Why coma occurs in myxedema
Why Coma Occurs in Myxedema
1. Direct Effect of Thyroid Hormone Deficiency on the Brain
- Cerebral blood flow (CBF) decreases by more than 20%
- Cerebral glucose metabolism falls by approximately 12%
2. Respiratory Depression and CO₂ Narcosis
- Hypoventilation - slow, shallow respirations
- Hypercapnia (elevated PaCO₂) and mild hypoxia
- Blunted hypoxic and hypercapnic ventilatory drives
3. Hypothermia
- Thyroid hormones are essential for thermogenesis (they stimulate the Na⁺/K⁺-ATPase pump and mitochondrial uncoupling)
- Without T3/T4, basal metabolic rate drops dramatically
- Heat production falls, and the body cannot maintain core temperature
4. Hyponatremia (SIADH)
- Severe hyponatremia causes cerebral edema and impaired neuronal function
- Can progress to seizures, which can contribute to or deepen coma
5. Hypoglycemia
6. Hypotension and Shock
- Myxedema produces bradycardia, diastolic dysfunction, and reduced cardiac output
- Hypotension can be refractory to fluids and vasopressors until thyroid hormone is replaced
- Reduced cerebral perfusion pressure contributes to loss of consciousness
7. Precipitating Events (the "Trigger")
| Category | Examples |
|---|---|
| Infection | Pneumonia, UTI, sepsis |
| Cardiac | MI, congestive heart failure |
| CNS | Stroke, trauma |
| Drugs | Sedatives, narcotics, anesthetics (metabolism dramatically slowed) |
| Cold exposure | Winter, hypothermia |
| Discontinuing thyroid meds | - |
Summary: The Convergence Model
Thyroid hormone deficiency
↓
↓ Cerebral metabolism + ↓ CBF
+
Respiratory depression → ↑ CO₂ → acidosis
+
Hypothermia → impaired synaptic function
+
Hyponatremia (SIADH) → cerebral edema
+
Hypoglycemia
+
Hemodynamic compromise
+
Precipitating event
↓
COMA / STUPOR
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, pp. 397-398
- Rosen's Emergency Medicine, Box 117.7, Chapter 117
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 13
- Goldman-Cecil Medicine, Chapter on Thyroid Disorders
Create a clinical reference poster on myxedema coma diagnosis and scoring
A clinical reference poster titled "MYXEDEMA COMA: Diagnosis & Scoring" for medical professionals. Dark navy blue background with clean white and cyan text. Professional medical poster layout with multiple clearly labeled sections: TOP HEADER: Large bold title "MYXEDEMA COMA" with subtitle "Clinical Reference & Scoring Tool" in bright cyan. Small tag "Life-threatening Hypothyroid Emergency" SECTION 1 - "RECOGNITION" (left column, red-orange accent): Bullet list: • Older woman, winter season • Altered mental status → coma • Hypothermia (core temp <36°C; <32°C = poor prognosis) • Slow, shallow respirations + hypercapnia • Bradycardia, long QT • Refractory hypotension • Myxedema facies: puffy eyelids, macroglossia, broad nose • Hyponatremia, hypoglycemia SECTION 2 - "PRECIPITANTS" (left column, yellow accent): • Infection (pneumonia, UTI, sepsis) • Cardiac: MI, CHF • Cold exposure • Sedatives / narcotics / anesthesia • Stroke / trauma • Stopping thyroid medication SECTION 3 - CENTER: Large scoring table titled "MYXEDEMA COMA SCORING TOOL" with columns Criterion and Score: GCS 0-10 → 4 pts GCS 11-13 → 3 pts GCS 14 → 2 pts GCS 15 → 0 pts TSH >30 mU/L → 2 pts TSH 15-30 mU/L → 1 pt Low FT4 (<0.6 ng/dL) → 1 pt Hypothermia (<35°C) → 1 pt Bradycardia (<60 bpm) → 1 pt Precipitating event → 1 pt Below the table, score interpretation: Score 8-10: MYXEDEMA COMA — Treat NOW (red) Score 5-7: LIKELY — Treat if no other diagnosis (orange) Score <5: UNLIKELY (green) SECTION 4 - "LABS & DIAGNOSTICS" (right column, blue accent): • TSH (elevated in primary), T4 (low) • BMP: Na+, glucose, creatinine • ABG: CO2 retention, hypoxia • CBC: mild anemia • CK: elevated (muscle involvement) • ECG: bradycardia, long QT • Chest X-ray • Cortisol (rule out adrenal insufficiency) SECTION 5 - "TREATMENT" (right column, green accent): • IV Levothyroxine loading: 200-400 mcg IV • Then 1.6 mcg/kg/day IV • ± T3 (liothyronine) 5-10 mcg IV q8h (with caution) • Hydrocortisone 100 mg IV (before T4) • Passive rewarming only • Cautious IV fluids • Hypertonic saline if severe hyponatremia • ICU admission • Treat precipitating cause BOTTOM FOOTER: "Mortality: 25-60% • Early recognition and treatment is critical" in red. Small note: "Based on Rosen's Emergency Medicine & Plum and Posner's Coma" Overall: Polished, print-ready clinical poster with clear grid layout, icons for each section, color-coded severity bands on the scoring table.
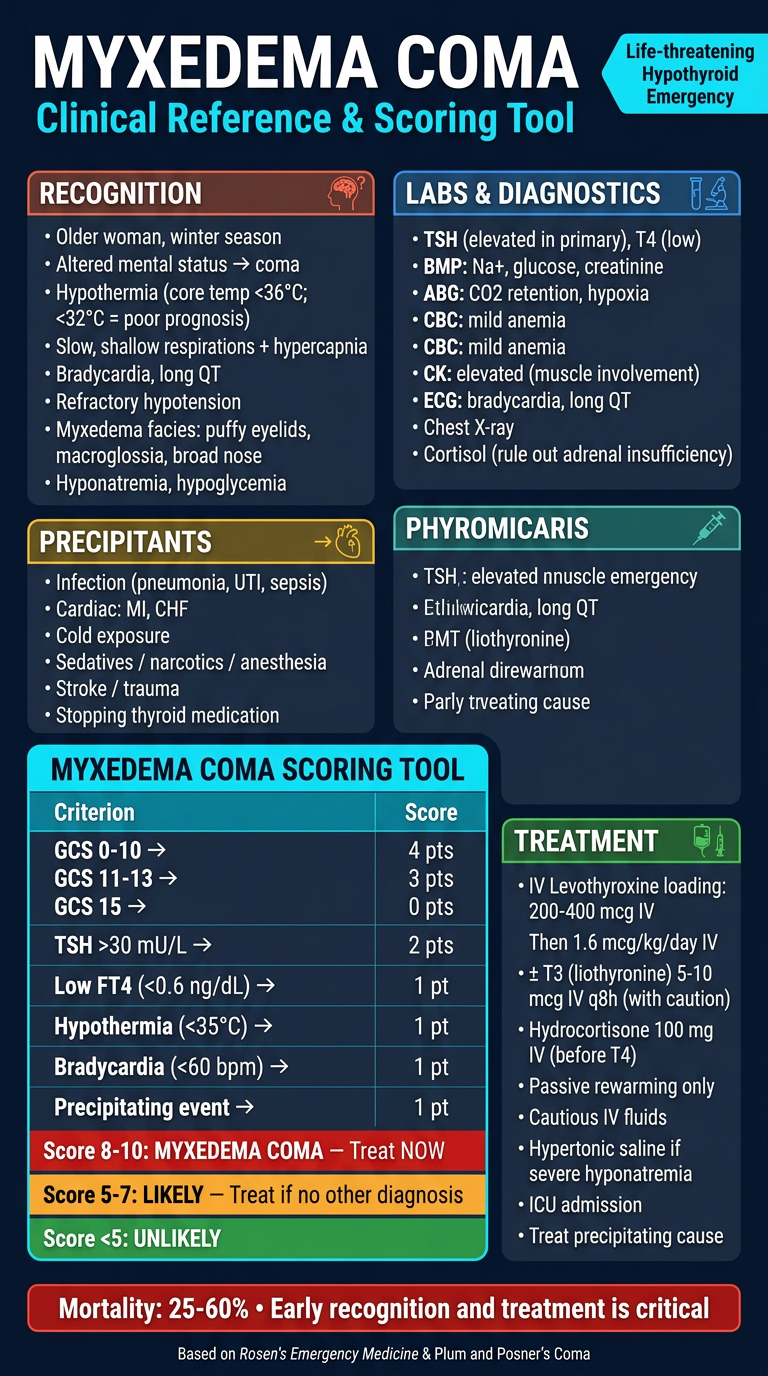
- Recognition criteria - the classic clinical features to look for
- Precipitating events - what triggers decompensation
- Myxedema Coma Scoring Tool - with the full GCS + lab + clinical scoring system and interpretation thresholds (Score ≥8 = treat immediately)
- Diagnostic workup - key labs, ECG, imaging
- Emergency treatment protocol - IV T4 loading, hydrocortisone, passive rewarming, and ICU management