I have all the material needed. Now I'll write the comprehensive 15-mark MD exam answer.
Granuloma and Granulomatous Infection of the Lung
DEFINITION AND ETYMOLOGY
The term granuloma (from the Latin granulum, a small grain) was coined by Rudolf Virchow (1818) originally to describe tumour-like lesions that ulcerate and form granulation tissue. In modern pathology, a granuloma is defined as a focal, compact collection of inflammatory cells in which mononuclear cells — principally activated macrophages (epithelioid histiocytes) — predominate, organised into a discrete structure with variable central necrosis, giant cells, and a peripheral lymphocytic cuff.
Granulomas are not merely passive collections of cells; they are active metabolic sites producing numerous enzymes and cytokines involved in trapping and removing the causative agent.
CLASSIFICATION OF GRANULOMAS
A. By Mechanism
| Type | Features | Examples |
|---|
| Immunological (Type IV hypersensitivity) | Prominent lymphocyte component; Th1-mediated | TB, sarcoidosis, berylliosis, hypersensitivity pneumonitis |
| Non-immunological (Foreign body) | No peripheral lymphocyte response | Silica, suture material, aspirated lipid |
B. By Necrosis
| Type | Features |
|---|
| Caseating (necrotising) | Central structureless "cheese-like" necrosis — classic of TB |
| Non-caseating (non-necrotising) | No necrosis — classic of sarcoidosis |
C. By Architecture
- Hard (proliferative) granuloma — well-circumscribed, compact epithelioid cells, lymphocyte cuff, few or no AFB
- Soft (exudative) granuloma — loose collection, neutrophils, macrophages, likely to harbour AFB
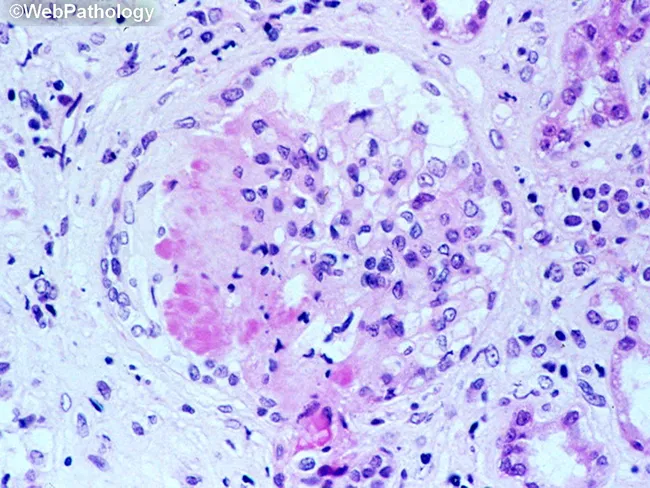
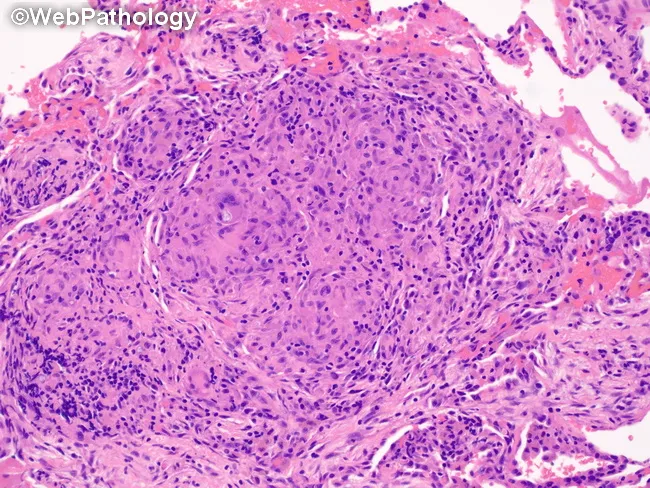
HISTOLOGICAL STRUCTURE OF A GRANULOMA
A well-formed epithelioid cell granuloma shows, from centre to periphery:
1. Central zone:
- Caseous necrosis (in TB) — structureless, acellular, eosinophilic material representing permanent tissue destruction
- Low O₂ tension and low pH within the caseum inhibit mycobacterial replication
2. Epithelioid histiocytes (activated macrophages):
- Activated macrophages with abundant pale eosinophilic cytoplasm
- Indistinct cell margins — form a continuous sheet resembling stratified squamous epithelium → hence "epithelioid"
- Express MHC class II molecules; function as antigen-presenting cells
3. Multinucleated giant cells:
Two types are seen in TB:
- Langhans giant cell: nuclei arranged along the periphery of the cell, forming a horseshoe/rosette — characteristic of TB
- Foreign body giant cell: nuclei irregularly scattered throughout the cytoplasm
Giant cells form by fusion of epithelioid macrophages, driven by cytokines (IFN-γ, TNF-α).
4. Peripheral lymphocytic cuff:
- Predominantly CD4+ T cells (Th1) in the centre; CD8+ T cells at periphery
- B cells may also be present
5. Fibroblastic rim:
- Surrounding fibrosis (more marked in hard granulomas)
- Reticulin fibres — preserved in sarcoidosis (useful distinguishing feature); lost or reduced in TB
PATHOGENESIS OF GRANULOMA FORMATION
The formation of a pulmonary granuloma follows a sequential Th1-driven immunological cascade:
-
Inhaled antigen (e.g., M. tuberculosis) is phagocytosed by alveolar macrophages via pattern recognition receptors (TLR2, TLR4, TLR9)
-
Macrophage-mycobacterium interaction: Mycobacteria prevent phagolysosome fusion, surviving intracellularly. Infected macrophages present antigen via MHC class II molecules to naïve CD4+ T cells in draining lymph nodes
-
Th1 polarisation: In the absence of IL-4, IL-12 released by macrophages drives differentiation of CD4+ T cells toward the Th1 phenotype. IFN-γ further amplifies IL-12 production — a positive feedback loop
-
Chemokine-mediated recruitment: Activated Th1 cells produce chemokines (MCP-1, MIP-1α, RANTES, IP-10) that recruit circulating monocytes and T cells to the lung parenchyma
-
Macrophage activation: IFN-γ and TNF-α activate recruited macrophages → production of reactive oxygen intermediates (H₂O₂) and reactive nitrogen intermediates (NO via iNOS2) → mycobactericidal activity
-
Granuloma assembly: Activated macrophages differentiate into epithelioid histiocytes; some fuse to form giant cells. CD4+ T cells predominate centrally; CD8+ cells at the periphery
-
Outcome: In immunocompetent hosts → containment, fibrocaseous healing, calcification. In immunocompromised → liquefaction, cavitation, dissemination
CAUSES OF GRANULOMATOUS LUNG DISEASE
Infectious
| Organism | Disease | Key Feature |
|---|
| Mycobacterium tuberculosis | Pulmonary TB | Caseating, confluent granulomas; AFB on ZN stain |
| M. leprae | Leprosy (lung rarely) | Leproma |
| Non-tuberculous mycobacteria (NTM) | e.g., MAC, M. kansasii | Loose granulomas; well-formed ones uncommon |
| Histoplasma capsulatum | Histoplasmosis | Necrotising granulomas; yeast in macrophages |
| Coccidioides immitis | Coccidioidomycosis | Granulomas with endospore-containing spherules |
| Blastomyces dermatitidis | Blastomycosis | Suppurative and granulomatous |
| Cryptococcus neoformans | Cryptococcosis | Gelatinous granulomas |
| Aspergillus spp. | Chronic pulmonary aspergillosis | Granulomatous reaction |
| Pneumocystis jirovecii | PCP (in AIDS) | Foamy alveolar exudate ± granuloma |
Non-infectious
| Cause | Disease |
|---|
| Unknown antigen | Sarcoidosis (non-caseating granulomas) |
| Beryllium dust | Chronic beryllium disease |
| Organic antigens | Hypersensitivity pneumonitis (extrinsic allergic alveolitis) |
| ANCA-associated vasculitis | Granulomatosis with polyangiitis (GPA, formerly Wegener's) |
| Eosinophilic granulomatosis | EGPA (Churg-Strauss) |
| Drug reactions | Methotrexate, TNF inhibitors |
| Aspirated material | Lipoid pneumonia |
PULMONARY TUBERCULOSIS — GRANULOMATOUS PATHOLOGY IN DETAIL
TB is the classical example of granulomatous inflammation. The pulmonary lesions are classified as:
A. Exudative (Soft) Granuloma
- Less well-demarcated
- Neutrophils, lymphocytes, macrophages, epithelioid cells in loose arrangement
- Little fibroblastic proliferation
- More likely to harbour AFB
- Seen more in primary disease, serous surfaces, immunosuppressed
B. Proliferative (Hard) Granuloma
- Well-circumscribed with a dense lymphocyte cuff
- Well-aggregated epithelioid histiocytes
- Prominent surrounding fibrosis
- Langhans giant cells more common
- AFB less readily demonstrated
C. Specific Pulmonary Lesions
Primary Complex (Ghon focus):
- Subpleural/lower lobe caseating granuloma at site of entry
- Draining lymph node granulomas + lymphangitis = Ghon complex
Post-primary (Adult) TB — Characteristic Lesions:
- Nodular lesions (Tuberculomas) — well-defined, <1 cm or >1 cm; central caseation surrounded by concentric fibrosis; rim calcification in healing
- Fibrocaseous disease — extensive caseation, fibrosis, multiple epithelioid palisades and Langhans cells; typically upper lobe/apical posterior segments
- Cavitary disease — liquefaction of caseous material + bronchial communication; cavity wall lined by TB granulation tissue; fibrosis; Rasmussen aneurysm from arterial wall erosion → fatal haemoptysis; AFB demonstrable in 88% of cavitary vs 77% non-cavitary lesions
- Miliary TB — haematogenous dissemination; symmetrical bilateral millet-seed nodules; two types:
- Hard (cellular) tubercles: compact epithelioid cells + Langhans cells, minimal caseation
- Soft tubercles: loose granulomas, prominent caseation, many AFB
- TB bronchopneumonia — acute dissemination via airways; neutrophilic reaction may mimic bacterial pneumonia; AFB stain essential
Healing and Fate of Granulomas:
- Fibrosis → cicatrisation (fibrocaseous → fibrous scar)
- Calcification (weeks to months)
- Ossification (years)
- Dormant bacilli may persist in calcified foci for decades
DIFFERENCES: TB vs SARCOIDOSIS GRANULOMAS
| Feature | Tuberculosis | Sarcoidosis |
|---|
| Necrosis | Usual (caseating) | Uncommon (non-caseating) |
| Granuloma pattern | Confluent | Discrete ("naked granulomas") |
| Giant cells | Multiple Langhans type | Few, foreign body type |
| Lymphocyte cuff | Prominent | Less prominent |
| Reticulin within granuloma | Usually lost | Usually preserved |
| Acid-fast bacilli | May be present | Absent |
| Fibrosis | Dense pericentric | Perigranuloma condensation |
| Vitamin D production | No | Yes (1,25-OH vitamin D by macrophages) → hypercalcaemia |
GRANULOMATOUS INFECTION: HISTOLOGICAL DIAGNOSIS
Staining Methods for AFB in Tissue
| Method | Notes |
|---|
| Modified Ziehl-Neelsen (ZN) | Standard; AFB = curved, beaded magenta/purplish-red rods; positivity 30–40% in histology, 60–70% in cytology smears |
| Auramine-Rhodamine | More sensitive; requires fluorescence microscope |
| Dieterle stain | Silver-based; more sensitive |
| Immunohistochemistry | Species identification possible |
| Nucleic acid amplification (PCR/GeneXpert) | Highest sensitivity; enables drug resistance detection |
| Culture | Gold standard for diagnosis and susceptibility testing |
Differential Diagnosis of Pulmonary Granulomas
When AFB is not identified, consider:
- Fungal infections (PAS, GMS stains for fungal organisms)
- Sarcoidosis (exclusion diagnosis; noncaseating, naked granulomas)
- Hypersensitivity pneumonitis (loose, ill-formed, bronchiolocentric granulomas + organizing pneumonia pattern)
- GPA (necrotising granulomatous vasculitis; C-ANCA/PR3-ANCA positive)
- Chronic beryllium disease (identical to sarcoidosis; beryllium lymphocyte proliferation test required)
- Foreign body granuloma (polarisable material on polarised light)
GRANULOMA IN IMMUNOCOMPROMISED HOSTS
In HIV/AIDS with severe immunosuppression (CD4 <200/mm³):
- Granulomas become poorly formed and eventually absent ("non-reactive TB")
- Epithelioid cells not well-developed; lymphocyte collar may be absent
- Giant cells rare; karyorrhexis present
- Multibacillary histiocytosis (macrophages stuffed with AFB, minimal inflammation) — characteristic of MAC in AIDS
- Middle and lower zone involvement rather than the classical apical disease
- Cavitation less frequent; sputum smear may be negative
- Antiretroviral therapy restores CMI → more typical granulomatous response returns
RADIOLOGICAL CORRELATION
| Pathological Stage | HRCT/CXR Finding |
|---|
| Early granulomas, no necrosis | Homogeneous hilar lymph node enhancement |
| Granulomas with central caseation | Peripheral rim-enhancement, central low attenuation on CECT |
| Fibrocaseous lesion | Upper lobe heterogeneous consolidation, volume loss |
| Cavitation | Thick-walled cavity, air-fluid level, bronchial communication |
| Miliary spread | 1–3 mm nodules bilaterally in random distribution |
| Healed/calcified | "Eggshell" or punctate calcification, Ghon calcification |
SUMMARY TABLE: CAUSES OF GRANULOMATOUS LUNG INFECTION
| Organism | Granuloma Type | Key Distinguishing Histology |
|---|
| M. tuberculosis | Caseating, confluent | Langhans cells, AFB on ZN |
| MAC/NTM | Loose, ill-formed | Spindle cell pseudotumours; multibacillary histiocytosis |
| Histoplasma | Necrotising | PAS+/GMS+ small yeasts (2–4 µm) within macrophages |
| Coccidioides | Granulomatous | Large spherules (20–60 µm) with endospores |
| Blastomyces | Suppurative + granulomatous | Broad-based budding yeast (8–15 µm), GMS+ |
| Cryptococcus | Gelatinous/granulomatous | Encapsulated yeast, mucicarmine+, India ink |
| Aspergillus | Necrotising | Septate hyphae, 45° branching, Grocott+ |
KEY POINTS FOR EXAM
- Definition: Focal compact collection of mononuclear inflammatory cells, predominantly activated macrophages (epithelioid histiocytes), ± necrosis, ± giant cells, ± lymphocytic cuff
- TB is the classical example of granulomatous inflammation — caseating, confluent granulomas
- Langhans giant cell (peripheral nuclear rosette) = TB; Foreign body giant cell (random nuclei) = foreign material
- Reticulin preserved in sarcoidosis; lost in TB — useful distinguishing histological feature
- Caseation implies active disease but mycobacteria can survive dormant in calcified foci
- Cavitation = liquefaction + bronchial communication; highest bacillary load; most infectious stage
- Th1 axis (IFN-γ, TNF-α, IL-12) is essential for granuloma integrity; defects → disseminated infection
- TNF-α blockade (biologics for RA) → reactivation TB via granuloma dissolution
- Non-reactive TB in AIDS: absent granulomas, sheets of AFB-laden macrophages
- Modified ZN stain remains the workhorse for AFB in tissue (30–40% positivity in histology)
Sources: Sharma SK & Mohan A, Textbook of Tuberculosis and Nontuberculous Mycobacterial Diseases (attached PDF, pp. 26–49); Murray & Nadel's Textbook of Respiratory Medicine, Ch. on Granulomatous Lung Disease (p. 366–367); Robbins & Kumar Basic Pathology — Sarcoidosis (p. 741–751), GPA (p. 333); Fishman's Pulmonary Diseases and Disorders — Sarcoidosis histopathology; Janeway's Immunobiology — granuloma immunopathogenesis