analyse_media
Reading File
Finding Sources
Finding Sources
Searching PubMed
mesenteric panniculitis management treatment
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation of your CT scan report (NECT Abdomen), issued by Dr. Shravan Patil at Krsnaa Diagnostics, Pune.
CT Abdomen Report - Plain Language Explanation
What the Scan Was
This is a Non-Enhanced CT (NECT) of the Abdomen - a CT scan done without contrast dye injection.
Findings Explained
1. Misty Mesentery / Mesenteric Panniculitis (Most Significant Finding)
The report states: "Increased hyperattenuation of the mesenteric fat predominantly along the mesenteric vessels and lymphadenopathy - findings suggestive of misty mesentery / mesenteric panniculitis."
The mesentery is the sheet of fatty tissue that holds your intestines in place and carries blood vessels to them. On CT, normally this fat appears dark (low density). Here it looks abnormally bright/dense ("hyperattenuated") and hazy around the blood vessels - this is called the "misty mesentery" sign.
What this means clinically:
- Mesenteric panniculitis is a benign inflammatory condition affecting the fatty tissue of the mesentery
- It can cause abdominal pain, bloating, nausea, or a feeling of abdominal fullness
- It is usually idiopathic (no clear cause found), but an important note: research from Sleisenger & Fordtran's GI textbook shows an association with malignancy in about 34 out of 49 patients with this CT pattern, so your doctor may want to rule out an underlying lymphoma or other malignancy
- It is found in about 0.6% of abdominal CT scans
- Treatment (when needed) typically involves glucocorticoids (steroids); the condition often resolves on its own
Here is what mesenteric panniculitis looks like on CT (this image matches your report's description):
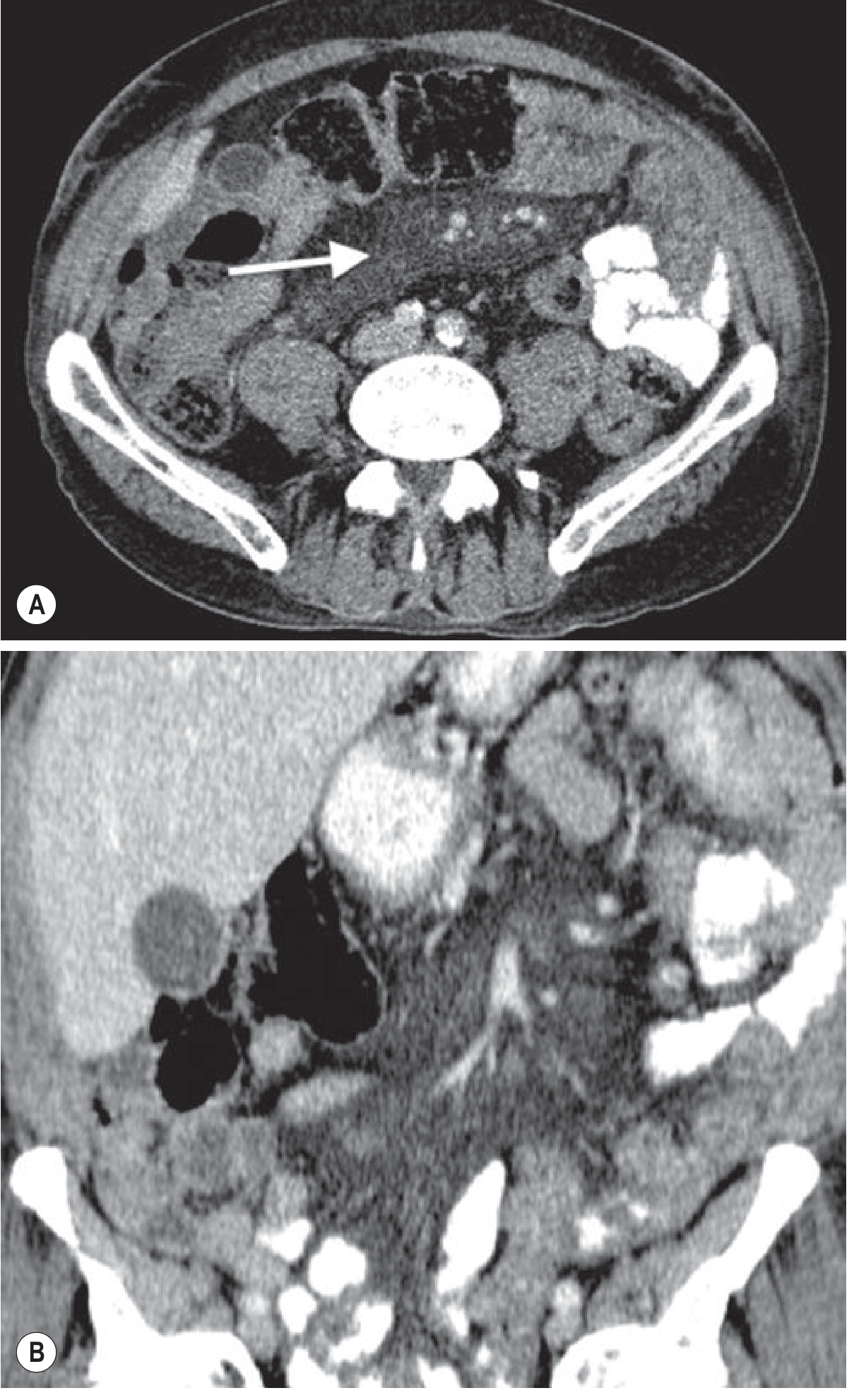
The white arrow points to the hazy, dense mesenteric fat stranding engulfing the mesenteric blood vessels - exactly the CT appearance described in your report. (Source: Grainger & Allison's Diagnostic Radiology)
2. Free Fluid in the Pouch of Douglas (Pelvic Fluid)
"Minimal to mild amount of free fluid noted in the pouch of Douglas. Needs clinical correlation to rule out PID."
- The pouch of Douglas is a small space between the uterus and the rectum - the lowest point of the abdominal cavity in women
- A very small amount of fluid here can be normal around ovulation
- Larger or symptomatic amounts raise concern for Pelvic Inflammatory Disease (PID) - an infection of the uterus, fallopian tubes, or ovaries
- Your doctor will assess this based on your symptoms (pelvic pain, fever, vaginal discharge)
3. Urinary Bladder - Thick and Irregular Walls
"The urinary bladder is distended with thick and irregular walls. Advice urine routine correlation to rule out cystitis."
- Bladder wall thickening can happen when the bladder is very full (an over-distended bladder appears thicker - this can be a normal finding)
- It can also indicate cystitis (bladder infection/UTI) or chronic bladder irritation
- The radiologist recommends a urine routine and culture test to check for infection
- If symptoms like burning urination, frequency, or pelvic discomfort are present, please mention these to your doctor
4. Normal Findings
- Uterus and bilateral adnexa (ovaries/fallopian tubes): unremarkable - these organs look normal
- No pleural effusion - no abnormal fluid around the lungs
5. Incidental / Age-Related Findings
| Finding | What It Means |
|---|---|
| Atherosclerotic calcifications in the aorta | Calcium deposits (hardening) in the main artery - common with age/cardiovascular risk factors |
| Degenerative changes in the spine | Wear-and-tear changes (like arthritis) in the spine - common finding |
| Mild scoliosis with left convexity | Very slight sideways curvature of the spine toward the left - usually minor/benign |
What You Should Do Next
The report strongly advises clinical correlation - this means the radiology findings alone do not confirm any diagnosis. They must be evaluated together with your symptoms and physical examination.
Urgent steps:
- See your treating doctor / gynecologist as soon as possible - bring this report
- Get a urine routine and culture test to check for UTI/cystitis (the report specifically requests this)
- Discuss symptoms of PID with your gynecologist - especially pelvic pain, fever, or unusual discharge
- The mesenteric panniculitis finding is important - your doctor may order blood tests (CBC, CRP, ESR) and may consider ruling out lymphoma given the association reported in literature
- If abdominal pain is significant, a gastroenterologist referral may be appropriate
Important note: A 2024 review in Mayo Clinic Proceedings (PMID 38702129) on sclerosing mesenteritis (the same disease spectrum as mesenteric panniculitis) confirms this is a condition requiring clinical evaluation to guide management - the CT finding alone is not sufficient for a final diagnosis or treatment plan.
This explanation is for informational purposes only and does not replace a consultation with your doctor. Please show this report to your physician, who can examine you and guide further management.
This is a shared conversation. Sign in to Orris to start your own chat.