Infective endocarditis
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content to write a thorough answer. Let me compile everything into a well-organized response.
Infective Endocarditis (IE)
Definition
Infective endocarditis is an infection, usually bacterial, of the endocardial surface of the heart - primarily the cardiac valves, though the septa, mural endocardium, and cardiovascular implantable electronic devices (pacemakers, defibrillators) can also be involved. It leads to formation of vegetations composed of thrombotic debris, fibrin, inflammatory cells, and microorganisms, often with underlying tissue destruction.
- Goldman-Cecil Medicine, p. 700
- Robbins & Kumar Basic Pathology, p. 368
Classification
| Type | Course | Key Feature |
|---|---|---|
| Acute IE | Rapid (days) | Destructive infection, high morbidity/mortality even with treatment; often S. aureus |
| Subacute IE | Insidious (weeks-months) | Protracted course, more recoveries with antibiotics; often viridans streptococci |
Note: Many cases fall along a spectrum between these two forms. Modern classification favors categorizing by causative organism, valve involved, and pace of disease.
- Robbins & Kumar Basic Pathology, p. 368
- Goldman-Cecil Medicine, p. 700
Epidemiology
-
Incidence in the US: approximately 10,000-20,000 new cases per year (~1 per 1000 hospital admissions)
-
S. aureus has become the most common cause in most high-income countries due to healthcare-associated infections and the opioid epidemic
-
In developing countries, viridans streptococci still predominate, driven by rheumatic heart disease in younger adults
-
More than one-third of non-drug-using patients with native valve IE have healthcare-associated endocarditis
-
Braunwald's Heart Disease, p. 829-830
-
Goldman-Cecil Medicine, p. 700
Pathogenesis
The disease follows a predictable sequence:
- Endothelial damage - turbulent flow, instrumentation, jet lesions
- Sterile vegetation formation - platelet-fibrin deposits (nonbacterial thrombotic endocarditis, NBTE)
- Transient bacteremia - from dental procedures, IV drug use, gut/oral flora, catheters
- Microbial seeding of the sterile vegetation
- Microbial proliferation and invasion - staphylococci/streptococci adhere avidly and evade host defenses
- Metastatic infection - emboli seed organs receiving high blood flow (kidneys, spleen, brain)
- Goldman-Cecil Medicine, p. 701
- Robbins & Kumar Basic Pathology, p. 368
Predisposing Conditions
More common:
- Mitral valve prolapse (especially with regurgitation) - now the leading pre-existing risk factor
- Degenerative valvular disease
- Injection drug use
- Prosthetic heart valves (10-20% of all IE)
- Prior endocarditis
- Congenital heart disease (uncorrected VSD)
Less common:
- Rheumatic heart disease
- Bicuspid aortic valve / calcific valvular stenosis
- Hypertrophic obstructive cardiomyopathy
- Coarctation of the aorta
Host risk factors: Neutropenia, immunodeficiency, malignancy, diabetes, alcohol use, HIV, end-stage renal disease on hemodialysis
- Goldman-Cecil Medicine, p. 700 (Table 61-1)
- Robbins & Kumar Basic Pathology, p. 368
Microbiology
| Organism | Setting | Notes |
|---|---|---|
| Staphylococcus aureus | Healthcare, IV drug use, community | Most common overall in high-income countries; MRSA in ~47% of healthcare-associated cases; causes acute IE, attacks healthy valves |
| Viridans streptococci (S. viridans group) | Community-acquired | 50-60% of community IE; oral flora; typically subacute on damaged valves |
| Enterococci | Community and nosocomial | ~10% of native and prosthetic valve IE |
| HACEK group | Oral/dental origin | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella - slow-growing gram-negatives |
| Coagulase-negative staphylococci | Early prosthetic valve IE | Common within 60 days of valve surgery |
| S. gallolyticus (formerly S. bovis) | Late PVE, community | Associated with colorectal malignancy |
| Fungi | Immunocompromised, prosthetic valves | Candida, Aspergillus; high mortality |
| Culture-negative | Prior antibiotics, fastidious organisms | ~10-15% of cases; consider Bartonella, Coxiella burnetii, Legionella, Brucella |
- Braunwald's Heart Disease, p. 830
- Robbins & Kumar Basic Pathology, p. 368-369
Morphology (Pathology)
Vegetations are friable, bulky, potentially destructive masses containing fibrin, inflammatory cells, and organisms.
-
Aortic and mitral valves are most common sites (left-sided)
-
Tricuspid valve is commonly involved in IV drug users (right-sided)
-
Vegetations may be single or multiple, involving more than one valve
-
Can erode into underlying myocardium causing ring abscess (paravalvular abscess)
-
Friable vegetations shed emboli leading to septic infarcts and mycotic aneurysms
-
Robbins & Kumar Basic Pathology, p. 368
Clinical Features
Symptoms:
- Fever (most consistent sign - present in ~80-90%)
- Malaise, fatigue, weight loss, night sweats
- Chills, rigors (especially acute IE)
Signs:
| Finding | Description | Mechanism |
|---|---|---|
| New/changing murmur | Present in 90% of left-sided lesions | Valve destruction or regurgitation |
| Splinter hemorrhages | Linear nail bed hemorrhages | Microemboli |
| Petechiae | Conjunctival, palatal, skin | Microemboli/vasculitis |
| Osler nodes | Painful, tender fingertip/toe nodules | Immunologic - immune complex deposition |
| Janeway lesions | Painless erythematous macules on palms/soles | Septic emboli |
| Roth spots | Retinal hemorrhages with pale center | Microemboli |
| Splenomegaly | Common in subacute IE | Prolonged infection |
| Clubbing | Chronic/subacute cases | Chronic infection |
Key mnemonic for peripheral signs: FROM JANE - Fever, Roth spots, Osler nodes, Murmur, Janeway lesions, Anemia, Nail (splinter) hemorrhages, Emboli
- Robbins & Kumar Basic Pathology, p. 368-369
- Goldman-Cecil Medicine, p. 702 (Table 61-2)
Echocardiography in IE
Here is TTE demonstrating aortic valve IE - vegetations on left ventricular aspects of cusps prolapsing into LVOT during diastole (Panel A), with severe aortic regurgitation on color Doppler (Panel B):
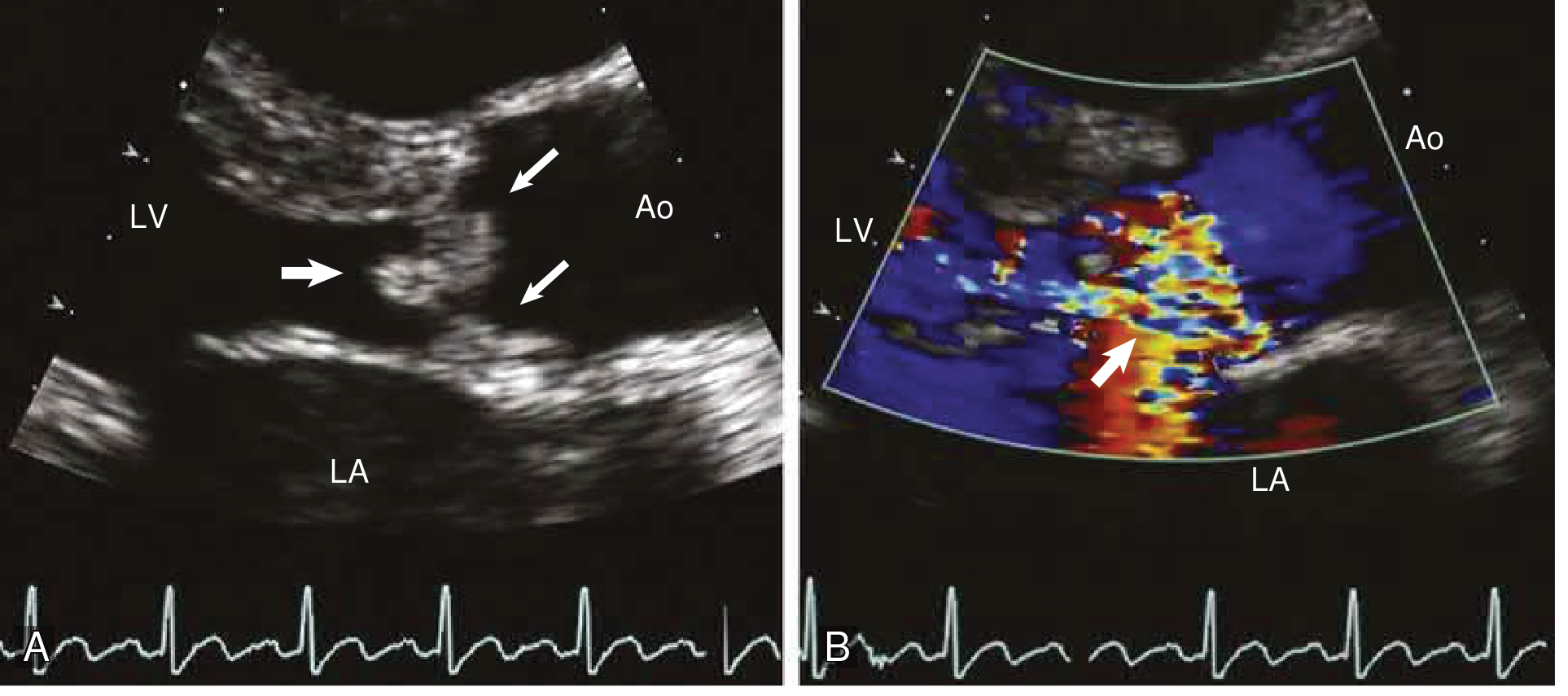
Braunwald's Heart Disease - Aortic valve IE: vegetations (small arrows) attached to LV aspects of valve cusps, prolapsing into LVOT (large arrow) during diastole; B: severe aortic regurgitation (arrow) on color Doppler. LV = left ventricle, LA = left atrium, Ao = ascending aorta.
TTE vs TEE:
-
TTE is the first test in most patients
-
TEE is preferred when: TTE is non-diagnostic, prosthetic valve involved, high clinical suspicion with negative TTE, or complicated IE (paravalvular abscess suspected)
-
TEE has higher sensitivity (~90-95%) vs TTE (~40-60%) for vegetations
-
Braunwald's Heart Disease, p. 831
Modified Duke Criteria (Diagnosis)
Definite IE: 2 major criteria, OR 1 major + 3 minor, OR 5 minor criteria
Possible IE: 1 major + 1 minor, OR 3 minor criteria
Rejected: Firm alternate diagnosis, resolution on ≤4 days antibiotics, or criteria not met
Major Criteria
-
Positive blood cultures for IE:
- Typical organisms (viridans streptococci, S. gallolyticus, S. aureus, HACEK, community-acquired enterococci) from ≥2 separate cultures, OR
- Persistently positive: ≥2 cultures drawn >12 hr apart, OR ≥3 of ≥4 cultures (first and last ≥1 hr apart), OR
- Single positive culture for Coxiella burnetii OR anti-phase I IgG ≥1:800
-
Evidence of endocardial involvement on echocardiography:
- Oscillating intracardiac mass (vegetation) on valve/supporting structures, OR
- Abscess, OR
- New partial dehiscence of prosthetic valve
- New valvular regurgitation (worsening of existing murmur alone does NOT qualify)
Minor Criteria
- Predisposing heart condition or IV drug use
- Fever >38°C
- Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Microbiologic evidence: positive blood culture not meeting major criteria
- Braunwald's Heart Disease, p. 151-192 (Modified from Li JS et al. Clin Infect Dis. 2000;30:633)
- Washington Manual of Medical Therapeutics, p. 5471
Diagnostic Workup
-
Blood cultures (3 sets from different sites before antibiotics) - cornerstone of diagnosis
-
Echocardiography (TTE then TEE as needed)
-
CBC: Normochromic normocytic anemia in subacute IE; leukocytosis in 50-60% (more in acute)
-
Inflammatory markers: ESR elevated in 61%; CRP elevated
-
Urinalysis: Hematuria (immune complex glomerulonephritis), proteinuria
-
Thrombocytopenia (~10%) - predictor of early adverse outcome
-
PCR techniques - for culture-negative cases (fastidious organisms)
-
18F-FDG PET/CT - increasingly used in prosthetic valve IE for paravalvular extension and metastatic foci
-
Braunwald's Heart Disease, p. 830
Antibiotic Treatment
Treatment is prolonged IV antibiotic therapy (4-6 weeks for most cases), targeted to the organism:
| Organism | Preferred Regimen | Duration |
|---|---|---|
| Viridans streptococci (PCN-susceptible) | Penicillin G or ceftriaxone | 4 weeks |
| S. aureus (MSSA) native valve | Nafcillin or oxacillin ± gentamicin | 6 weeks |
| MRSA | Vancomycin | 6 weeks |
| Enterococci | Ampicillin + gentamicin (if susceptible) | 4-6 weeks |
| HACEK | Ceftriaxone | 4 weeks |
| Fungal | Amphotericin B ± azole; often surgery required | Prolonged |
Blood cultures should be repeated 48-72 hours after starting treatment to document clearance.
Complications
| Complication | Notes |
|---|---|
| Heart failure | Most common indication for surgery; new/worsening valve dysfunction |
| Systemic emboli | Brain (stroke), kidneys, spleen, coronary arteries |
| Paravalvular abscess | Extension of infection; new AV block on ECG is a warning sign |
| Mycotic aneurysm | Bacterial infection of arterial wall at embolization sites |
| Glomerulonephritis | Immune complex deposition; hematuria, renal failure |
| Neurologic complications | Embolic stroke, mycotic aneurysm, brain abscess, meningitis |
| Septic metastatic infection | Abscesses in brain, spleen, kidneys |
| Conduction system disease | Abscess extension into septum/AV node |
- Robbins & Kumar Basic Pathology, p. 369
- Harrison's Principles of Internal Medicine 22E, p. 1362
Surgical Indications and Timing
Between 25-40% of left-sided IE patients require surgery during active infection.
| Timing | Indications |
|---|---|
| Emergent (same day) | Valve dysfunction with pulmonary edema or cardiogenic shock; acute AR with preclosure of mitral valve; sinus of Valsalva abscess ruptured into right heart; rupture into pericardial sac |
| Urgent (1-2 days) | Valve obstruction by vegetation; unstable dehisced prosthesis; acute AR or MR with NYHA class III-IV HF; septal perforation; paravalvular extension with new conduction abnormalities; no effective antibiotic therapy available |
| Elective | Progressive paravalvular prosthetic regurgitation; valve dysfunction with persistent infection after >7-10 days of antibiotics; fungal (mold) endocarditis; Candida endocarditis; antibiotic-resistant organisms |
| Consider urgently | Vegetation >10 mm with severe valve dysfunction; major embolus + persisting large vegetation (>10 mm); mobile vegetation >30 mm |
Surgery for NVE appears to convey a 27-55% survival benefit when current indications are met.
- Harrison's Principles of Internal Medicine 22E, p. 1355-1362
Prophylaxis (2021 AHA Update)
Antibiotic prophylaxis is recommended only for highest-risk patients undergoing invasive dental procedures:
High-risk conditions:
- Prosthetic cardiac valve (including transcatheter-implanted)
- Prior history of IE
- Unrepaired cyanotic congenital heart disease, or within 6 months of repair
- Cardiac transplant with valvulopathy
- Ventricular assist devices and implantable hearts (new in 2021)
- Cardiac valve repair with devices/annuloplasty rings
Preferred regimen: Amoxicillin 2g PO 30-60 min before procedure
2021 updates:
-
Allergy screening recommended - 90% of "penicillin-allergic" patients test negative; use amoxicillin in these
-
Clindamycin is no longer recommended as an alternative (risk of C. difficile)
-
Doxycycline added as alternative in truly penicillin-allergic patients
-
Braunwald's Heart Disease, p. 831
Prognosis
- Untreated IE is nearly uniformly fatal
- With appropriate antibiotics ± surgery, in-hospital mortality is ~15-25% for NVE; higher for PVE
- Predictors of worse prognosis: S. aureus, prosthetic valve, large vegetations, embolic events, heart failure, abscess formation, thrombocytopenia, renal failure
- Relapse rates: ~5% in NVE, higher in PVE and fungal IE
Sources: Braunwald's Heart Disease (10th ed.), Robbins & Kumar Basic Pathology, Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E (2025), Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.