You are a Nursing Teacher and Exam Expert. Create simple, clear, deep, exam-ready notes for the topic I give. Rules: - Use very simple English and short sentences. - Explain the topic deeply so no important textbook concept is missed. - Use bullet points, flowcharts (→), tables, and simple labeled diagrams/pictures when useful. - Explain difficult words in brackets. Structure: 1. Introduction 2. Definition 3. Types / Classification 4. Causes / Etiology 5. Pathophysiology (flowchart) 6. Signs & Symptoms 7. Diagnosis / Investigations 8. Management - Medical - Nursing care (detailed) 9. Complications 10. Prevention 11. Quick revision points Add if needed: - Microbiology → structure, classification, culture, lab diagnosis - Pharmacology → classification, mechanism, uses, side effects, nursing responsibilities Also include: - 1–2 short clinical examples - Mnemonics if useful - 5 long questions, 5 short questions, 10 very short, 10 MCQs - Answer key - A final 1-page quick revision summary Wait for my topic. Unit IV: Explain the concepts of immunity, hyper sensitivity and immunization · Immunity · Immunity: Types, classification · Antigen and antibody reaction · Hypersensitivity reactions · Serological tests · Immunoglobulins: Structure, types & properties · Vaccines: Types & classification, storage and handling, cold chain, Immunization for various diseases · Immunization Schedule
immunoglobulin structure IgG antibody diagram
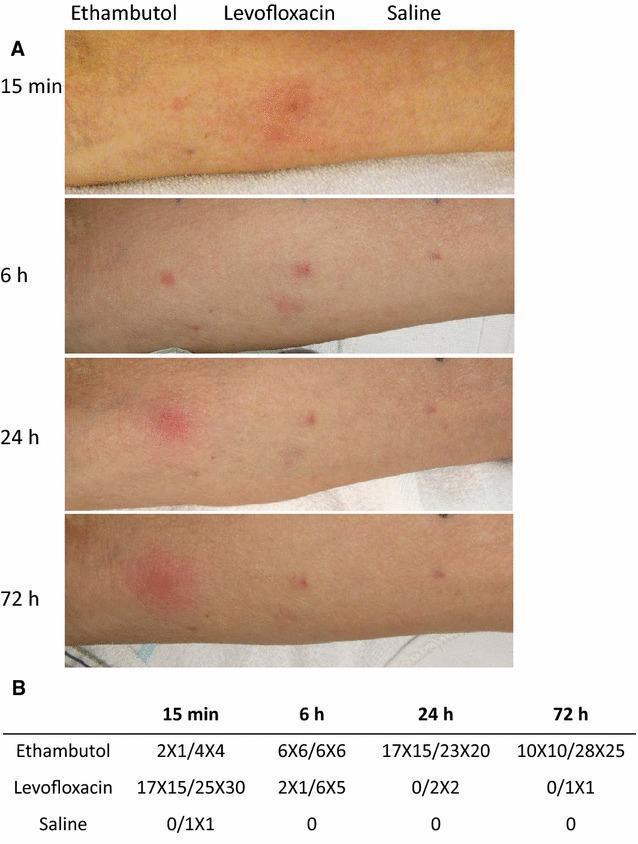
hypersensitivity types Gell Coombs classification reactions
📚 UNIT IV: IMMUNITY, HYPERSENSITIVITY & IMMUNIZATION
Complete Nursing Exam-Ready Notes
1. INTRODUCTION
- The human body is constantly exposed to harmful microorganisms (bacteria, viruses, fungi, parasites).
- The body has a defense system called the immune system to fight these threats.
- This unit covers how immunity works, what happens when it overreacts (hypersensitivity), and how we use vaccines to protect people.
2. DEFINITION
| Term | Definition |
|---|---|
| Immunity | The body's ability to resist infection and disease caused by foreign substances |
| Antigen | Any foreign substance that triggers an immune response (e.g., bacteria, virus, pollen) |
| Antibody | A protective protein made by B cells in response to an antigen |
| Immunization | The process of making a person immune to a disease, usually by a vaccine |
| Hypersensitivity | An exaggerated immune response that damages the body's own tissues |
3. TYPES / CLASSIFICATION OF IMMUNITY
A. Basic Classification
IMMUNITY
├── INNATE (Natural / Non-Specific)
│ ├── Present from birth
│ ├── No memory
│ └── First line of defense
└── ADAPTIVE (Acquired / Specific)
├── Develops after exposure
├── Has MEMORY
└── Specific to each antigen
B. Innate Immunity — Details
| Component | Function |
|---|---|
| Skin & mucus membranes | Physical barrier |
| Stomach acid (pH 2) | Kills pathogens |
| Fever | Slows pathogen growth |
| Inflammation | Brings WBCs to site of infection |
| NK cells (Natural Killer cells) | Kill virus-infected & cancer cells |
| Phagocytes (neutrophils, macrophages) | Engulf and destroy pathogens |
| Complement system | Proteins that lyse (burst) bacteria |
| Interferons | Antiviral proteins released by infected cells |
C. Adaptive Immunity — Details
ADAPTIVE IMMUNITY
├── HUMORAL (B-cell mediated)
│ ├── B lymphocytes → plasma cells → ANTIBODIES
│ ├── Fights extracellular pathogens (bacteria, viruses in blood)
│ └── Example: antibodies against Tetanus toxin
└── CELL-MEDIATED (T-cell mediated)
├── T lymphocytes (T-helper, T-cytotoxic)
├── Fights intracellular pathogens (viruses, TB, fungi)
└── Example: killing of virus-infected cells by CD8+ T cells
D. Classification by How Immunity Is Acquired
ACQUIRED IMMUNITY
├── ACTIVE (host makes own antibodies)
│ ├── Natural Active → infection/disease (e.g., chicken pox)
│ └── Artificial Active → VACCINES (e.g., MMR vaccine)
└── PASSIVE (ready-made antibodies given)
├── Natural Passive → maternal antibodies via placenta/breast milk
└── Artificial Passive → antiserum/immunoglobulins (e.g., anti-rabies serum)
Mnemonic: NAPA — Natural Active, Passive Active → think "NAPA" for the four types
| Feature | Active | Passive |
|---|---|---|
| Antibody source | Host makes own | Transferred from outside |
| Onset | Slow (days-weeks) | Immediate |
| Duration | Long-lasting (years/life) | Short (weeks-months) |
| Memory | YES | NO |
| Example | Vaccine, natural infection | Anti-tetanus serum, breast milk |
4. ANTIGEN AND ANTIBODY REACTION
What is an Antigen?
- A substance (usually protein or polysaccharide) that the immune system recognizes as foreign
- Has special sites called epitopes (antigenic determinants) — these are the parts the antibody binds to
- Types:
- T-dependent antigen → needs T-helper cells to stimulate antibody production (most proteins)
- T-independent antigen → stimulates B cells directly (polysaccharides)
What is an Antibody (Immunoglobulin)?
- A Y-shaped glycoprotein made by plasma cells (activated B cells)
- Specifically binds to the antigen that triggered its production
Antigen-Antibody Reaction (Immunological Reaction)
Antigen enters body
↓
Recognized by B cells (with help from T-helper cells)
↓
B cells → Plasma cells → Antibodies produced
↓
Antibody binds to specific antigen (lock-and-key)
↓
Results in:
├── Neutralization (toxin/virus rendered harmless)
├── Opsonization (antigen coated for phagocytosis)
├── Complement activation (bacterial lysis)
├── Agglutination (clumping of antigens)
└── Precipitation (soluble antigen made insoluble)
5. IMMUNOGLOBULINS: STRUCTURE, TYPES & PROPERTIES
Structure of an Antibody (IgG as model)
Fab (Antigen-binding) Fab
┌────────┐ ┌────────┐
│ VH+VL │ │ VH+VL │ ← Variable regions (bind antigen)
└────┬───┘ └────┬───┘
│ │
─────┴────────────────┴─────
│ HINGE REGION │ ← Flexible
│ CH2 │
│ CH3 │ ← Fc region (complement, receptor binding)
└──────────────────────────┘
- 2 Heavy chains (H) + 2 Light chains (L) linked by disulfide bonds
- Each chain has a Variable region (V) — binds antigen (unique per antibody)
- Each chain has a Constant region (C) — determines Ig class and effector function
- Fab fragment = antigen-binding fragment (contains variable regions)
- Fc fragment = crystallizable fragment (binds complement, macrophage receptors)
- Paratope = part of antibody that binds to epitope
Five Classes of Immunoglobulins
| Class | % in serum | Structure | Key Properties |
|---|---|---|---|
| IgG | 75–80% | Monomer | Most abundant; crosses placenta (passive immunity to newborn); 4 subclasses (IgG1–4); secondary immune response; opsonization |
| IgA | 10–15% | Dimer (secretory) | Found in secretions: saliva, tears, breast milk, intestinal mucus; first defense at mucosal surfaces |
| IgM | 5–10% | Pentamer | Largest Ig; first to appear in primary immune response; best at agglutination & complement activation; ABO blood group antibodies |
| IgE | Trace (<0.01%) | Monomer | Allergic reactions (binds mast cells, basophils); anti-parasitic immunity; involved in Type I hypersensitivity |
| IgD | <1% | Monomer | B-cell surface receptor; function not fully known |
Mnemonic: GAMED — IgG, IgA, IgM, IgE, IgD (in order of serum concentration)
Properties Summary Table
| Property | IgG | IgA | IgM | IgE | IgD |
|---|---|---|---|---|---|
| Crosses placenta | ✅ | ❌ | ❌ | ❌ | ❌ |
| In secretions | ❌ | ✅ | ❌ | ❌ | ❌ |
| Complement fixation | ✅ | ❌ | ✅✅ | ❌ | ❌ |
| Allergy/anaphylaxis | ❌ | ❌ | ❌ | ✅ | ❌ |
| Primary response | ❌ | ❌ | ✅ | ❌ | ❌ |
6. HYPERSENSITIVITY REACTIONS
Definition
- An exaggerated or inappropriate immune response to an antigen (allergen) that causes tissue damage
- Classified by Gell and Coombs (1963) into 4 types
Gell & Coombs Classification
HYPERSENSITIVITY
├── Type I → Immediate / Anaphylactic (IgE-mediated)
├── Type II → Cytotoxic (IgG/IgM-mediated, cell destruction)
├── Type III → Immune Complex (IgG-mediated, complex deposition)
└── Type IV → Delayed / Cell-mediated (T-cell mediated, NO antibody)
Mnemonic: ACID — Anaphylactic, Cytotoxic, Immune-complex, Delayed
TYPE I — Immediate Hypersensitivity (Anaphylactic)
Time of onset: Within minutes (15–30 min)
Cells involved: Mast cells, basophils, eosinophils
First exposure to allergen (e.g., peanut, penicillin, pollen)
↓
B cells stimulated → IgE antibodies produced
↓
IgE binds to surface of MAST CELLS and BASOPHILS (sensitization)
↓
Second exposure to same allergen
↓
Allergen cross-links IgE on mast cells
↓
DEGRANULATION → release of:
├── Histamine → vasodilation, bronchoconstriction, itching
├── Leukotrienes → prolonged bronchoconstriction
├── Prostaglandins → inflammation
└── Tryptase (marker of anaphylaxis)
↓
Clinical effects: urticaria, angioedema, bronchospasm, anaphylaxis
- Anaphylaxis (penicillin, bee sting)
- Bronchial asthma
- Allergic rhinitis (hay fever)
- Urticaria (hives)
- Food allergy (peanuts, shellfish)
A 22-year-old nursing student receives IV penicillin and within 10 minutes develops rash, swelling of throat, low BP, and difficulty breathing → Anaphylactic shock = Type I hypersensitivity. Treatment: Adrenaline (epinephrine) 0.5 mg IM immediately.
TYPE II — Cytotoxic Hypersensitivity
Time of onset: Minutes to hours
Target: Cell surface antigens (host cells destroyed)
Antibody (IgG/IgM) binds to antigen on HOST CELL SURFACE
↓
Complement activated → cell LYSIS (MAC attack)
OR
Phagocytosis of opsonized cells
OR
ADCC (Antibody Dependent Cell-mediated Cytotoxicity)
↓
HOST CELLS DESTROYED
- ABO transfusion reactions (wrong blood group given)
- Hemolytic disease of newborn (Rh incompatibility — Rh−ve mother, Rh+ve baby)
- Autoimmune hemolytic anemia
- Goodpasture syndrome (antibodies to glomerular basement membrane)
- Myasthenia gravis (antibodies against acetylcholine receptors)
- Graves' disease (antibodies stimulate TSH receptors → hyperthyroidism)
TYPE III — Immune Complex Hypersensitivity
Time of onset: Hours (3–10 hours)
Target: Blood vessels, kidneys, joints (where complexes deposit)
Antigen (soluble) + Antibody → IMMUNE COMPLEX formed
↓
Immune complexes DEPOSIT in vessel walls, glomeruli, joints
↓
Complement activated
↓
Neutrophils attracted → release lysosomal enzymes
↓
TISSUE INFLAMMATION and DAMAGE
- Serum sickness (after horse antiserum — old anti-tetanus)
- Post-streptococcal glomerulonephritis
- Systemic Lupus Erythematosus (SLE)
- Rheumatoid arthritis
- Arthus reaction (local immune complex reaction — repeat injection)
- Farmer's lung (inhaled mold antigens)
TYPE IV — Delayed-Type Hypersensitivity (Cell-Mediated)
Time of onset: 48–72 hours (delayed)
Cells: CD4+ T-helper cells (Th1), CD8+ cytotoxic T cells, macrophages
First exposure to antigen → T cells sensitized (memory T cells formed)
↓
Second exposure (24–72 hrs later)
↓
Memory T cells recognize antigen via APC (dendritic cells/macrophages)
↓
T cells activated → release CYTOKINES (IFN-γ, TNF, IL-2)
↓
Macrophages activated → release inflammatory mediators
↓
TISSUE DESTRUCTION (granuloma formation)
- Tuberculin (Mantoux) test ← most important exam example
- Contact dermatitis (nickel, latex, poison ivy)
- Graft rejection (transplant rejection)
- Granulomatous diseases (TB, leprosy, sarcoidosis)
A nurse reads a Mantoux test 72 hours after injection. She finds induration [hardness] of 15 mm → Positive → suggests TB infection = Type IV hypersensitivity
Comparison Table of All 4 Types
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Mediator | IgE | IgG/IgM | IgG/IgM complexes | T cells |
| Onset | Min (< 30 min) | Min–hours | 3–10 hrs | 48–72 hrs |
| Complement | ❌ | ✅ | ✅ | ❌ |
| Cells | Mast cells, basophils | Complement, phagocytes | Neutrophils | T cells, macrophages |
| Key example | Anaphylaxis | ABO mismatch | SLE, serum sickness | Mantoux, contact dermatitis |
| Transferred by | Serum (IgE) | Serum | Serum | Cells only |
7. SEROLOGICAL TESTS (Antigen-Antibody Tests)
Serology [sero = serum] = laboratory tests that detect antibodies or antigens in blood serum
Classification of Serological Tests
A. Precipitation Tests
- Antigen + Antibody → insoluble precipitate forms
- Examples:
- Immunodiffusion (Ouchterlony test) — antigens/antibodies diffuse in gel; precipitation line forms where they meet
- VDRL test (Venereal Disease Research Laboratory) — for syphilis screening; flocculation [clumping] reaction
- RPR test (Rapid Plasma Reagin) — syphilis
- C-reactive protein (CRP) test — detects inflammation
B. Agglutination Tests
- Antigen (cell surface) + Antibody → visible clumping
- Examples:
- Widal test — for typhoid fever (detects antibodies against Salmonella typhi)
- ABO blood grouping — agglutination of RBCs
- Coombs test (DCT/ICT) — hemolytic disease of newborn, autoimmune hemolytic anemia
- ASO test (Anti-Streptolysin O) — detects recent streptococcal infection
- RA Factor (Rheumatoid Factor) test — for rheumatoid arthritis
C. Complement Fixation Tests
- If antigen + antibody present → complement is "used up" (fixed) → indicator system remains intact (no lysis)
- Examples:
- Wassermann test — syphilis (historical)
- CFT for viral antibodies — measles, mumps
D. Neutralization Tests
- Antibody neutralizes the biological activity of a toxin or virus
- Examples:
- ASO titre — neutralization of streptolysin O
- Virus neutralization tests — check immunity to specific viruses
E. Immunofluorescence Tests
- Antibodies labeled with fluorescent dye → seen under fluorescence microscope
- Examples:
- IFAT (Indirect Fluorescent Antibody Test)
- ANA test (Anti-Nuclear Antibody) — for SLE
- TPHA test — for syphilis confirmation
F. Enzyme-Linked Tests (ELISA)
- ELISA (Enzyme-Linked ImmunoSorbent Assay)
- Most common and important modern test
- Detects antibodies (IgG, IgM) or antigens
- Used for:
- HIV screening (ELISA for anti-HIV antibodies)
- Hepatitis B & C
- TORCH infections in pregnancy
- COVID-19 antibody tests
G. Radioimmunoassay (RIA)
- Uses radioactively labeled antigen or antibody
- Very sensitive but requires radioactive material
- Used for: hormone levels (insulin, TSH), HBsAg (Hepatitis B surface antigen)
H. Western Blot
- Confirmatory test for HIV (after ELISA screening)
- Separates viral proteins by electrophoresis → detected by antibodies
- Gold standard for HIV confirmation
Important Serological Tests Summary Table
| Test | Disease | Principle |
|---|---|---|
| Widal test | Typhoid | Agglutination |
| VDRL / RPR | Syphilis | Precipitation/Flocculation |
| ASO titre | Streptococcal infection | Neutralization/Agglutination |
| Coombs test (DCT/ICT) | Hemolytic anemia, Rh incompatibility | Agglutination |
| ELISA | HIV, Hepatitis, COVID-19 | Enzyme-linked |
| Western Blot | HIV confirmation | Immunoelectrophoresis |
| ANA test | SLE | Immunofluorescence |
| Mantoux/Tuberculin | TB | Delayed hypersensitivity (Type IV) |
| RA Factor | Rheumatoid arthritis | Agglutination |
8. VACCINES: TYPES, CLASSIFICATION, STORAGE & COLD CHAIN
Definition
- A vaccine is a biological preparation that provides active acquired immunity to a specific disease
- It contains antigens (weakened/killed/toxoid/subunit) that stimulate an immune response without causing disease
Types / Classification of Vaccines
1. Live Attenuated [weakened] Vaccines
- Contain weakened but living microorganisms
- Give strong, long-lasting immunity (similar to natural infection)
- Usually 1–2 doses sufficient
- Contraindicated in immunocompromised patients (HIV, on steroids)
| Vaccine | Disease |
|---|---|
| BCG | Tuberculosis |
| OPV (Oral Polio Vaccine) | Poliomyelitis |
| MMR | Measles, Mumps, Rubella |
| Varicella vaccine | Chickenpox |
| Yellow Fever vaccine | Yellow fever |
| Rotavirus vaccine | Rotavirus diarrhea |
| Typhoid oral (Ty21a) | Typhoid |
2. Killed (Inactivated) Vaccines
- Contain dead microorganisms — cannot cause disease
- Safer, more stable
- Require multiple doses + boosters (weaker immunity)
- Safe in immunocompromised patients
| Vaccine | Disease |
|---|---|
| IPV (Inactivated Polio Vaccine) | Poliomyelitis |
| Pertussis (whole cell) in DPT | Whooping cough |
| Rabies vaccine (HDCV) | Rabies |
| Influenza (injectable) | Influenza |
| Cholera vaccine | Cholera |
| Hepatitis A vaccine | Hepatitis A |
3. Toxoid Vaccines
- Made from inactivated bacterial toxins (the poison, not the bacteria)
- Stimulate antibodies against toxin only
- Very stable
| Vaccine | Disease |
|---|---|
| DT / dT / Td | Diphtheria, Tetanus |
| TT (Tetanus Toxoid) | Tetanus |
4. Subunit / Recombinant Vaccines
- Contain only specific parts (proteins) of the pathogen
- Very safe, no risk of infection
- Hepatitis B vaccine (HBsAg protein) — recombinant DNA technology
- Pertussis acellular (DTaP) — pertussis proteins only
- HPV vaccine (Gardasil, Cervarix) — virus-like particles
- Pneumococcal vaccine (PCV)
- Meningococcal vaccine
5. Conjugate Vaccines
- Polysaccharide antigen conjugated (joined) to a protein carrier
- Makes polysaccharide antigens work in infants (T-cell dependent response)
- Examples:
- Hib vaccine (Haemophilus influenzae type b)
- PCV (Pneumococcal Conjugate Vaccine)
- MenACWY (Meningococcal conjugate vaccine)
6. mRNA Vaccines (Newer type)
- Deliver instructions (mRNA) for cells to make viral protein → immune response
- Example: COVID-19 vaccines (Pfizer-BioNTech, Moderna)
- No DNA alteration; mRNA quickly degraded
7. Combination Vaccines
- Multiple vaccines in one injection
- Reduces number of injections, increases compliance
| Vaccine | Diseases covered |
|---|---|
| DPT (Diphtheria-Pertussis-Tetanus) | Diphtheria, Whooping cough, Tetanus |
| MMR | Measles, Mumps, Rubella |
| MMRV | Measles, Mumps, Rubella, Varicella |
| Pentavalent vaccine | Diphtheria, Tetanus, Pertussis, Hepatitis B, Hib |
| Hexavalent vaccine | + Polio |
Vaccine Storage and Handling
Principles
- Vaccines are biological products — destroyed by heat, freezing (some), and light
- Must be stored at correct temperature throughout supply chain
Storage Temperatures
| Vaccine Category | Storage Temp |
|---|---|
| Freeze-sensitive (must NOT freeze) | +2°C to +8°C (refrigerator) |
| Freeze-tolerant (can freeze) | −15°C to −25°C (freezer) |
| Vaccine | Storage | Sensitivity |
|---|---|---|
| BCG | Freezer (−15°C to −25°C) | Sensitive to heat & light |
| OPV | Freezer (−20°C) | Very heat-sensitive; can store frozen |
| IPV | Refrigerator (+2 to +8°C) | Freeze-sensitive |
| DPT | Refrigerator (+2 to +8°C) | FREEZE-SENSITIVE — freezing destroys it |
| Hepatitis B | Refrigerator (+2 to +8°C) | FREEZE-SENSITIVE |
| TT | Refrigerator (+2 to +8°C) | FREEZE-SENSITIVE |
| MMR | Freezer or refrigerator | Sensitive to heat & light |
| Measles | Refrigerator, protect from light | Heat & light-sensitive |
| Pentavalent | Refrigerator (+2 to +8°C) | FREEZE-SENSITIVE |
⚠️ Key exam point: Vaccines most sensitive to freezing: DPT, TT, Hepatitis B, IPV, Pentavalent
⚠️ Vaccines most sensitive to heat: OPV, BCG, Measles, MMR
Reconstituted Vaccines (mixed before use)
- BCG, Measles, MMR must be used within 4–6 hours after reconstitution [mixing with diluent]
- Discard unused reconstituted vaccine at end of session
Cold Chain
Definition
- Cold chain = the system of transporting and storing vaccines at the correct temperature from manufacturer to patient
Importance
- Maintains potency (effectiveness) of vaccines
- Prevents vaccine wastage
- Ensures immunization programs succeed
Cold Chain Equipment
VACCINE MANUFACTURER (−25°C to −15°C or +2 to +8°C)
↓
PRIMARY VACCINE STORE (National level) — Deep freezers + ILR
↓
REGIONAL / STATE VACCINE STORE — Deep freezers + ILR
↓
DISTRICT VACCINE STORE — ILR (Ice-Lined Refrigerator) + Deep freezers
↓
PHC (Primary Health Center) — ILR + Deep freezers
↓
SUBCENTRE / SESSION SITE — Vaccine carrier + cold packs
↓
PATIENT / COMMUNITY
- ILR = Ice-Lined Refrigerator (insulated box, runs on electricity, stores +2 to +8°C)
- Deep Freezer = stores at −15°C to −25°C (for OPV, BCG)
- Vaccine carrier = insulated box with frozen ice packs — for transport to field
- Cold box = large insulated box for transport between stores
- Cold packs / Ice packs = keep vaccines cold in carrier
Cold Chain Monitoring Tools
| Tool | Purpose |
|---|---|
| VVM (Vaccine Vial Monitor) | Sticker on vaccine vial — changes color if vaccine exposed to excess heat; tells if vaccine is unusable |
| Thermometer | Measures fridge/freezer temperature |
| Freeze indicator (FI) | Detects if freeze-sensitive vaccine was frozen |
| Electronic data logger | Continuous temperature recording |
| Open Vial Policy | Allows reuse of unopened multi-dose vials at next session (except BCG, measles, yellow fever, VZV) |
VVM Reading (Exam Important)
VVM (inner square inside outer circle)
├── Inner square LIGHTER than outer circle → USABLE ✅
└── Inner square SAME or DARKER than outer circle → DISCARD ❌
Nursing Responsibilities in Cold Chain
- Check temperature daily (2 times/day: morning and evening) — record in temperature log
- Never store food, blood, or other items in vaccine fridge
- Never keep vaccines in door of refrigerator (temperature fluctuates)
- Place ice packs at bottom of vaccine carrier before use
- Check VVM before giving each vaccine
- Report cold chain equipment failures immediately
- Store vaccines according to FIFO (First In, First Out) principle
- Keep extra ice packs in freezer always
9. IMMUNIZATION FOR VARIOUS DISEASES — NATIONAL IMMUNIZATION SCHEDULE (India)
Universal Immunization Programme (UIP)
- Started in India in 1985 (expanded from EPI started 1978)
- Mission Indradhanush launched 2014 — aimed to increase coverage to 90%+ children
- Target: Pregnant women + children 0–5 years
Immunization Schedule (India — Current UIP)
| Age | Vaccine | Route | Dose | Site |
|---|---|---|---|---|
| Birth (0–24 hrs) | OPV-0 (birth dose) | Oral | 2 drops | Mouth |
| BCG | Intradermal | 0.05 ml (<1 yr), 0.1 ml (>1 yr) | Left upper arm | |
| Hepatitis B (birth dose) | IM | 0.5 ml | Anterolateral thigh (right) | |
| 6 weeks (1.5 months) | OPV-1 | Oral | 2 drops | Mouth |
| Pentavalent-1 (DPT+HepB+Hib) | IM | 0.5 ml | Anterolateral thigh (left) | |
| Rotavirus-1 | Oral | 5 drops | Mouth | |
| PCV-1 (Pneumococcal) | IM | 0.5 ml | Anterolateral thigh (right) | |
| fIPV-1 (Fractional IPV) | Intradermal | 0.1 ml | Right anterolateral thigh | |
| 10 weeks (2.5 months) | OPV-2 | Oral | 2 drops | |
| Pentavalent-2 | IM | 0.5 ml | ||
| Rotavirus-2 | Oral | 5 drops | ||
| 14 weeks (3.5 months) | OPV-3 | Oral | 2 drops | |
| Pentavalent-3 | IM | 0.5 ml | ||
| Rotavirus-3 | Oral | 5 drops | ||
| PCV-2 | IM | 0.5 ml | ||
| fIPV-2 | Intradermal | 0.1 ml | ||
| 9–12 months | Measles-Rubella (MR)-1 | Subcutaneous | 0.5 ml | Right upper arm |
| PCV Booster | IM | 0.5 ml | ||
| Vitamin A (1st dose) | Oral | 1 lakh IU | ||
| 16–24 months | DPT Booster-1 | IM | 0.5 ml | Anterolateral thigh |
| OPV Booster | Oral | 2 drops | ||
| MR-2 | Subcutaneous | 0.5 ml | Right upper arm | |
| Vitamin A (every 6 months till 5 yrs) | Oral | 2 lakh IU | ||
| 5–6 years | DPT Booster-2 | IM | 0.5 ml | Upper arm |
| 10 years & 16 years | Td (Tetanus + adult diphtheria) | IM | 0.5 ml | Upper arm |
Vaccines for Pregnant Women
| Vaccine | Schedule | Purpose |
|---|---|---|
| TT/Td-1 | As early as possible in pregnancy | Sensitization dose |
| TT/Td-2 | 4 weeks after TT-1 | Boosts immunity |
| TT Booster | If received TT in last 3 years | Single booster dose |
Protection conferred: Prevents neonatal tetanus (tetanus in newborn) and maternal tetanus
Other Important Vaccines (Optional/Special Situations)
| Vaccine | For Whom | Schedule |
|---|---|---|
| Typhoid vaccine | Age 2 yrs+; endemic areas, travellers | Oral (Ty21a): 3 doses; IM (Vi): 1 dose; booster every 3 years |
| Hepatitis A vaccine | Age 1 yr+; not in UIP | 2 doses: 0 and 6–12 months |
| Varicella (Chickenpox) | 12 months+; 2 doses | 0 and 3 months |
| HPV vaccine | Girls 9–14 yrs (cervical cancer prevention) | 2 doses: 0 and 6 months |
| Meningococcal | High-risk, Hajj pilgrims | Single dose |
| Yellow Fever | Travellers to endemic areas (Africa, S. America) | 1 dose; life-long protection |
| Rabies (post-exposure) | After animal bite | Days 0, 3, 7, 14, 28 (IM) |
| Japanese Encephalitis (JE) | Endemic districts in India | 2 doses at 9 months and 16–24 months |
| Influenza | Healthcare workers, elderly, high-risk | Annual dose |
| Pneumococcal (PPSV23) | Adults >65 yrs, immunocompromised | 1–2 doses |
10. NURSING CARE IN IMMUNIZATION
Pre-vaccination Nursing Responsibilities
- Take detailed history: previous vaccinations, allergies, current illness
- Contraindications to check:
- Acute febrile illness → postpone vaccine
- Anaphylaxis to previous dose → contraindicated
- Live vaccines in immunocompromised patients
- Encephalopathy within 7 days of DPT → no more DPT
- Inform parents about the vaccine, disease it prevents, and possible side effects (consent)
- Check VVM on each vaccine vial
- Check expiry date
- Prepare correct dose and reconstitute if needed
- Check cold chain maintenance
During Vaccination
- Use correct route (IM, SC, intradermal, oral)
- Use correct site as per age
- Use proper injection technique (no air bubbles for injections)
- Observe strict aseptic technique
- Dispose of needles safely (no recapping — sharps container)
- Reconstituted vaccine: shake well before use
Post-vaccination Nursing Responsibilities
- Observe patient for 30 minutes for anaphylaxis (especially after first dose)
- Anaphylaxis kit ready: adrenaline, antihistamine, corticosteroids, IV fluids
- Document: vaccine name, dose, batch number, expiry, site, date
- Inform parents about normal post-vaccination reactions
- Advice for common side effects:
- Fever → paracetamol, tepid sponging
- Local swelling/redness → cold compress, reassurance
- BCG ulcer/scar → normal, no treatment needed
- OPV: sore mouth → very rare; reassure
AEFI (Adverse Events Following Immunization)
-
Any untoward medical event that follows immunization
-
Types:
- Vaccine-related (e.g., VAPP — vaccine-associated paralytic polio from OPV)
- Injection-related (abscess, nerve damage)
- Immunization error (wrong dose, wrong route)
- Coincidental (not caused by vaccine)
-
Must be reported to health authorities within 24 hours for serious AEFI
11. SIGNS & SYMPTOMS — ANAPHYLAXIS (most important acute immune emergency)
Anaphylaxis = severe, life-threatening Type I hypersensitivity reaction
Mnemonic: "ABCDEF" for Anaphylaxis features
- Airway obstruction (throat swelling, stridor)
- Breathing difficulty (bronchospasm, wheeze)
- Cardiovascular collapse (hypotension, tachycardia)
- Dermal signs (urticaria, angioedema, flushing, itching)
- Excretion (nausea, vomiting, diarrhea)
- Feeling of doom (anxiety, confusion, loss of consciousness)
Anaphylaxis Management (Nursing Emergency)
RECOGNIZE: Symptoms within minutes of exposure
↓
CALL FOR HELP / CODE BLUE
↓
LAY PATIENT FLAT — raise legs (unless breathing difficulty → semi-recumbent)
↓
ADRENALINE (EPINEPHRINE): 0.5 mg IM (1:1000) in outer thigh — FIRST DRUG
↓
O₂ therapy (high flow, 10–15 L/min via mask)
↓
IV access — normal saline bolus (500 ml–1 L)
↓
ANTIHISTAMINE: Chlorphenamine 10 mg IV/IM
↓
HYDROCORTISONE: 200 mg IV (prevents biphasic reaction)
↓
MONITOR: BP, pulse, SpO₂ every 5 min
↓
OBSERVE minimum 6 hours (risk of biphasic reaction — second wave)
12. DIAGNOSIS / INVESTIGATIONS FOR IMMUNE DISORDERS
| Investigation | Purpose |
|---|---|
| CBC with differential | WBC count; lymphocytopenia → immunodeficiency |
| Serum immunoglobulins (IgG, IgA, IgM, IgE) | Low IgG → hypogammaglobulinemia; high IgE → allergy |
| Skin prick test / intradermal test | Detects Type I hypersensitivity (allergy testing) |
| Patch test | Detects Type IV (contact dermatitis) |
| Mantoux test | Detects TB (Type IV hypersensitivity) |
| ELISA | HIV, Hepatitis, autoantibodies |
| ANA (Anti-Nuclear Antibody) | SLE |
| Complement levels (C3, C4) | Low in SLE, immune complex diseases |
| Flow cytometry | CD4/CD8 count (HIV staging) |
| Western Blot | HIV confirmation |
| Coombs test | Hemolytic anemia |
13. COMPLICATIONS
Complications of Immune Disorders
| Condition | Complication |
|---|---|
| Anaphylaxis | Death from cardiovascular/respiratory collapse |
| Hypersensitivity reactions | Organ damage, chronic inflammation |
| SLE | Lupus nephritis, pericarditis, neuropsychiatric lupus |
| Rheumatoid arthritis | Joint deformity, disability |
Complications of Vaccines
| Vaccine | Complication |
|---|---|
| OPV | VAPP (Vaccine-Associated Paralytic Polio) — rare, 1/750,000 |
| BCG | BCG-itis (disseminated BCG in immunocompromised) |
| DPT | Febrile seizures, encephalopathy (rare) |
| MMR | Febrile seizures, thrombocytopenia (rare) |
Complications of Cold Chain Failure
- Vaccine rendered ineffective (loss of potency)
- Vaccine-preventable disease outbreaks
- False sense of security in immunized population
14. PREVENTION
- Maintain cold chain rigorously
- Educate communities about immunization benefits
- Ensure complete immunization schedule is followed (full doses, correct timing)
- Monitor for AEFI and report
- Conduct immunization camps in remote areas (Mission Indradhanush)
- Administer vaccines by trained healthcare personnel only
- Maintain herd immunity [when enough population is immune, disease cannot spread]
15. QUICK REVISION POINTS ⚡
- Innate = non-specific, fast, no memory | Adaptive = specific, slower, has memory
- Active immunity = makes own antibodies (long lasting) | Passive = ready-made antibodies (short lasting)
- IgG = most abundant, crosses placenta | IgA = secretions/mucosa | IgM = first in primary response | IgE = allergy/anaphylaxis
- Type I = IgE, mast cells, immediate → anaphylaxis, asthma, urticaria
- Type II = IgG/IgM, cell destruction → ABO mismatch, hemolytic disease of newborn
- Type III = immune complexes → SLE, serum sickness, post-strep GN
- Type IV = T cells, 48–72 hrs → Mantoux test, contact dermatitis, graft rejection
- VDRL = syphilis | Widal = typhoid | ELISA = HIV, Hep B | Western Blot = HIV confirmation
- VVM inner square lighter than outer = vaccine usable ✅ | Same/darker = discard ❌
- DPT, TT, HepB = freeze-sensitive | OPV, BCG = heat-sensitive
- First drug in anaphylaxis = ADRENALINE (Epinephrine) 0.5 mg IM
- BCG given at birth (0–24 hrs) | OPV birth dose also at birth
- Pentavalent = 5 antigens in 1 vaccine: DPT + HepB + Hib
- Observe 30 minutes post-vaccination for anaphylaxis
16. MICROBIOLOGY — RELEVANT POINTS
Immunological Aspects of Microbiology
Viral vaccines: Live attenuated (OPV, MMR, BCG) or killed (IPV, rabies)
- Typhoid: Widal test (H & O agglutinins ≥ 1:160 = significant)
- Syphilis: VDRL (screening) → TPHA or FTA-ABS (confirmation)
- HIV: ELISA (screening) → Western blot (confirmation)
- Hepatitis B: HBsAg (surface antigen) = active infection; Anti-HBs = immunity
17. PHARMACOLOGY — RELEVANT DRUGS
Drugs Used in Anaphylaxis
| Drug | Class | Mechanism | Dose | Nursing Points |
|---|---|---|---|---|
| Epinephrine (Adrenaline) | Alpha + Beta agonist | Bronchodilates, raises BP, reverses vasodilation | 0.5 mg IM (1:1000) | FIRST DRUG; IM in outer thigh; can repeat after 5 min |
| Chlorphenamine (Piriton) | H1-antihistamine | Blocks histamine H1 receptors → reduces itch, urticaria | 10 mg IV/IM | Causes drowsiness; do not drive |
| Hydrocortisone | Corticosteroid | Anti-inflammatory; prevents late/biphasic reaction | 200 mg IV | Not first-line; supports long-term control |
| Salbutamol | Beta-2 agonist | Bronchodilation | Nebulized | For persistent bronchospasm |
Drugs Used in Hypersensitivity (Allergy)
| Drug | Use |
|---|---|
| Cetirizine, Loratadine (2nd gen antihistamines) | Allergic rhinitis, urticaria — less sedating |
| Montelukast (Leukotriene receptor antagonist) | Asthma, allergic rhinitis |
| Prednisolone (oral corticosteroid) | Severe allergy, autoimmune disease |
| Omalizumab (Anti-IgE antibody) | Severe allergic asthma — reduces free IgE |
18. CLINICAL EXAMPLES
Case 1: Anaphylaxis
A 30-year-old woman receives IV amoxicillin for UTI. Within 5 minutes she develops generalized urticaria, throat tightness, wheezing, and BP drops to 70/40 mmHg.
Diagnosis: Anaphylaxis — Type I hypersensitivity to penicillin
Immediate nursing action: Stop drug → Call help → Lay flat → Adrenaline 0.5 mg IM → O₂ → IV fluids
Case 2: Mantoux (Tuberculin) Test
A 20-year-old nurse undergoes a Mantoux test. At 72 hours, she has induration [raised hardness] of 18 mm.
Interpretation: Positive (≥10 mm in healthcare workers = significant)
Type: Type IV (Delayed) Hypersensitivity
Next step: Chest X-ray + sputum AFB smear to rule out active TB
📝 EXAMINATION QUESTIONS
LONG QUESTIONS (10–15 marks each)
- Classify immunity. Describe innate and adaptive immunity in detail with differences.
- Describe the structure and classes of immunoglobulins. Add a note on their properties and functions.
- Classify and explain hypersensitivity reactions with pathophysiology, clinical examples, and nursing management.
- Describe the cold chain system in immunization. What are cold chain equipment, monitoring tools, and nursing responsibilities in maintaining cold chain?
- Write the national immunization schedule for children under 5 years. Add a note on vaccines for pregnant women and AEFI.
SHORT QUESTIONS (5 marks each)
- Write a note on Type I (anaphylactic) hypersensitivity — mechanism and management.
- Differentiate between active and passive immunity with examples.
- Explain the Gell and Coombs classification of hypersensitivity reactions.
- What is the Vaccine Vial Monitor (VVM)? How is it used?
- Write a short note on serological tests used in clinical practice.
VERY SHORT QUESTIONS (2 marks each)
- Define antigen and antibody.
- What is an epitope?
- Which immunoglobulin crosses the placenta?
- Name the immunoglobulin involved in allergic reactions.
- What is the first drug given in anaphylaxis?
- What is herd immunity?
- Define cold chain.
- What is AEFI? Give one example.
- State two freeze-sensitive vaccines.
- What is the route and dose of BCG vaccine?
MULTIPLE CHOICE QUESTIONS (MCQs)
a) IgG b) IgA c) IgM ✅ d) IgE
a) IgE b) IgG c) Complement d) T lymphocytes ✅
a) Type I b) Type II c) Type III d) Type IV ✅
a) DPT b) TT c) OPV ✅ d) Hepatitis B
a) Hydrocortisone b) Chlorphenamine c) Adrenaline ✅ d) Salbutamol
a) Blood only b) Secretions (saliva, tears, breast milk) ✅ c) Lymph nodes d) Bone marrow
a) DPT b) Hepatitis B c) BCG ✅ d) OPV
a) Use the vaccine b) Keep in freezer c) Discard the vaccine ✅ d) Warm the vaccine
a) Type I b) Type II c) Type III ✅ d) Type IV
a) 3 b) 4 c) 5 ✅ d) 6
(Diphtheria, Pertussis, Tetanus, Hepatitis B, Hib)
ANSWER KEY
| Q | Answer |
|---|---|
| MCQ 1 | c — IgM |
| MCQ 2 | d — T lymphocytes |
| MCQ 3 | d — Type IV |
| MCQ 4 | c — OPV |
| MCQ 5 | c — Adrenaline |
| MCQ 6 | b — Secretions |
| MCQ 7 | c — BCG |
| MCQ 8 | c — Discard vaccine |
| MCQ 9 | c — Type III |
| MCQ 10 | c — 5 diseases |
📄 FINAL 1-PAGE QUICK REVISION SUMMARY
╔══════════════════════════════════════════════════════════════════════════╗
║ IMMUNITY, HYPERSENSITIVITY & IMMUNIZATION — QUICK REVISION ║
╠══════════════════════════════════════════════════════════════════════════╣
║ IMMUNITY ║
║ Innate = fast, non-specific, no memory (skin, phagocytes, NK cells) ║
║ Adaptive = slow, specific, has memory (B cells→antibodies; T cells) ║
║ Active (own antibody, long-lasting) vs Passive (ready-made, short) ║
╠══════════════════════════════════════════════════════════════════════════╣
║ IMMUNOGLOBULINS (GAMED) ║
║ IgG = most abundant, crosses placenta ║
║ IgA = secretions (saliva, milk, tears) ║
║ IgM = first in primary response, pentamer ║
║ IgE = allergy/anaphylaxis (binds mast cells) ║
║ IgD = B-cell surface receptor ║
╠══════════════════════════════════════════════════════════════════════════╣
║ HYPERSENSITIVITY (ACID) ║
║ Type I = IgE + mast cells = Anaphylaxis (<30 min) [Penicillin, pollen] ║
║ Type II = IgG/IgM + complement = Cytotoxic [ABO mismatch, MG] ║
║ Type III = Immune complexes = Tissue damage [SLE, serum sickness] ║
║ Type IV = T cells = Delayed 48-72 hrs [Mantoux, contact dermatitis] ║
╠══════════════════════════════════════════════════════════════════════════╣
║ SEROLOGICAL TESTS ║
║ Widal=Typhoid | VDRL=Syphilis | ELISA=HIV/HepB | Western Blot=HIV confirm║
║ Mantoux = TB | ANA = SLE | Coombs = Hemolytic anemia ║
╠══════════════════════════════════════════════════════════════════════════╣
║ VACCINES ║
║ Live attenuated: BCG, OPV, MMR, Measles (strong, long immunity) ║
║ Killed: IPV, DPT-whole cell, Hepatitis A (multiple doses needed) ║
║ Toxoid: DPT, TT (against bacterial toxin) ║
║ Subunit/Recombinant: HepB, HPV, Pneumococcal, Acellular Pertussis ║
╠══════════════════════════════════════════════════════════════════════════╣
║ COLD CHAIN IMPORTANT FACTS ║
║ Heat-sensitive: OPV, BCG, Measles, MMR (store in freezer) ║
║ Freeze-sensitive: DPT, TT, HepB, IPV, Pentavalent (store +2 to +8°C) ║
║ VVM: inner square LIGHTER = usable ✅ | SAME/DARKER = discard ❌ ║
║ Reconstituted BCG/Measles/MMR: use within 4-6 hours ║
╠══════════════════════════════════════════════════════════════════════════╣
║ NATIONAL IMMUNIZATION SCHEDULE KEY POINTS ║
║ Birth: BCG (ID), OPV-0 (oral), HepB-0 (IM) ║
║ 6, 10, 14 weeks: OPV, Pentavalent, Rotavirus (+PCV & fIPV at 6 & 14 wk)║
║ 9-12 months: MR-1, PCV booster, Vit A ║
║ 16-24 months: DPT B1, OPV B, MR-2, Vit A ║
║ 5-6 years: DPT Booster-2 | 10 & 16 years: Td ║
║ Pregnant women: TT/Td-1 + TT/Td-2 (4 weeks apart) → neonatal tetanus ║
╠══════════════════════════════════════════════════════════════════════════╣
║ ANAPHYLAXIS MANAGEMENT ║
║ FIRST → ADRENALINE 0.5 mg IM (1:1000) outer thigh ║
║ Then: O₂, IV fluids, Chlorphenamine, Hydrocortisone ║
║ Observe 30 min post-vaccination; 6 hrs after anaphylaxis (biphasic) ║
╚══════════════════════════════════════════════════════════════════════════╝