Facial nerve
Reading File
Finding Sources
Searching Images
facial nerve anatomy branches
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Here is a complete overview of the Facial Nerve (CN VII):
Facial Nerve (CN VII)
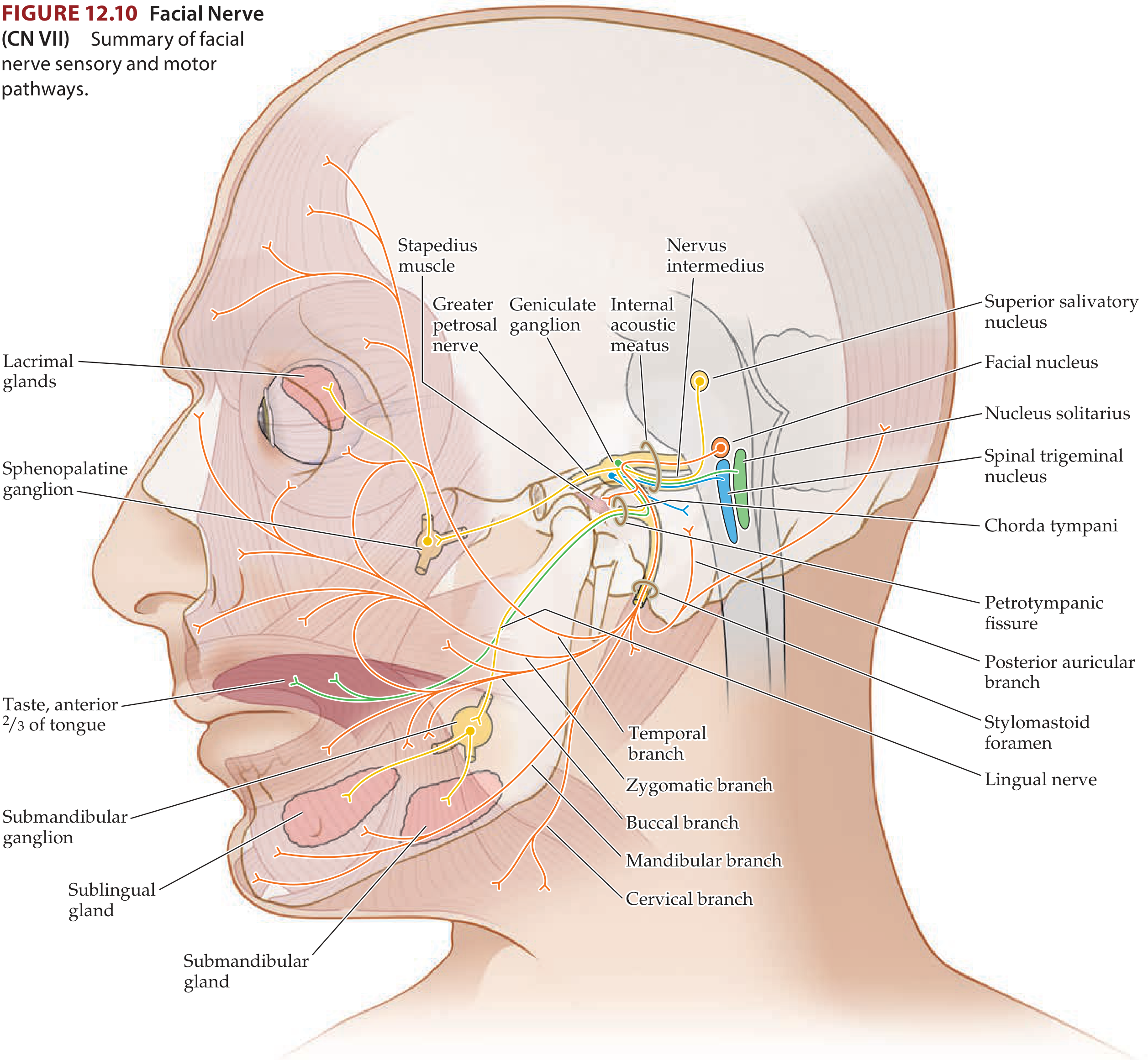
Fiber Components
The facial nerve carries four functional fiber types (Cummings Otolaryngology):
| Fiber Type | Function | Nucleus of Origin |
|---|---|---|
| Special visceral efferent (SVE) | Motor to muscles of facial expression, stapedius, stylohyoid, posterior digastric | Motor facial nucleus (caudal pons) |
| General visceral efferent (GVE) | Parasympathetic to lacrimal, nasal, submandibular, sublingual glands | Superior salivatory nucleus |
| Special visceral afferent (SVA) | Taste from anterior 2/3 of tongue, palate, tonsillar fossae | Cell bodies in geniculate ganglion → nucleus solitarius |
| General somatic afferent (GSA) | Sensation from EAC, conchal skin, mastoid; proprioception from facial muscles | Spinal trigeminal nucleus |
Nuclei (Central Connections)
- Facial motor nucleus — lateral tegmentum, caudal pons. The fascicles loop dorsally around the abducens nucleus, forming the facial colliculus on the floor of the fourth ventricle (a key landmark). Fibres then exit the brainstem ventrolaterally at the pontomedullary junction.
- Supranuclear innervation: Bilateral cortical input to the rostral (upper face) sub-nucleus; only contralateral input to the caudal (lower face) sub-nucleus. This explains why an upper motor neuron lesion spares the forehead.
- Superior salivatory nucleus — preganglionic parasympathetic fibres
- Nucleus tractus solitarius — taste afferents
- Spinal trigeminal nucleus — somatic afferents
Course & Segments
The nerve is classically divided into six segments (KJ Lee's Essential Otolaryngology):
1. Intracranial segment (17–24 mm)
Exits the pontomedullary junction at the cerebellopontine angle (CPA), lateral to CN VI, travelling with CN VIII and the nervus intermedius through the subarachnoid space to the internal auditory meatus (IAC). Blood supply: AICA.
2. Meatal (Canal) segment (8–10 mm)
Runs in the anterosuperior quadrant of the IAC to the meatal foramen. The motor division lies on the superoanterior surface of CN VIII. No branches arise here.
3. Labyrinthine segment (4 mm) ← narrowest & shortest
From the meatal foramen to the geniculate ganglion. Runs anterolaterally above the labyrinth. The nerve lacks endoneurium in the IAC but acquires a fibrous sheath at the geniculate ganglion. The meatal foramen is the narrowest point — most susceptible to inflammatory oedema (relevant in Bell's palsy).
Branch: Greater superficial petrosal nerve (GSPN) — arises from the geniculate ganglion apex; carries preganglionic parasympathetic fibres → pterygopalatine ganglion → lacrimal, palatal, and nasal glands. Also carries cutaneous afferents from EAC and mastoid.
4. Tympanic (Horizontal) segment (11 mm)
From the geniculate ganglion (first genu) to the second genu at the pyramidal eminence. Runs along the medial wall of the middle ear, superior to the oval window. No major branches. Bone over this segment is dehiscent in ~25% of ears.
5. Mastoid (Vertical) segment (13 mm)
From the second genu (just anteroinferior to the lateral semicircular canal) to the stylomastoid foramen. Lined distally by the aponeurosis of the posterior digastric — a surgical landmark for the stylomastoid foramen.
Branches:
- Nerve to stapedius — arises near the upper end
- Chorda tympani — arises just proximal to the stylomastoid foramen; ascends into the middle ear (passing between malleus and incus), exits via the petrotympanic fissure, joins the lingual nerve (V3) → submandibular ganglion → submandibular and sublingual glands (parasympathetic) + taste from anterior 2/3 tongue (afferent)
Blood supply of intrapetrosal segment: superficial branch of the middle meningeal artery and stylomastoid branch of the posterior auricular artery.
6. Extratemporal segment
Exits the stylomastoid foramen, immediately giving off:
- Posterior auricular nerve → occipitalis, posterior auricular, auricular muscles
- Digastric branch → posterior belly of digastric
- Stylohyoid branch → stylohyoid muscle
The nerve then enters the parotid gland, dividing at the pes anserinus into five terminal branches:
"To Zanzibar By Motor Car" (Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical)
These emerge from the borders of the parotid gland to innervate all muscles of facial expression.
Parasympathetic Pathways (Nervus Intermedius)
| Pathway | Preganglionic Origin | Ganglion | Target |
|---|---|---|---|
| GSPN → Vidian nerve | Superior salivatory / lacrimal nucleus | Pterygopalatine ganglion | Lacrimal gland, nasal/palatal glands |
| Chorda tympani → lingual nerve | Superior salivatory nucleus | Submandibular ganglion | Submandibular & sublingual glands |
Vascular Supply Summary
| Segment | Supply |
|---|---|
| Intracranial | AICA |
| Intrapetrosal | Middle meningeal artery (superficial br.) + stylomastoid br. of posterior auricular artery |
| Extracranial | Stylomastoid, posterior auricular, superficial temporal, transverse facial arteries |
Lesion Localisation
| Level of Lesion | Features |
|---|---|
| UMN (cortex/corticobulbar) | Contralateral lower face weakness; forehead spared (bilateral supranuclear supply) |
| Facial nucleus/fascicle (pons) | Ipsilateral whole face weakness + ipsilateral CN VI palsy (abducens involvement → facial colliculus) |
| Proximal to geniculate ganglion | All below + loss of lacrimation (GSPN affected) |
| Distal to geniculate, proximal to stapedius | All below + hyperacusis (stapedius nerve affected) |
| Distal to stapedius, proximal to chorda tympani | All below + loss of taste anterior 2/3 tongue, decreased salivation |
| Distal to chorda tympani / at stylomastoid foramen | Pure motor — ipsilateral facial palsy only |
Clinical Mnemonic
Bell's palsy (idiopathic) is the most common cause of acute lower motor neuron facial palsy. MRI shows linear enhancement from the distal IAC through the labyrinthine segment and geniculate ganglion. Imaging is reserved for atypical presentations (no recovery >6 months, recurrent ipsilateral palsy, facial twitching).
Causes of bilateral facial palsy: Lyme disease, Möbius syndrome, NF2, Guillain-Barré syndrome, bilateral temporal bone fractures, HIV.
Sources: Neuroanatomy through Clinical Cases 3rd Ed.; Cummings Otolaryngology Head and Neck Surgery; KJ Lee's Essential Otolaryngology; Gray's Anatomy for Students; Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology 8e
This is a shared conversation. Sign in to Orris to start your own chat.