What is menopause explain its complications
Reading File
Finding Sources
Searching the Web
menopause definition complications cardiovascular osteoporosis 2024
Searching PubMed
"menopause"[MeSH Terms] AND "complications"
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have rich, detailed content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Menopause: Definition, Physiology, and Complications
Definition
Menopause is the permanent cessation of menstruation, defined clinically as 12 consecutive months of amenorrhea resulting from the decline and ultimate failure of ovarian function. It is the culmination of reproductive aging and typically occurs in the fifth to sixth decades of life, with a median age of 51-52.5 years. The period leading up to menopause (usually 2-10 years of irregular cycles) is called perimenopause or the menopausal transition.
- Goldman-Cecil Medicine, p. 3958
- Guyton & Hall Medical Physiology, p. 1028
Types of Menopause
| Type | Description |
|---|---|
| Natural menopause | Spontaneous cessation due to follicular exhaustion |
| Premature menopause | Before age 40 (also called Primary Ovarian Insufficiency) |
| Surgical menopause | Bilateral oophorectomy - causes abrupt menopause |
| Induced menopause | Chemotherapy or pelvic radiation damaging ovaries |
| Perimenopause | Transition phase with irregular cycles, rising FSH |
Pathophysiology
The fundamental mechanism involves progressive depletion of primordial follicles. A woman is born with ~1-2 million follicles; by puberty ~300,000 remain; by age 45-50, only a few hundred remain. When the follicle pool nears exhaustion:
- Estrogen and progesterone production falls dramatically
- FSH rises markedly (loss of negative feedback) - FSH is the most sensitive marker
- LH rises moderately
- Without follicle stimulation, ovulation ceases permanently
- The small amount of estrogen still produced comes from peripheral aromatization of androstenedione in adipose tissue - this becomes the primary estrogen source after menopause
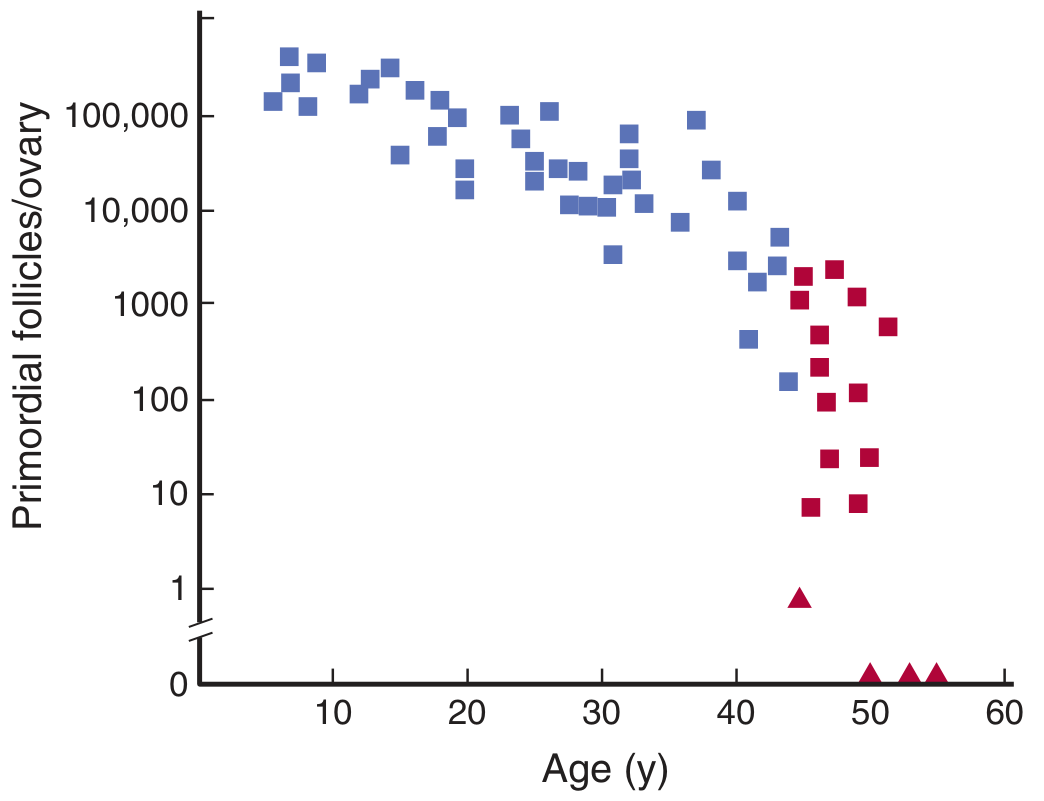
Ganong's Review of Medical Physiology, Fig. 22-14 - note follicle counts collapse to near-zero by the time of menopause
Symptoms of Menopause
Vasomotor Symptoms
- Hot flushes/flashes - occur in ~75% of menopausal women; may persist for up to 40 years. They coincide with LH secretion surges. An estrogen-sensitive hypothalamic event triggers both the LH burst and the flush simultaneously.
- Night sweats - nocturnal hot flushes causing disrupted sleep
- Palpitations
Genitourinary Syndrome of Menopause (GSM)
- Vaginal dryness, atrophy, and dyspareunia
- Urinary urgency, frequency, and recurrent UTIs
- Atrophy of the uterus and vagina
Neuropsychological Symptoms
- Irritability and mood changes
- Anxiety and depression
- Cognitive changes / "brain fog"
- Fatigue
- Sleep disturbances
Sexual Dysfunction
- Decreased libido
- Dyspareunia (from vaginal dryness)
Musculoskeletal
- Joint aches and myalgia
- Decreased muscle mass
Complications of Menopause
1. Osteoporosis
This is one of the most serious long-term complications. Estrogen normally inhibits osteoclast activity and promotes osteoblast survival. With estrogen loss:
- Accelerated bone resorption occurs (osteoclasts become overactive)
- Bone mineral density (BMD) decreases at ~2-3% per year in the first few years after menopause
- Trabecular bone (spine, wrist) is lost faster than cortical bone
- Risk of vertebral, hip, and wrist fractures rises sharply
- Hip fractures carry 15-20% mortality in the first year
- Postmenopausal women with osteoporosis also have proportionally increased cardiovascular event risk
2. Cardiovascular Disease (CVD)
CVD is the leading cause of death in postmenopausal women. Estrogen is cardioprotective:
- Maintains favorable lipid profile (raises HDL, lowers LDL)
- Promotes endothelial vasodilation via nitric oxide
- Has anti-inflammatory and antioxidant effects on vessel walls
After menopause:
- LDL increases, HDL falls
- Blood pressure tends to rise
- Risk of coronary artery disease, myocardial infarction, and stroke increases significantly
- Women with early menopause (<45 years) have disproportionately higher cardiovascular risk
- The AHA Scientific Statement confirms CVD risk notably increases after the menopausal transition
3. Dementia and Cognitive Decline
- Estrogen has neuroprotective effects (promotes synaptic plasticity, reduces amyloid accumulation)
- Postmenopausal estrogen deficiency is associated with increased risk of Alzheimer's disease and vascular dementia
- The "critical window" hypothesis suggests early estrogen replacement may be protective; late initiation may increase risk
4. Urogenital Atrophy / Genitourinary Syndrome
- Vaginal epithelium thins, loses rugae, and becomes dry (atrophic vaginitis)
- Bladder neck and urethral atrophy → stress incontinence, urgency incontinence
- Recurrent urinary tract infections due to loss of protective acidic vaginal flora
5. Weight Gain and Metabolic Syndrome
- Central (abdominal) fat redistribution after menopause
- Insulin resistance increases
- Higher risk of type 2 diabetes mellitus
- Metabolic syndrome risk rises significantly
6. Mood Disorders and Depression
- Estrogen modulates serotonin and dopamine pathways
- Increased rates of depression and anxiety during perimenopause and early post-menopause
- Sleep disruption from night sweats compounds mood disturbances
7. Increased Cancer Risk
- Endometrial cancer: Unopposed estrogen (from exogenous sources or adipose aromatization) without progesterone increases endometrial hyperplasia and cancer risk
- Colorectal cancer: Postmenopausal women have higher rates compared to premenopausal
- Note: Ovarian cancer risk also rises with age through this period
8. Skin and Hair Changes
- Skin becomes thinner, drier, loses collagen (up to 30% of skin collagen lost in first 5 years post-menopause)
- Hair thinning and scalp alopecia
- Increased facial hair (relative androgen excess)
Factors That Affect Age at Menopause
- Earlier menopause: Smoking (1-2 years earlier), low socioeconomic status, African American or Hispanic ethnicity, genetic factors (CYP3A4, MSH6 mutations), endocrine-disrupting chemicals, high altitude
- Later menopause: Oral contraceptive use, Asian ethnicity, higher parity
Diagnosis
- Clinical: 12 months of amenorrhea in a woman ~45-55 years (no testing usually needed)
- FSH > 40 mIU/mL (elevated on 2 occasions, 4-6 weeks apart) confirms menopause
- Estradiol < 20 pg/mL
- For women < 40: rule out pregnancy, thyroid disease, hyperprolactinemia before diagnosing premature ovarian insufficiency
Management
| Symptom/Complication | Treatment |
|---|---|
| Hot flashes (moderate-severe) | Hormone therapy (HRT) - most effective; or SSNRIs (venlafaxine), SSRIs, gabapentin, clonidine |
| GSM | Topical vaginal estrogen, ospemifene, lubricants |
| Osteoporosis prevention | Weight-bearing exercise, calcium/Vit D, bisphosphonates if high risk |
| Osteoporosis treatment | Bisphosphonates (alendronate), denosumab, raloxifene, teriparatide |
| Cardiovascular risk | Lifestyle modification, statin if indicated |
| Mood disorders | Psychotherapy, antidepressants, HRT if concurrent vasomotor symptoms |
Hormone Replacement Therapy (HRT) - reverses many symptoms effectively but carries risks:
- Benefits: Reduces hot flashes, prevents bone loss, may reduce CVD risk if started early ("timing hypothesis")
- Risks: Increased risk of breast cancer (combined estrogen-progestogen), venous thromboembolism, stroke - these risks must be weighed individually
- Current evidence: If started before age 60 or within 10 years of menopause onset, benefits generally outweigh risks in low-risk women
Sources:
- Goldman-Cecil Medicine (International Ed.), Chapter 222 - Menopause (Santoro & Neal-Perry)
- Guyton & Hall Textbook of Medical Physiology, p. 1027-1028
- Ganong's Review of Medical Physiology (26th Ed.), p. 686-701
- StatPearls - Menopause, NIH
- AHA: Menopause Transition and Cardiovascular Disease Risk
This is a shared conversation. Sign in to Orris to start your own chat.