Direct, indirect, femoral hernia explain route and how to identify, differentiate clinically and test to identify each type
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a thorough, well-illustrated answer. Let me compile it:
Inguinal and Femoral Hernias: Route, Identification, Differentiation, and Clinical Tests
Anatomical Foundation
The three groin hernias all arise in the same small anatomical region but through different defects. The key landmarks are:
- The inferior epigastric vessels (separate direct from indirect)
- The inguinal ligament (separates inguinal from femoral)
- The pubic tubercle (the single most important clinical landmark)

The three sacs side-by-side: indirect inguinal (through deep ring), direct inguinal (through Hesselbach's triangle), and femoral (through femoral canal) - Bailey & Love, 28th Ed.
1. INDIRECT INGUINAL HERNIA
Route
The hernia passes through the deep inguinal ring, which lies in the transversalis fascia midway between the anterior superior iliac spine (ASIS) and the pubic tubercle, approximately 2-3 cm above and lateral to the femoral artery pulse. It then travels obliquely along the inguinal canal, lateral to the inferior epigastric vessels, and exits through the superficial inguinal ring, potentially descending all the way into the scrotum (scrotal hernia).
- Origin: Lateral to inferior epigastric vessels
- Path: Oblique, following the processus vaginalis / spermatic cord
- Can descend into scrotum - distinguishes it from direct hernia
Cause: Congenital (failure of obliteration of processus vaginalis) OR acquired. All childhood inguinal hernias are indirect. - Schwartz's Principles of Surgery, 11th Ed.
Clinical Features
- Common in young males
- Swelling appears in the inguinal region, can extend to scrotum
- Swelling is elliptical/elongated, follows the canal obliquely
- Reducible: contents go up, back, and outward toward the deep ring
- Can strangulate (narrow neck at deep ring)
2. DIRECT INGUINAL HERNIA
Route
The hernia bulges directly forward through Hesselbach's triangle - the weak zone in the posterior wall of the inguinal canal medial to the inferior epigastric vessels. It does not pass through the deep ring. Hesselbach's triangle is bounded by:
- Lateral: inferior epigastric vessels
- Medial: lateral edge of rectus abdominis
- Below: inguinal ligament
It exits through (or bulges toward) the superficial inguinal ring but takes a direct (not oblique) path. It cannot descend into the scrotum. - Bailey & Love, 28th Ed.
Cause: Always acquired - due to weakening and stretching of the transversalis fascia with age, obesity, or raised intra-abdominal pressure.
Clinical Features
- Common in elderly men
- Swelling is broad-based, globular, appears directly forward
- Rarely strangulates (broad neck)
- Does not usually reach the scrotum
- May contain bladder (cystocele in direct hernia)
3. FEMORAL HERNIA
Route
The hernia passes through the femoral canal - the small medial compartment of the femoral sheath - and emerges at the saphenous opening, approximately 1.5 inches (4 cm) below and lateral to the pubic tubercle in the upper thigh. The femoral canal boundaries are:
| Wall | Structure |
|---|---|
| Anterior | Inguinal ligament |
| Posterior | Iliopectineal (Astley Cooper's) ligament / pectineal ligament |
| Lateral | Femoral vein |
| Medial | Lacunar (Gimbernat's) ligament - sharp, unyielding edge |
Once through the femoral canal (a tight space), the hernia expands into loose areolar tissue at the saphenous opening, giving it a retort shape (narrow neck, bulbous fundus). The bulb can then turn upward above the inguinal ligament, making it potentially confused with an inguinal hernia. - S Das Manual on Clinical Surgery, 13th Ed.
Cause: Acquired. The female pelvis widens the femoral canal, making it more common in thin elderly women (F:M = 2:1). However, note: even in women, inguinal hernia is still overall more common than femoral hernia.
Clinical Features
- Right side > left (2:1); 20% bilateral
- Highest strangulation rate of all groin hernias (50% present as emergency) due to the rigid, sharp lacunar ligament medially
- Often small (1-2 cm), easily missed and mistaken for a lymph node
- No cough impulse if irreducible (neck too tight)
Clinical Differentiation - The Key Test: Pubic Tubercle
The single most important landmark for differentiating inguinal from femoral hernia is the pubic tubercle:
| Feature | Inguinal Hernia | Femoral Hernia |
|---|---|---|
| Relation to pubic tubercle | Above and medial | Below and lateral |
| Relation to inguinal ligament | Above | Below |
| Sex | Predominantly male | F > M (though inguinal still commoner even in women) |
| Age | Any (indirect: young; direct: elderly) | Elderly |
| Neck | Narrow (indirect) or broad (direct) | Narrow, rigid - high strangulation risk |
| Reaches scrotum/labium | Yes (indirect) | No |
| Cough impulse | Present | Often absent (rigid neck) |
| Shape | Elongated (indirect) or globular (direct) | Retort-shaped, bulbous |
Clinical Tests to Identify Each Type
The Three-Finger Rule (THIEME Atlas)
Place the thenar eminence on the ASIS, fingers pointing medially and downward:
- Index finger points to the deep inguinal ring → Indirect inguinal hernia
- Middle finger points to Hesselbach's triangle → Direct inguinal hernia
- Ring finger points to the femoral canal → Femoral hernia
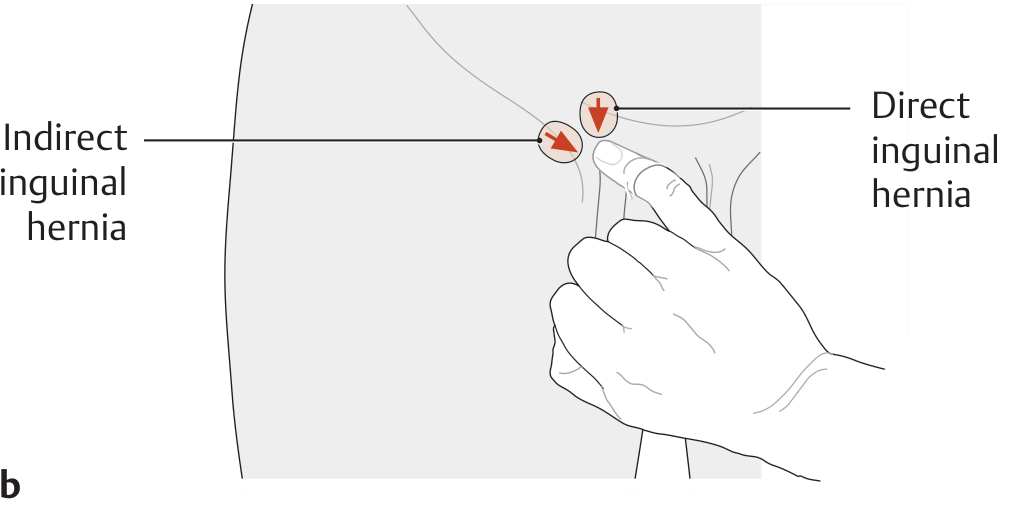
THIEME Atlas: Index finger = direct hernia, middle finger = indirect hernia (the finger directions in this diagram show placement of the examining finger's tip vs. pad for scrotal palpation).
Ring Occlusion Test (Deep Ring Pressure Test)
Purpose: Distinguish indirect from direct inguinal hernia (and from femoral).
Method:
- Reduce the hernia with the patient standing
- Press the thumb firmly over the deep inguinal ring (½ inch above the midpoint between ASIS and symphysis pubis)
- Ask the patient to cough or strain
Interpretation:
- Indirect hernia - controlled (cannot come out) because the deep ring is occluded
- Direct hernia - bulge appears medial to the occluding thumb (the hernia bypasses the deep ring)
- Femoral hernia - bulge appears below the inguinal ligament; can be controlled separately by pressing over the femoral canal / saphenous opening
S Das Manual on Clinical Surgery, 13th Ed.
Invagination (Finger-in-Ring) Test
Method: With the patient standing, invaginate the scrotal skin along the spermatic cord and insert the fingertip up to the superficial inguinal ring. Ask the patient to cough.
Interpretation:
- Impulse felt on the TIP of the finger → Indirect (oblique) hernia (comes down through the deep ring, striking the fingertip)
- Impulse felt on the PULP (pad) of the finger → Direct hernia (bulges straight forward, striking the pad)
Also note the direction the finger naturally travels when entering the ring:
- Goes upward, backward, and outward → Indirect
- Goes directly backward → Direct
S Das Manual on Clinical Surgery, 13th Ed.
Femoral Canal Pressure Test
Method: Apply firm pressure directly over the femoral canal / saphenous opening (4 cm below and lateral to the pubic tubercle) while asking the patient to cough.
Interpretation:
- Femoral hernia - occluded and prevented from bulging out
- Inguinal hernia - unaffected by this pressure
Laparoscopic View
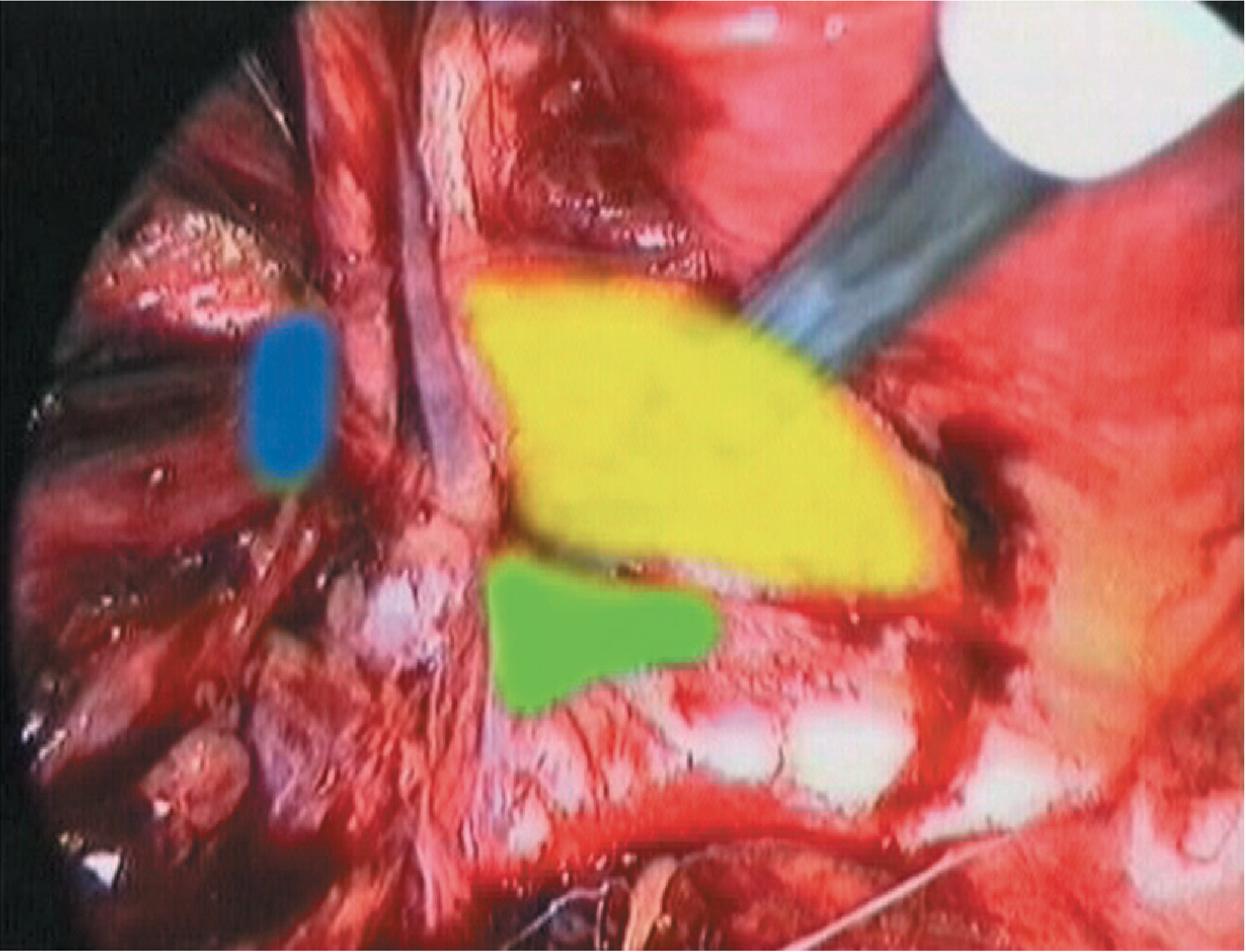
Laparoscopic view: Yellow = Hesselbach's triangle (direct), Blue = lateral/deep ring (indirect), Green = femoral defect - Bailey & Love, 28th Ed.
Summary Comparison Table
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Route | Through deep inguinal ring, oblique along canal | Through Hesselbach's triangle, directly forward | Through femoral canal, below inguinal ligament |
| Relation to epigastric vessels | Lateral | Medial | Below inguinal ligament |
| Relation to pubic tubercle | Above & medial | Above & medial | Below & lateral |
| Neck | Narrow (deep ring) | Broad | Narrow, rigid (lacunar ligament) |
| Strangulation risk | Moderate | Very low | Very high |
| Sex predominance | Male (10:1) | Male, elderly | Female > Male (2:1) |
| Congenital vs acquired | Both | Always acquired | Acquired |
| Descends to scrotum | Yes | No | No |
| Ring occlusion test | Controlled | Not controlled (bulges medially) | Bulges below ligament |
| Finger impulse | Tip of finger | Pad of finger | Not felt in canal |
Differential Diagnosis of Femoral Hernia Swelling
A femoral hernia must be distinguished from: saphena varix (fluid thrill rather than impulse; positive Schwartz's test with percussion of varicosities), enlarged inguinal lymph nodes (firm, no cough impulse), femoral artery aneurysm (expansile pulsatile swelling), and psoas abscess (fluctuant, tracks from the spine, cross-fluctuance possible). - Bailey & Love, 28th Ed.
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed. | S Das A Manual on Clinical Surgery, 13th Ed. | Schwartz's Principles of Surgery, 11th Ed. | THIEME Atlas of General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.