I need 2-3 slides description for abdominal wall mass in rif region like incisional hernia abscess lipoma etc those found in rif region as my slide heading is abdominal wall contents in rif
Slide Deck: Abdominal Wall Masses in the RIF Region
🟦 Slide 1 — Overview & Classification
| Category | Examples |
|---|---|
| Hernias | Incisional hernia, Spigelian hernia, inguinal hernia |
| Infective/Inflammatory | Abdominal wall abscess, psoas abscess |
| Vascular | Rectus sheath hematoma |
| Neoplastic (Benign) | Lipoma, desmoid tumor |
| Neoplastic (Malignant) | Soft tissue sarcoma, metastatic deposit |
🟦 Slide 2 — Hernias in the RIF
Incisional Hernia
- Occurs in ~10–20% of patients following laparotomy; less common after laparoscopy (~0.7%)
- Risk factors: wound infection, obesity, absorbable sutures for fascial closure, transverse incision
- Presents as a reducible or irreducible bulge along or near a previous surgical scar in the RIF (e.g., appendicectomy, right hemicolectomy scar)
- Complications: incarceration, strangulation, bowel obstruction
- Management: mesh repair (laparoscopic or open); mesh overlap is a key determinant in preventing recurrence (Yamada's Textbook of Gastroenterology, 7e; Roberts & Hedges' Clinical Procedures in Emergency Medicine)
Spigelian Hernia
- Uncommon (0.1–2% of ventral hernias); occurs through a defect at the semilunar line (lateral edge of rectus abdominis), typically below the level of the umbilicus → commonly presents in the RIF area
- Often interparietal (between muscle layers) so may not be visible as a bulge — easily missed clinically
- Differential diagnosis includes rectus sheath hematoma, lipoma, or sarcoma
- Diagnosed best on CT or ultrasound; treatment is surgical repair
- Adverse outcomes include recurrence, seroma, hematoma, and infection (Sleisenger & Fordtran's GI and Liver Disease; Sabiston Textbook of Surgery, 21e)
🟦 Slide 3 — Non-Hernia Abdominal Wall Masses in the RIF
Lipoma
- Most common benign soft tissue tumor; arises from subcutaneous or intermuscular fat
- Presents as a soft, lobulated, non-tender, compressible mass — moves with the abdominal wall (not with respiration)
- Important differential from incarcerated hernia (no cough impulse, no expansile cough)
- Confirmed by ultrasound or MRI; excision if symptomatic or diagnostic doubt exists
Abdominal Wall Abscess
- May follow appendicectomy, laparotomy, or trauma in the RIF
- Features: localized tenderness, erythema, fluctuance, fever, raised WBC
- Can arise from a skin/wound infection or as extension of an intraperitoneal collection (e.g., appendix abscess tracking to wall)
- Management: incision and drainage ± antibiotics; CT used to delineate depth and extent
Rectus Sheath Hematoma (RIF variant)
- Caused by rupture of the inferior epigastric artery — commonly in the lower rectus sheath
- Risk factors: anticoagulation, coughing, trauma, post-surgical
- Presents as an acute, tender, firm, non-reducible mass — may mimic appendicitis
- Carnett's sign helps differentiate: tenderness increases on tensing the abdominal muscles (wall origin)
- Confirmed on CT; managed conservatively or with embolization/surgery in large bleeds (Tintinalli's Emergency Medicine; Sabiston Textbook of Surgery; Sleisenger & Fordtran's)
Desmoid Tumor (Fibromatosis)
- Locally aggressive, non-metastasizing fibrous tumor; may arise in the RIF wall, especially after prior surgery (e.g., appendicectomy scar)
- Firm, fixed, non-tender mass; associated with Gardner syndrome / FAP
- CT/MRI for characterization; wide local excision is mainstay of treatment; high recurrence rate
Carnett's test (increased tenderness on muscle contraction) and cough impulse examination help distinguish wall masses from intraperitoneal ones. CT is the gold standard for characterization.
What should be my heading for my slide to describe all these?
- Abdominal Wall Masses in the Right Iliac Fossa
- Swellings of the Abdominal Wall in the RIF
- Abdominal Wall Pathology in the RIF Region
- Differential Diagnosis of RIF Abdominal Wall Swellings
- Abdominal Wall Lesions in the RIF: A Surgical Perspective
- RIF Masses: Abdominal Wall Origin
- Masses in the Right Iliac Fossa: Abdominal Wall Contents
- Right Iliac Fossa Swellings — The Abdominal Wall
"Abdominal Wall Swellings in the Right Iliac Fossa"
For my seminar to present in front of professor as I am jr2 general surgery
Best Heading:
"Abdominal Wall Swellings in the Right Iliac Fossa"
- Uses correct surgical terminology ("swellings" is the standard surgical term, preferred over "masses" or "lumps" in formal presentations)
- Anatomically specific — tells the examiner/professor exactly what you're covering
- Clean, professional, and to the point — no fluff
- Easy to defend when questioned, since it clearly scopes your topic to the wall, separating it from intraperitoneal RIF pathology
"A Surgical Approach to Diagnosis and Management"
Abdominal Wall Swellings in the Right Iliac Fossa A Surgical Approach to Diagnosis and Management
Slide 2 and slide 3 you described please make it more consice
Slide 2 — Hernias of the Abdominal Wall in the RIF
Incisional Hernia
- Occurs after ~10–20% of laparotomies (e.g., appendicectomy, right hemicolectomy scars)
- Risk factors: wound infection, obesity, large incisions, absorbable fascial sutures
- Presents as a reducible bulge at or near scar site; cough impulse positive
- Complications: incarceration, strangulation
- Tx: mesh repair (open or laparoscopic)
Spigelian Hernia
- Defect at the semilunar line, below umbilicus → commonly in RIF
- Often interparietal — no visible bulge, easily missed clinically
- Diagnose with USS or CT
- Tx: surgical repair
Slide 3 — Non-Hernia Abdominal Wall Masses in the RIF
| Condition | Features | Management |
|---|---|---|
| Lipoma | Soft, lobulated, non-tender; moves with wall not respiration; no cough impulse | USS/MRI; excise if doubt |
| Abdominal Wall Abscess | Tender, erythematous, fluctuant; fever; post-op or post-trauma | I&D ± antibiotics; CT if deep |
| Rectus Sheath Hematoma | Acute tender firm mass; anticoagulants/coughing; Carnett's sign +ve | CT to confirm; conservative or embolisation |
| Desmoid Tumor | Firm, fixed, post-surgical scar; linked to FAP/Gardner's | MRI; wide local excision |
Carnett's test — tenderness increases on muscle contraction → confirms abdominal wall origin
some more details in spigelian hernia
Slide 2 — Hernias of the Abdominal Wall in the RIF
Incisional Hernia (as before)
Spigelian Hernia
- Protrudes through the Spigelian fascia — fused aponeurosis of transversus abdominis + internal oblique, lateral to the rectus sheath
- Occurs at the junction of the linea semilunaris and arcuate line (semicircular line of Douglas) — roughly 1/3 to 1/2 of the way between pubic crest and umbilicus → RIF location
- External oblique muscle remains intact overlying the defect → hernia is interparietal, not subcutaneous
- Rare — 0.1–2% of all ventral hernias
- Most diagnosed in the 5th–6th decade; slight female predominance
- Associated with: obesity, chronic cough, connective tissue disorders, smoking
- Pain/tenderness along the linea semilunaris — often no visible bulge
- Examine in supine + standing positions with Valsalva — hernia may be palpable at lateral border of rectus
- Contents: omentum, small bowel, large bowel, appendix, ovary
- Can mimic acute appendicitis or diverticulitis — important differential
- High risk of incarceration and strangulation — must identify and repair promptly
- CT scan preferred (higher PPV than USS; less operator-dependent)
- USS acceptable but limited in obese patients
- If high clinical suspicion persists despite negative imaging → diagnostic laparoscopy
- Surgical repair — open or laparoscopic (TEP/TAPP)
- Low recurrence rate with minimally invasive repair (0–5%)
- Outcomes: seroma, hematoma, infection are rare but recognized complications
not this much
Spigelian Hernia
- Protrudes through the Spigelian fascia (aponeurosis of transversus abdominis + internal oblique) at the linea semilunaris, just below the umbilicus → RIF location
- External oblique remains intact → hernia is interparietal — no visible bulge, easily missed
- 5th–6th decade; associated with obesity, chronic cough
- Contents: omentum, bowel, appendix — can mimic acute appendicitis
- High risk of incarceration & strangulation
- Dx: CT scan preferred; diagnostic laparoscopy if high suspicion despite negative imaging
- Tx: surgical repair (open or laparoscopic); low recurrence (0–5%)
bookish details in one slide
Spigelian Hernia
- Spigelian fascia = fused aponeurosis of internal oblique + transversus abdominis
- External oblique remains intact → hernia lies interparietal (between muscle layers)
- Named after Belgian anatomist Adriaan van den Spiegel
- Rare — only ~1000 cases reported in literature
- 0.1–2% of all ventral hernias
- More common in females; diagnosed in 5th–6th decade
- Pain/tenderness along linea semilunaris with no visible bulge
- Examine supine + standing with Valsalva maneuver
- May mimic appendicitis or diverticulitis
- Contents: omentum, small/large bowel, appendix, ovary
- High risk of incarceration and strangulation
- CT scan (preferred) > Ultrasound
- Diagnostic laparoscopy if imaging negative but suspicion high
- Surgical repair — open or laparoscopic
- Recurrence rate 0–5% with minimally invasive approach
create a good image of spigelian hernia
Medical anatomical diagram of Spigelian hernia showing anterior abdominal wall layers. Labeled diagram showing: rectus abdominis muscle, linea semilunaris, arcuate line (semicircular line of Douglas), Spigelian fascia (fused aponeurosis of internal oblique and transversus abdominis), and the hernia defect protruding through the Spigelian fascia but with intact external oblique muscle overlying it (interparietal hernia). Include a cross-sectional inset showing the layers: skin, external oblique (intact), internal oblique, transversus abdominis, and the hernial sac between layers. Clean medical illustration style with clear labels and arrows, white background.
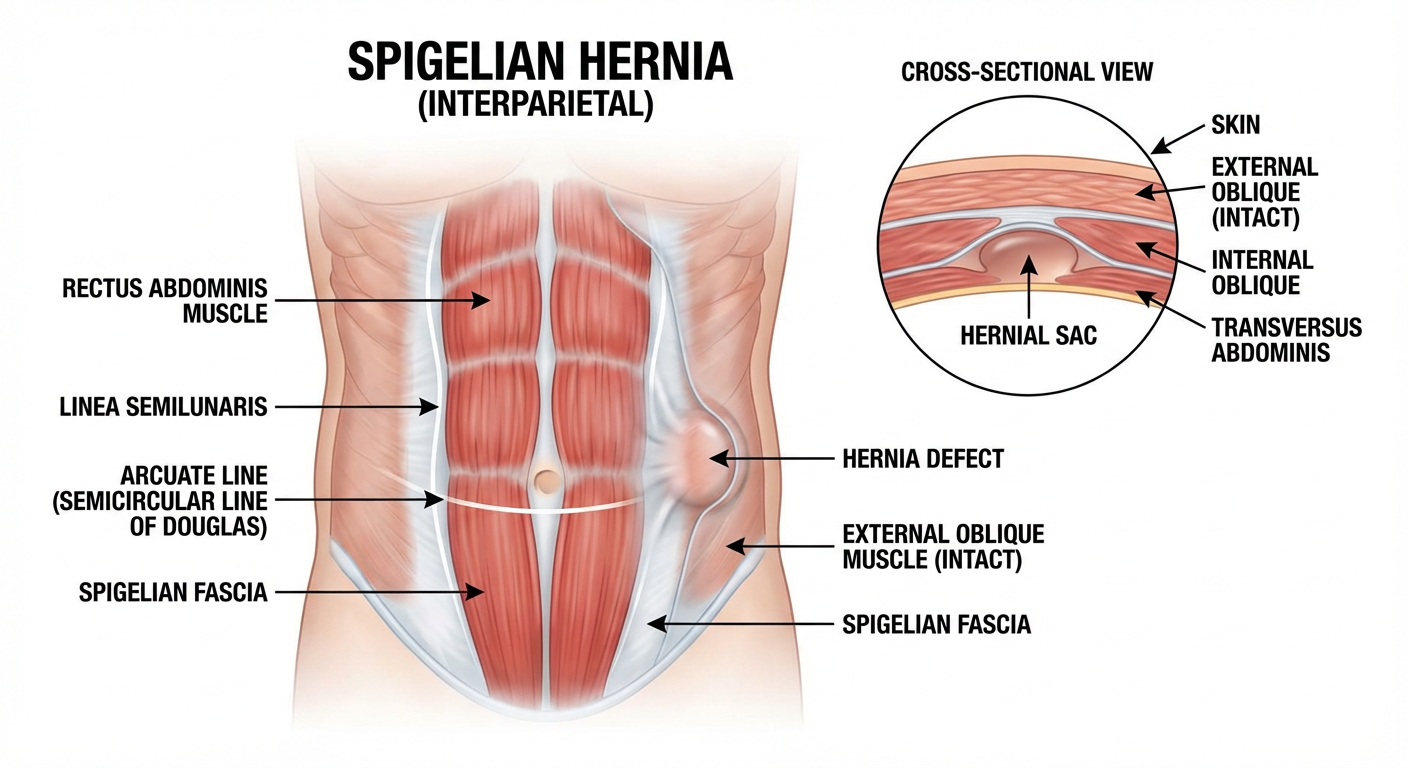
- The hernia defect at the Spigelian fascia, at the junction of the linea semilunaris and arcuate line
- The intact external oblique overlying the defect — explaining why there's no visible bulge
- The interparietal nature of the hernial sac between muscle layers
- Cross-sectional view of the abdominal wall layers
make this image as spigelian hernia should be shown on rif region
Medical anatomical diagram of Spigelian hernia location on the anterior abdominal wall. Show a front view of the human abdomen divided into regions (epigastric, umbilical, hypogastric, right and left iliac fossae, etc.). Highlight and label the Spigelian hernia occurring in the RIGHT ILIAC FOSSA region, at the junction of the linea semilunaris and arcuate line (semicircular line of Douglas), below the umbilicus on the right side. Show the hernia bulge marked clearly in the RIF. Include labels: Linea semilunaris, Arcuate line, Spigelian fascia, Rectus abdominis, Right Iliac Fossa, and an arrow pointing to the hernia site. Add a small inset cross-section showing intact external oblique over the interparietal hernial sac. Clean medical illustration, white background, clear anatomical labels.
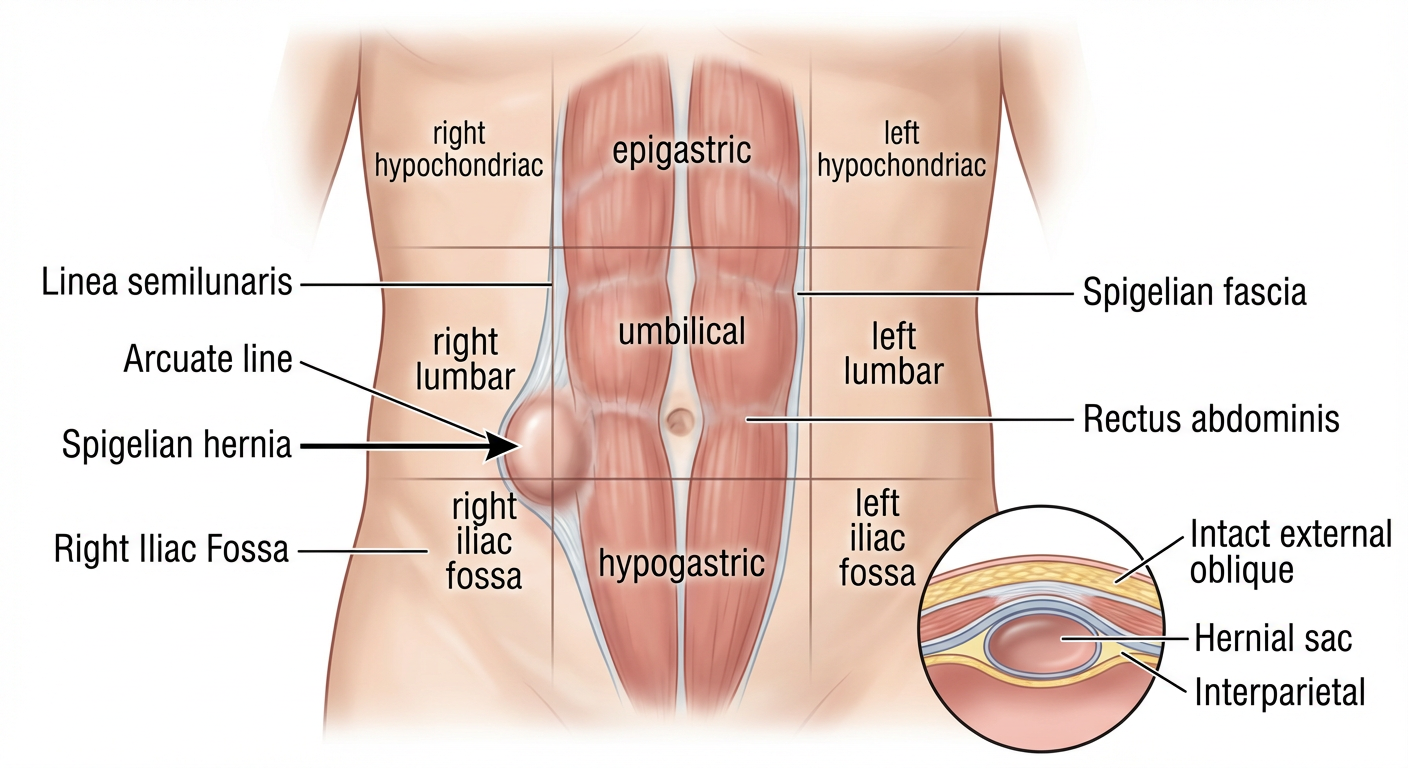
- The Spigelian hernia clearly located in the RIF, below the umbilicus on the right side
- The defect at the junction of linea semilunaris and arcuate line
- Abdominal regions labeled for orientation
- The interparietal nature with intact external oblique shown in the inset