability.
In Summary: A 4-Step Approach
- Look at the thresholds — are they in the normal zone (top 25 dB)?
- Compare AC and BC — is there an air-bone gap?
- Classify the type — conductive / SNHL / mixed
- Describe the configuration — flat, sloping, notched, etc., and identify the frequency range affected
Sources: K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology Head and Neck Surgery; Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.