Appendicular abscess in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from authoritative surgical textbooks. Let me compile a detailed, well-organized response.
Appendicular Abscess — A Detailed Overview
Definition and Pathogenesis
An appendicular abscess is a localized collection of pus in the right iliac fossa (and sometimes the pelvis or retroperitoneum), forming as a consequence of perforated acute appendicitis. It represents complicated appendicitis — a distinct pathophysiologic entity from uncomplicated appendicitis, not simply a progression of it.
When the appendix perforates, two outcomes are possible:
- Free perforation → diffuse peritonitis (if the contamination is not contained)
- Walled-off perforation → localized abscess (if the omentum, loops of small bowel, or retroperitoneal position seals off the leak)
The sequence is: acute inflammation → transmural necrosis → perforation → phlegmon formation → true abscess
"An abscess will develop after perforation if the perforated appendix is walled off from the remainder of the peritoneal cavity because of its retroperitoneal location or by loops of small intestine or omentum. A localized collection of inflammatory tissue (phlegmon) initially forms, and subsequently a true abscess develops." — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Epidemiology
- Overall perforation rate in appendicitis: 10–30% across most series
- Perforation rates are highest at the extremes of age:
- Children <2 years: up to 90%
- Patients >70 years: 50–70%
- Ages 10–30: lowest, around 10–20%
- Risk of perforation increases significantly after 24 hours of symptoms
- Patients with perforation typically have symptoms averaging 30 hours longer than those with simple appendicitis
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Clinical Features
Symptoms
- Right lower quadrant (RLQ) pain — often more prolonged than typical appendicitis (>24–48 hours)
- High-grade fever, rigors
- Nausea, vomiting, anorexia
- Diarrhea or constipation
Signs
- Significant fever and leukocytosis (more pronounced than uncomplicated appendicitis)
- Palpable RLQ mass — the hallmark; formed by the walled-off phlegmon/abscess
- Signs of local peritonism (guarding, tenderness) over the RLQ
- Rarely, if the abscess is pelvic: rectal tenderness, urinary frequency, diarrhea
"On physical examination, patients with an abscess resulting from appendicitis often have a palpable RLQ abdominal mass." — Sleisenger and Fordtran's
Imaging
CT Scan (Investigation of Choice)
- Most sensitive and specific modality
- Findings:
- Thickened, non-filling appendix ± appendicolith
- Periappendiceal fluid collection with enhancing wall = abscess
- Surrounding fat stranding
- Extraluminal gas (perforation)
- Free intraperitoneal air (if free perforation has occurred)
- Detects abscess, phlegmon, appendicolith, free fluid, free air — all features associated with complicated appendicitis
- Guides percutaneous drainage planning
Ultrasound
- Useful in children and pregnant women; identifies fluid collection and inflamed appendix
- Operator-dependent; lower sensitivity for retroperitoneal/pelvic collections
MRI
- Reserved for pregnant patients (no radiation); performed without contrast
- Sensitivity 97%, specificity 95% for appendicitis
- Can identify abscess formation
— Sabiston Textbook of Surgery
Distinction: Abscess vs. Phlegmon
| Feature | Phlegmon | Abscess |
|---|---|---|
| Nature | Inflammatory soft tissue mass (no fluid) | True loculated pus collection |
| CT appearance | Soft tissue/inflammatory density, no drainable fluid | Fluid collection with enhancing rim |
| Drainage | Not drainable | Drainable percutaneously |
| Initial management | IV antibiotics alone | Image-guided drainage + antibiotics |
Management
The management algorithm (below) is individualized based on presentation:
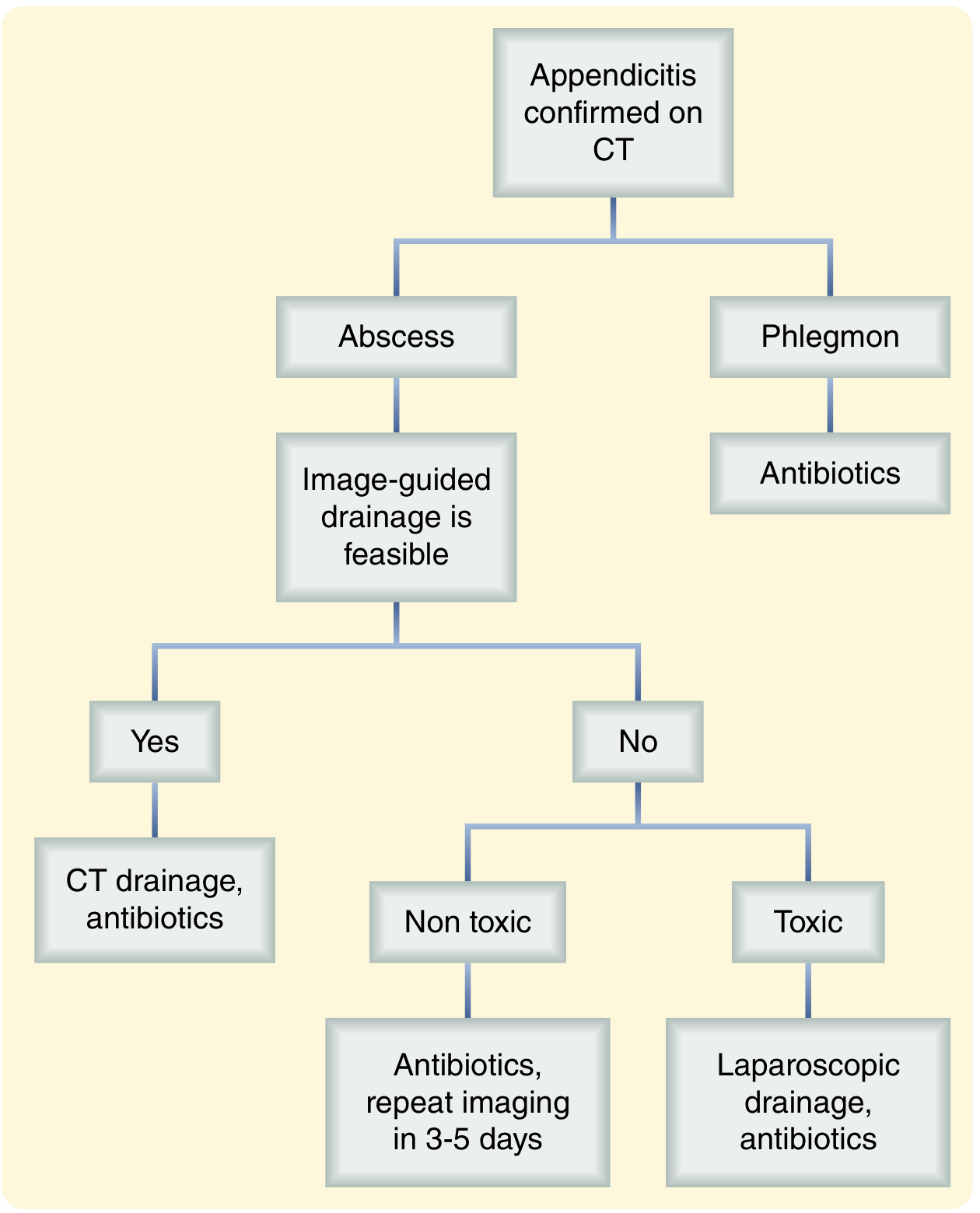
1. Resuscitation (All Patients)
- IV fluids, correction of electrolyte imbalances
- Broad-spectrum IV antibiotics (covering gram-negatives and anaerobes)
2. True Abscess — Image-Guided Percutaneous Drainage
- Preferred first-line approach for a drainable abscess
- CT-guided drainage is most successful; transgluteal drainage and lower-grade abscesses have better resolution rates
- Drain left in place until output ceases/slows to institutional standard
- Antibiotics continued for 4 days after source control
- Success rate: ~79% of patients achieve complete resolution
- If CT-guided drainage is not technically feasible: consider laparoscopic, transrectal, or transvaginal drainage
3. Phlegmon (No Drainable Collection)
- IV antibiotics alone for 4–7 days (per IDSA guidelines for intra-abdominal infection)
- If no improvement → re-imaging in 3–5 days to check for interval development of a drainable abscess
4. Immediate Surgery — Indications
- Diffuse peritonitis (free perforation)
- Septic/toxic patient not responding to conservative measures
- Failure of conservative management
"Immediate surgery is necessary in patients that appear septic, but this is usually associated with higher complications, including abscesses and enterocutaneous fistulae due to dense adhesions and inflammation." — Schwartz's Principles of Surgery
5. Operative Management (When Required)
- Laparoscopic appendectomy by experienced surgeons — supported by WSES Jerusalem Guidelines
- In severe inflammation: may require ileocecectomy (due to extreme induration/friability)
- Risks of immediate surgery in established abscess: failure to identify appendix, postoperative abscess, fistula, extension of resection
Antibiotic Regimens
For non-perforated (prophylaxis): Cefoxitin, ampicillin/sulbactam, cefazolin + metronidazole
For complicated/perforated appendicitis:
- Piperacillin/tazobactam (monotherapy)
- Cefepime or carbapenem + metronidazole
- β-lactam allergy: clindamycin + fluoroquinolone/gentamicin/aztreonam
— Schwartz's Principles of Surgery
Interval Appendectomy
After successful nonoperative treatment, the question of interval appendectomy (6–8 weeks later) is debated:
Arguments FOR:
- Recurrence rate of appendicitis after nonoperative management: 8–31.8%
- Risk of finding appendiceal neoplasm: benign 0.7%, malignant 1.3%
- Appendicolith on CT predicts higher recurrence → selective indication for interval appendectomy
Arguments AGAINST:
- 91% of patients have no further events at median 34-month follow-up
- Interval appendectomy is technically challenging (adhesions, inflammation) → higher complication rate
- WSES Jerusalem Guidelines: do NOT recommend routine interval appendectomy
Key update — Neoplasm risk:
The Peri-Appendicitis Acute (PERIA) randomized trial comparing interval appendectomy vs. MRI follow-up was stopped early due to a high rate of neoplasm in the interval appendectomy group (all in patients >40 years). Therefore:
"If no interval appendectomy is performed, colonoscopy and full-dose contrast-enhanced CT should be performed in all adult patients 40 and older as routine follow-up after nonoperative management of complicated appendicitis." — Sabiston Textbook of Surgery (citing WSES guidelines)
Complications of Appendicular Abscess / Perforated Appendicitis
| Complication | Details |
|---|---|
| Portal pylephlebitis | Septic thrombophlebitis of portal vein; presents with high fever + mild jaundice; treat with 4–6 weeks IV antibiotics; hepatic abscess in 50%, mortality 30–50% |
| Hepatic abscess | Secondary to pylephlebitis; common organisms: gram-negative aerobes + anaerobes |
| Enterocutaneous fistula | Risk with early operative intervention in inflamed tissues |
| Pelvic abscess | From pelvic positioning of appendix; may require transrectal/transvaginal drainage |
| Psoas abscess | Retroperitoneal extension |
| Portal vein thrombosis | Long-term sequela of pylephlebitis; leads to cavernous transformation and esophagogastric varices |
| Sepsis | Systemic inflammatory response from uncontrolled source |
Summary
| Feature | Detail |
|---|---|
| Cause | Perforated appendicitis, walled-off by omentum/bowel |
| Key sign | Palpable RLQ mass |
| Investigation of choice | CT abdomen-pelvis |
| First-line treatment | Percutaneous image-guided drainage + IV antibiotics |
| Phlegmon treatment | IV antibiotics ± re-imaging |
| Emergency surgery | Diffuse peritonitis, septic/toxic patient |
| Interval appendectomy | Selective (appendicolith present, age >40 neoplasm workup mandatory) |
| Follow-up (age ≥40) | Colonoscopy + CT after nonoperative management |
Sources: Sabiston Textbook of Surgery (20th ed.); Sleisenger and Fordtran's Gastrointestinal and Liver Disease (11th ed.); Schwartz's Principles of Surgery (11th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.