Antiviral drugs
Reading File
Finding Sources
Searching the Web
antiviral drugs classification mechanisms 2025
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer:
Antiviral Drugs
Antiviral drugs are agents that inhibit viral replication by targeting virus-specific steps in the viral life cycle. Because viruses replicate inside host cells using the host's own machinery, these drugs must selectively target viral - not cellular - enzymes and processes. All antiviral drugs are virustatic (they inhibit replication but do not kill the virus), so immune responses remain essential for viral clearance, and reactivation can occur when treatment stops.
Key Principles
- Antiviral drugs target virus-specific events: entry, uncoating, nucleic acid synthesis, integration, protein synthesis/processing, or viral release.
- Resistance is more common with RNA viruses (higher mutation rate) than DNA viruses - resistant DNA virus variants are mainly a problem in immunocompromised patients.
- Combination therapy (targeting multiple steps simultaneously) reduces resistance selection and is the standard for HIV and HCV.
- Quantitative PCR is used to monitor treatment responses for viruses that circulate in blood (CMV, HBV, HCV, HIV).
(Harrison's Principles of Internal Medicine 22E, 2025 - Chapter 196)
Classification by Target Virus
1. Anti-Herpesvirus Drugs
Acyclovir, Valacyclovir, Famciclovir, Penciclovir
- Mechanism: Acyclovir (a deoxyguanosine analogue) is phosphorylated to its monophosphate form by viral thymidine kinase (in HSV/VZV-infected cells only). Cellular kinases complete phosphorylation to the active triphosphate, which inhibits viral DNA polymerase and is incorporated into viral DNA, terminating replication.
- Valacyclovir is a valine ester prodrug of acyclovir - better oral bioavailability, achieving plasma levels ~4x higher.
- Famciclovir/penciclovir work similarly but through a different nucleoside analogue pathway.
- Uses: HSV (genital herpes, herpes labialis, encephalitis, neonatal HSV), VZV (varicella, zoster). Higher doses needed for VZV (less susceptible). Poor activity against CMV.
- Resistance: Mutations in HSV thymidine kinase or DNA polymerase; managed with foscarnet or cidofovir.
Ganciclovir / Valganciclovir
- Mechanism: Phosphorylated in CMV-infected cells by the UL97 kinase (a viral phosphotransferase), then by cellular enzymes to the active triphosphate that inhibits viral DNA polymerase.
- Uses: CMV retinitis, CMV disease in transplant/immunocompromised patients; CMV prophylaxis post-transplant.
- Toxicity: Myelosuppression (neutropenia, thrombocytopenia) - major dose-limiting toxicity.
- Resistance: UL97 kinase mutations (most common) or DNA polymerase mutations.
Foscarnet
- Mechanism: Pyrophosphate analogue that directly inhibits viral DNA polymerase (HSV, CMV, VZV) and reverse transcriptase (HIV) without requiring phosphorylation.
- Uses: Acyclovir-resistant HSV/VZV, ganciclovir-resistant CMV, CMV retinitis.
- Toxicity: Nephrotoxicity (major), electrolyte abnormalities (hypocalcemia, hypomagnesemia, hypophosphatemia), genital ulceration.
Cidofovir
- Mechanism: Nucleotide analogue of deoxycytidine monophosphate; does not require viral enzymes for initial phosphorylation. Inhibits viral DNA polymerase.
- Uses: CMV retinitis (IV), acyclovir-resistant HSV, HPV-related lesions (topical).
- Toxicity: Severe nephrotoxicity (requires IV saline prehydration + probenecid).
(Harrison's Principles of Internal Medicine 22E, 2025)
2. Anti-Influenza Drugs
Neuraminidase Inhibitors: Oseltamivir, Zanamivir, Peramivir
- Mechanism: Inhibit viral neuraminidase, blocking cleavage of sialic acid required for release of new virions from infected cells and spread to other cells.
- Oseltamivir (oral prodrug, cleaved by liver esterases); Zanamivir (inhaled); Peramivir (IV).
- Uses: Treatment of influenza A and B (must start within 48 h of symptom onset - shortens duration by ~1 day); prophylaxis.
- Resistance: Neuraminidase or hemagglutinin mutations; ~15% in healthy children, ~1% adults; more common in immunocompromised patients.
- Oseltamivir is less active against influenza B than A.
Baloxavir Marboxil
- Mechanism: Inhibits influenza endonuclease (cap-dependent endonuclease), blocking viral mRNA transcription. Single-dose regimen.
- Uses: Acute uncomplicated influenza A and B.
M2 Ion Channel Inhibitors: Amantadine, Rimantadine
- Mechanism: Block the M2 ion channel (amantadine pocket) required for viral uncoating of influenza A.
- Active only against influenza A (not B).
- Now largely obsolete due to widespread resistance (>99% of circulating influenza A strains are resistant).
3. Antiretroviral Drugs (HIV)
Combination antiretroviral therapy (HAART) targeting multiple steps is standard care, suppressing viral load below detection and restoring immune function.
| Drug Class | Examples | Target |
|---|---|---|
| NRTIs (Nucleoside/Nucleotide Reverse Transcriptase Inhibitors) | Tenofovir, Abacavir, Emtricitabine, Lamivudine, Zidovudine | Viral reverse transcriptase (chain termination) |
| NNRTIs (Non-Nucleoside RTIs) | Efavirenz, Nevirapine, Rilpivirine, Etravirine | Reverse transcriptase (non-competitive, allosteric) |
| Protease Inhibitors (PIs) | Ritonavir, Darunavir, Atazanavir, Lopinavir | HIV protease (prevents maturation of virions) |
| Integrase Strand Transfer Inhibitors (INSTIs) | Dolutegravir, Raltegravir, Bictegravir, Cabotegravir | HIV integrase (blocks chromosomal integration) |
| Fusion Inhibitors | Enfuvirtide (T-20) | gp41 - blocks fusion of HIV envelope with cell membrane |
| CCR5 Antagonists (Entry Inhibitors) | Maraviroc | CCR5 coreceptor - blocks HIV entry into CD4+ cells |
(Jawetz, Melnick & Adelberg's Medical Microbiology 28E; Harrison's 22E)
Key points for HIV therapy:
- Monotherapy leads to rapid resistance selection; combination targeting multiple steps is mandatory.
- Drug-resistant variants can be transmitted; 8-10% of newly diagnosed patients in the US/Europe carry resistant virus.
- Tenofovir-based regimens also provide pre-exposure prophylaxis (PrEP).
- HAART has transformed HIV from a lethal to a chronic manageable disease, but must be continued lifelong.
4. Anti-Hepatitis Drugs
Hepatitis B (HBV)
Two classes are FDA-approved:
- Nucleos(t)ide Analogues - act as chain terminators of nascently replicating HBV DNA, competitively inhibiting HBV reverse transcriptase:
- Entecavir - first-line; very low resistance rate (~1-2% at 5 years in nucleoside-naive patients)
- Tenofovir disoproxil fumarate (TDF) / Tenofovir alafenamide (TAF) - first-line; no resistance detected after up to 10 years
- Lamivudine, Adefovir, Telbivudine - older agents with higher resistance rates
- Pegylated Interferons (PEG-IFN-α2a, α2b) - augment innate antiviral immune responses; SC injection for 48 weeks; significant side effects (flu-like syndrome, leukopenia, neuropsychiatric effects)
Hepatitis C (HCV) - Direct-Acting Antivirals (DAAs)
Modern HCV therapy achieves >95% sustained virological response (SVR = cure):
| Class | Examples | Target |
|---|---|---|
| NS3/4A Protease Inhibitors | Glecaprevir, Voxilaprevir, Grazoprevir | HCV serine protease (NS3/4A) |
| NS5A Inhibitors | Pibrentasvir, Elbasvir, Velpatasvir, Daclatasvir | NS5A replication complex protein |
| NS5B Polymerase Inhibitors | Sofosbuvir (nucleotide); Dasabuvir (non-nucleoside) | HCV RNA-dependent RNA polymerase |
Current standard regimens (8-12 weeks, pangenotypic):
- Sofosbuvir/velpatasvir (Epclusa) - pangenotypic
- Glecaprevir/pibrentasvir (Mavyret) - pangenotypic, 8 weeks in most patients
5. Anti-Respiratory Syncytial Virus (RSV) Drugs
- Palivizumab - monoclonal antibody against RSV F protein; used for prophylaxis in high-risk infants (premature, congenital heart disease, immunocompromised). Not therapeutic.
- Nirsevimab (Beyfortus) - newer long-acting monoclonal antibody for RSV prophylaxis in all infants.
- Ribavirin - nucleoside analogue with broad-spectrum activity; inhaled form used for severe RSV bronchiolitis in immunocompromised patients. Mechanisms include inhibiting viral RNA synthesis and viral mRNA capping.
6. Antivirals for Other Viruses
| Virus/Condition | Drug | Mechanism |
|---|---|---|
| HPV (genital warts) | Imiquimod (topical) | TLR-7 agonist - induces IFN-α and cytokines |
| HPV (anogenital warts) | IFN-α (intralesional) | Enhances cell resistance to virus |
| Mpox/Smallpox | Tecovirimat | Inhibits poxvirus replication (VP37 protein); blocks viral egress |
| CMV, Adenovirus, Poxvirus | Brincidofovir | Lipid conjugate of cidofovir; inhibits DNA polymerase; less nephrotoxic |
| COVID-19 | Nirmatrelvir/ritonavir (Paxlovid) | Inhibits SARS-CoV-2 main protease (Mpro) |
| COVID-19 | Remdesivir | Nucleoside analogue - RNA-dependent RNA polymerase inhibitor |
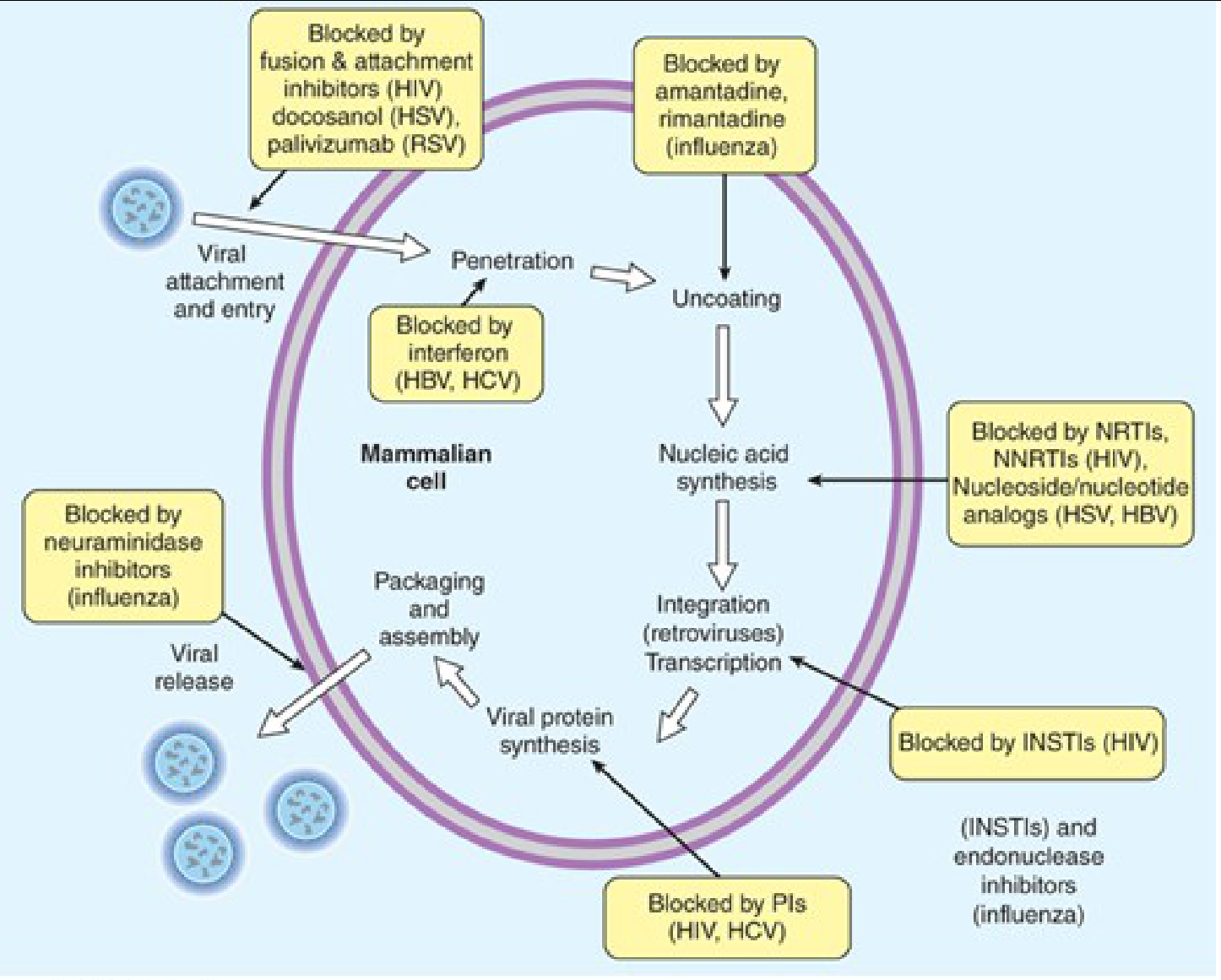
Mechanisms Summary by Stage of Viral Life Cycle
| Stage | Drug Examples |
|---|---|
| Attachment/Entry | Maraviroc (HIV), Enfuvirtide (HIV), Docosanol (HSV), Palivizumab (RSV) |
| Uncoating | Amantadine, Rimantadine (influenza A M2 inhibitors) |
| Nucleic Acid Synthesis | NRTIs/NNRTIs (HIV RT), Acyclovir/Ganciclovir (herpesvirus DNA pol), Sofosbuvir (HCV RdRp), Oseltamivir (influenza - viral release) |
| Integration | INSTIs - Dolutegravir, Raltegravir (HIV integrase) |
| Protein Processing | Protease inhibitors (HIV PIs, HCV NS3/4A inhibitors) |
| Viral Release | Neuraminidase inhibitors (Oseltamivir, Zanamivir); Tecovirimat (poxvirus) |
| Immune Modulation | Interferons (IFN-α/β), Imiquimod |
Drug Resistance
- Antiviral resistance arises from mutations in viral target proteins (e.g., thymidine kinase, DNA polymerase, reverse transcriptase, protease, neuraminidase).
- RNA viruses mutate faster than DNA viruses - resistant RNA virus variants can arise in healthy persons; resistant DNA virus variants are primarily a problem in immunocompromised patients.
- Cross-resistance within a drug class is common (e.g., PI-resistant HIV mutants are often resistant to multiple PIs).
- Strategies to limit resistance: combination therapy, adequate drug levels, adherence, resistance testing before therapy changes.
(Harrison's Principles of Internal Medicine 22E, 2025; Katzung's Basic and Clinical Pharmacology 16th Ed.; Jawetz, Melnick & Adelberg's Medical Microbiology 28E)
This is a shared conversation. Sign in to Orris to start your own chat.