Approach to proteinuria
Reading File
Finding Sources
Finding Sources
Searching PubMed
proteinuria evaluation management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have comprehensive content from multiple authoritative sources. Let me compile the full response:
Approach to Proteinuria
Normal Protein Excretion
Normal urine protein excretion is less than 150 mg/day, composed primarily of:
- Uromodulin (Tamm-Horsfall protein) - the dominant fraction
- Albumin: <30 mg/day (the kidneys filter ~4-8 g albumin/day, with nearly all reabsorbed by megalin/cubilin in the proximal tubule)
- Low-molecular-weight proteins (10-20 mg/day) and secreted proteins like IgA (40-60 mg/day)
Mechanisms / Types of Proteinuria
Proteinuria arises through four distinct mechanisms, each with different clinical implications:
1. Glomerular Proteinuria
The glomerular filtration barrier has three layers: fenestrated endothelium (coated with glycocalyx), the glomerular basement membrane (GBM, with heparan sulfate proteoglycans providing charge selectivity), and podocyte foot processes linked by slit diaphragms (nephrin, podocin) providing size selectivity. Defects in any of these result in:
- Predominantly albuminuria (albumin is large, 70 kDa, and anionic)
- Can range from microalbuminuria to nephrotic-range proteinuria (>3.5 g/day)
- Causes: minimal change disease, FSGS, membranous nephropathy, MPGN, IgA nephropathy, lupus nephritis, diabetic nephropathy, Alport syndrome
Glomerular proteinuria is further subclassified as:
| Subtype | Description |
|---|---|
| Functional/transient | Fever, exercise, heart failure, hyperadrenergic states - hemodynamic; benign |
| Orthostatic | Proteinuria only in upright position; absent in early-morning (recumbent) urine; total <1 g/day; normal biopsy; excellent prognosis |
| Fixed nonnephrotic | Persistent; GFR may be preserved; if <0.5 g/day biopsy not mandatory; if >1 g/day, consider biopsy especially after ACE-I/ARB trial |
| Nephrotic range | >3.5 g/day; virtually always glomerular; triggers full workup |
2. Tubular Proteinuria
- Low-molecular-weight proteins (<25 kDa): β₂-microglobulin, retinol-binding protein, α₁-microglobulin
- Normally filtered freely but reabsorbed in the proximal tubule; appear in urine when tubule is damaged
- Usually <2 g/day; dipstick may be negative (dipstick detects intact albumin only)
- Causes: tubulointerstitial nephritis, heavy-metal poisoning (lead, cadmium), Dent disease, Lowe syndrome, Fanconi syndrome, pyelonephritis, ATN
- Tubular proteinuria alongside glomerular proteinuria is an adverse prognostic sign indicating tubulointerstitial damage
3. Overflow Proteinuria
- Occurs when an excess of low-molecular-weight proteins is produced, overwhelming normal tubular reabsorption
- Dipstick negative (non-albumin proteins); SSA test positive
- Causes:
- Immunoglobulin light chains (Bence Jones protein) - multiple myeloma
- Lysozyme - myelomonocytic leukemia
- Myoglobin - rhabdomyolysis
- Free hemoglobin - intravascular hemolysis
- Key clue: SSA strongly positive + dipstick negative
4. Postrenal (Post-glomerular) Proteinuria
- From inflammation, infection, irritation, or malignancy of the collecting system (renal pelvis, ureters, bladder, prostate)
- Typically low-level, non-albumin, transient
Quantification of Proteinuria
| Test | Normal | Microalbuminuria | Proteinuria | Nephrotic Range |
|---|---|---|---|---|
| 24-h urine protein | <150 mg | -- | 150-3500 mg | >3500 mg |
| 24-h albumin | 8-10 mg | 30-300 mg | >300 mg | >3500 mg |
| Albumin/creatinine ratio (ACR) | <30 mg/g | 30-300 mg/g | >300 mg/g | >3000-3500 mg/g |
| Protein/creatinine ratio (PCR) | <0.2 | -- | >0.2 | >3-3.5 |
| Dipstick | Negative | Trace/1+ | Trace-3+ | 3-4+ |
Preferred test: Spot urine protein-to-creatinine ratio (or ACR) is as accurate as 24-h collection and far more convenient. Results correlate well with 24-h excretion rates.
Dipstick pitfalls:
- False positives: alkaline urine (pH >8), iodinated contrast, cephalosporins, chlorhexidine, concentrated urine
- False negatives: dilute urine, non-albumin proteins (Bence Jones, myoglobin)
- Requires confirmation: a 2+ or greater is highly suggestive; trace/1+ is only predictive if specific gravity <1.025
SSA (sulfosalicylic acid) test: Detects all proteins (sensitivity 5-10 mg/dL). SSA positive + dipstick negative = overflow proteinuria (light chains, myoglobin, etc.)
Clinical Evaluation - Step-by-Step
Step 1: Confirm and Quantitate
- Repeat dipstick to confirm (exclude transient causes: fever, exercise, dehydration, UTI)
- Spot urine PCR or ACR
- Consider 24-h urine only if body habitus is unusual (low or high muscle mass) affecting creatinine generation
Step 2: Categorize by Amount
- Microalbuminuria (ACR 30-300 mg/g): primarily for DM/HTN screening - marker of cardiovascular and renal risk
- Nonnephrotic proteinuria (<3.5 g/day): wide differential; may be glomerular, tubular, overflow, or functional
- Nephrotic-range proteinuria (>3.5 g/day): virtually diagnostic of glomerular disease
Step 3: History and Examination
- DM (duration, control), hypertension, SLE, HIV, hepatitis B/C, amyloidosis, malignancy
- Drug history (NSAIDs, lithium, heavy metals, heroin, penicillamine, gold)
- Family history (Alport syndrome, polycystic kidney disease)
- Symptoms: frothy urine, edema, hematuria, hypertension, oliguria
Step 4: Baseline Investigations
- Urine: dipstick + microscopy (casts? red cells? granular casts?), 24-h protein or spot PCR/ACR, urine electrophoresis (if overflow suspected)
- Blood: serum creatinine/eGFR, electrolytes, albumin, lipid profile, glucose/HbA1c, CBC
- Serologies (if glomerular disease suspected): ANA, anti-dsDNA, ANCA (MPO, PR3), anti-GBM, complement (C3, C4), hepatitis B/C, HIV, SPEP/UPEP (myeloma screen), cryoglobulins, ASO titre
- Imaging: renal ultrasound (size, echogenicity, obstruction)
Step 5: Classify the Proteinuria Pattern
Check for associated findings:
- Proteinuria + hematuria + RBC casts + hypertension → nephritic pattern → glomerulonephritis
- Proteinuria >3.5 g + hypoalbuminemia + edema + hyperlipidemia → nephrotic syndrome
- Proteinuria + reduced GFR → CKD evaluation + consider biopsy
- Proteinuria alone (no hematuria, normal GFR, normal BP) → isolated proteinuria pathway (see flowchart below)
Evaluation Flowchart for Isolated Asymptomatic Proteinuria
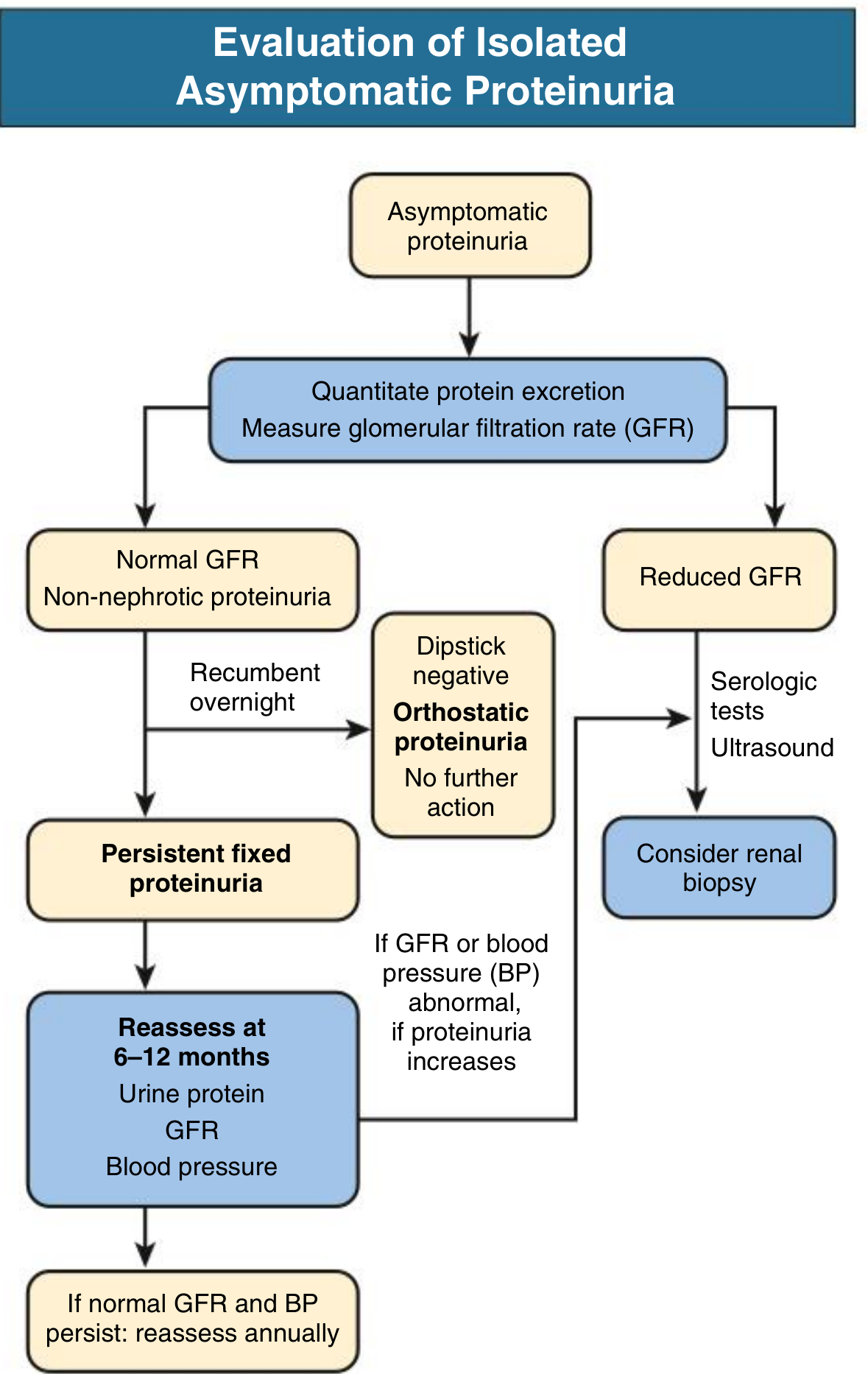
From Comprehensive Clinical Nephrology, 7th Edition
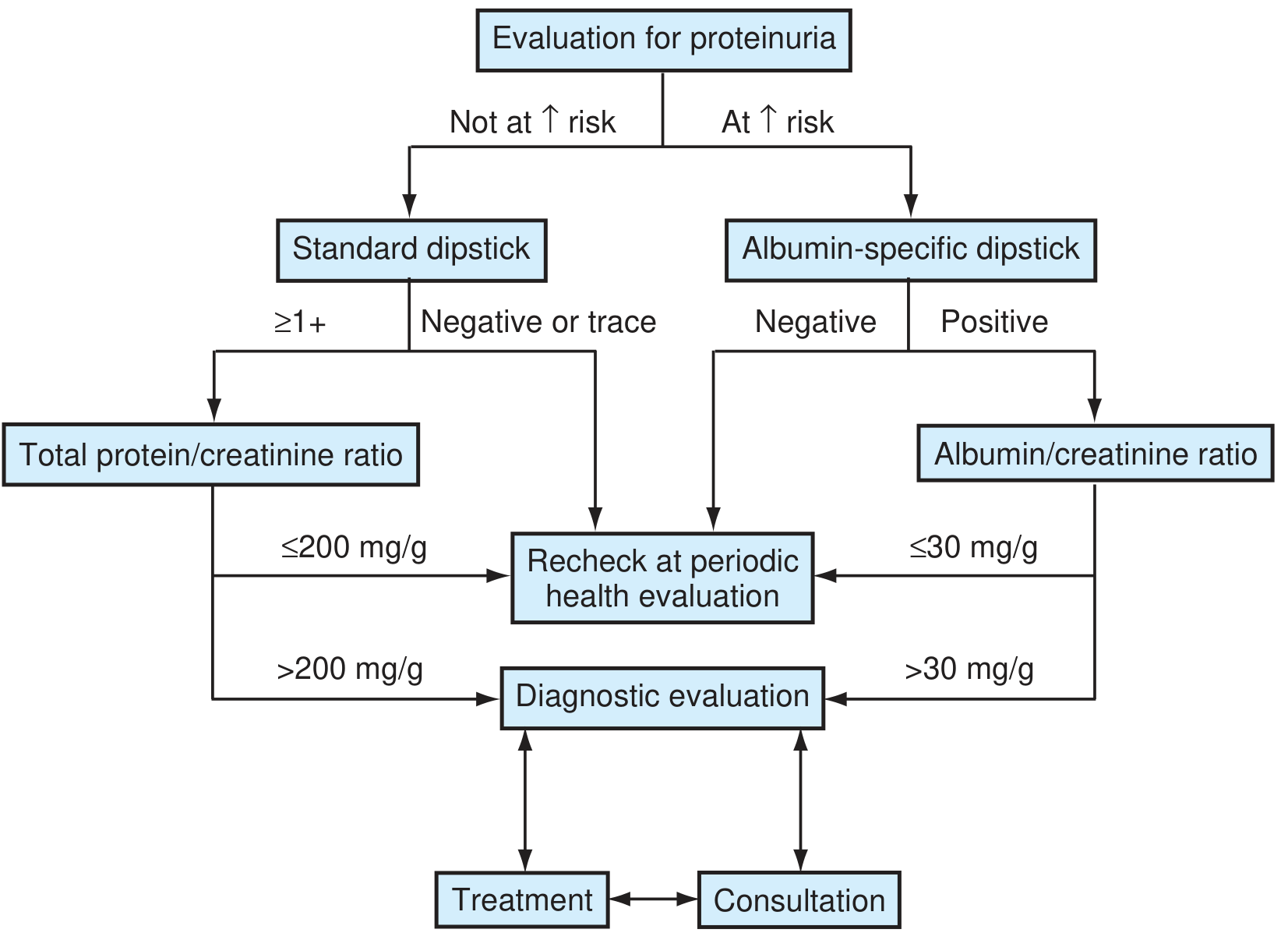
From Textbook of Family Medicine, 9e
When to Biopsy?
| Scenario | Biopsy? |
|---|---|
| Orthostatic proteinuria | Not indicated - prognosis excellent |
| Fixed proteinuria <0.5-1 g/day, normal GFR, normal BP | Not indicated; monitor |
| Fixed proteinuria >1 g/day, especially post ACE-I/ARB | Consider biopsy |
| Proteinuria + hematuria + casts or declining GFR | Biopsy often indicated even at 0.5-1 g/day |
| Nephrotic syndrome | Usually requires biopsy (except in children <10y with classic MCD presentation) |
| Reduced GFR + proteinuria | Serologic tests + ultrasound first; then biopsy |
Proteinuria in Special Populations
Diabetes
- Screen annually with ACR
- Microalbuminuria (ACR 30-300 mg/g) = moderately increased albuminuria; start ACE-I or ARB
- Macroalbuminuria (ACR >300 mg/g) = severely increased albuminuria; optimize RAAS blockade, BP <130/80
Children
- Most transient when followed over weeks
- Persistent = present in ≥2 of 3 weekly samples
- Orthostatic proteinuria most common benign cause - confirmed by normal first-morning (recumbent) urine PCR
- Nephrotic syndrome in children: first presentation at age 1-10 years often treated empirically with steroids (presumed MCD) without biopsy
Management Principles
-
Treat the underlying cause (immunosuppression for GN, antivirals for HBV/HCV-related nephropathy, treat myeloma, etc.)
-
RAAS blockade is the cornerstone of antiproteinuric therapy:
- ACE inhibitor or ARB reduces intraglomerular pressure and directly decreases proteinuria
- Titrate to maximum tolerated dose
- Reduces TGF-β expression, limiting tubulointerstitial fibrosis
- Angiotensin II directly reduces nephrin expression in podocytes - blockade partially restores this
- Target: minimize proteinuria (reduction in proteinuria is itself a therapeutic goal)
-
Blood pressure control: target <130/80 mmHg (lower in heavy proteinuria); additional antihypertensives added to RAAS blockade if needed
-
Sodium restriction: reduces RAAS activation, enhances antiproteinuric effect of RAAS blockers
-
Monitoring: reassess urine protein, GFR, and BP every 6-12 months if stable; increase frequency if declining
-
Nephrology referral: when proteinuria >1-2 g/day, when hematuria or GFR decline is present, when biopsy is being considered, or when etiology is unclear
Key Causes of Pathologic Proteinuria (Summary Table)
| Category | Causes |
|---|---|
| Primary glomerular | Minimal change disease, FSGS, membranous nephropathy, MPGN, IgA nephropathy |
| Secondary glomerular | Diabetic nephropathy, lupus nephritis, amyloidosis, hypertensive nephropathy, postinfectious GN, ANCA vasculitis |
| Tubular/interstitial | Tubulointerstitial nephritis, obstructive uropathy, reflux nephropathy, ATN, heavy metal toxicity |
| Overflow | Multiple myeloma (Bence Jones), rhabdomyolysis, hemolysis |
| Functional | Exercise, fever, heart failure, stress |
| Orthostatic | Young patients, benign, position-dependent |
Sources: Comprehensive Clinical Nephrology 7e, National Kidney Foundation Primer on Kidney Diseases 8e, Brenner and Rector's The Kidney, Harrison's Principles of Internal Medicine 22e, Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.