10 most common ecgs we see as a doctor in India and explain me that how to diagnose and step by step explanation
Reading File
Finding Sources
Finding Sources
Searching the Web
10 most common ECG patterns seen in India clinical practice diagnosis
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG normal sinus rhythm 12-lead
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
left ventricular hypertrophy LVH ECG voltage criteria
Finding Sources
Finding Sources
Searching Images
ventricular tachycardia wide complex tachycardia ECG
Searching Images
complete heart block third degree AV block ECG
Searching Images
right bundle branch block RBBB left bundle branch block LBBB ECG
Searching Images
sinus tachycardia bradycardia ECG
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
hyperkalemia peaked T waves ECG electrolyte
I now have comprehensive image and content resources for all 10 ECGs. Let me compile the complete, detailed answer.
🫀 10 Most Common ECGs in Clinical Practice (India) — Step-by-Step Diagnosis Guide
How to Read ANY ECG — The Universal 7-Step Approach
Before diagnosing any ECG, always follow this systematic method:
| Step | What to Check |
|---|---|
| 1 | Rate — Count R-R intervals. 300 ÷ large squares between R waves |
| 2 | Rhythm — Regular or irregular? Use calipers/pen |
| 3 | P waves — Present? Upright in II? One before every QRS? |
| 4 | PR interval — 0.12–0.20 sec (3–5 small squares) |
| 5 | QRS width — < 0.12 sec (3 small squares) = narrow (supraventricular) |
| 6 | ST segment & T wave — Elevation, depression, inversion? |
| 7 | Axis — Lead I & aVF: both +ve = normal axis |
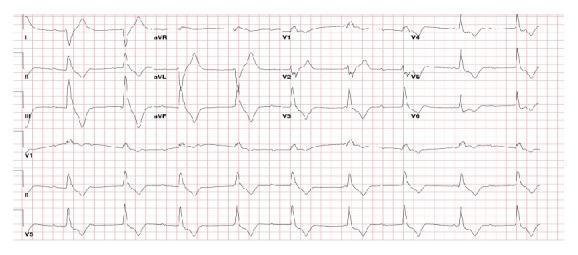
ECG 1: Normal Sinus Rhythm (NSR)
Why common in India: Baseline for all comparisons; seen in routine health checks, preoperative workups, outpatient clinics.
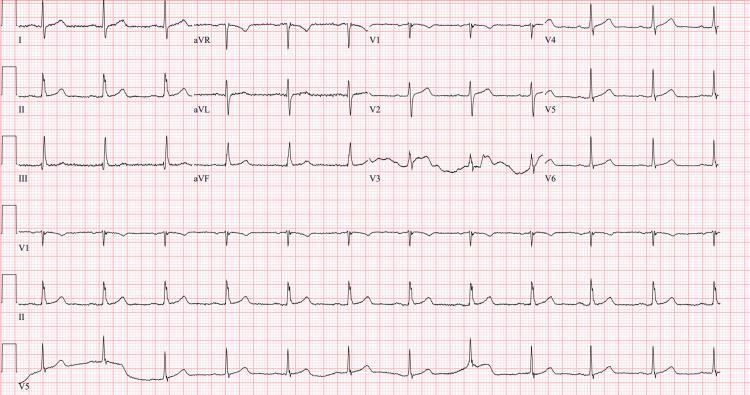
Step-by-step diagnosis:
- Rate: 60–100 bpm
- Rhythm: Regular (R-R intervals equal)
- P waves: Upright in leads I, II, aVF, V4–V6; inverted in aVR — confirms sinus origin
- PR interval: 0.12–0.20 sec (constant)
- QRS: Narrow < 0.12 sec
- ST segment: Isoelectric; T waves upright in I, II, V3–V6
- Axis: Normal (0° to +90°)
✅ Diagnosis: NSR when ALL 7 criteria met
ECG 2: STEMI — ST-Elevation Myocardial Infarction
Why common in India: India has a very high burden of CAD — younger age of onset (10–15 years earlier than Western populations), driven by diabetes, smoking, and genetic susceptibility.

Step-by-step diagnosis:
- Identify ST elevation: ≥ 1 mm in ≥ 2 contiguous limb leads, or ≥ 2 mm in ≥ 2 contiguous precordial leads
- Localise the territory:
| Territory | Leads with ST elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | V1–V2 (ST depression + tall R); do V7–V9 | RCA/LCx |
- Look for reciprocal ST depression — confirms true STEMI (e.g., inferior STEMI → ST depression in I, aVL)
- Hyperacute T waves: Earliest sign — tall, broad, symmetrical T waves
- Pathological Q waves: Develop in hours — necrosis marker; ≥ 0.04 sec wide and ≥ 25% of R wave height
- Assess for complications: LBBB, heart block (inferior STEMI can cause complete AV block via RCA)
⚠️ Key Indian context: Inferior + right ventricular MI is common (RCA dominant in Indians). Always do right-sided leads (V3R, V4R) in inferior STEMI — ST elevation ≥ 1 mm in V4R = RV infarct. Avoid nitrates in this case!
ECG 3: Atrial Fibrillation (AF)
Why common in India: Rheumatic heart disease (mitral stenosis), hypertension, and dilated cardiomyopathy are the dominant causes — all prevalent in India.
Step-by-step diagnosis:
- Rhythm: Irregularly irregular (hallmark) — no two R-R intervals are the same
- P waves: Absent — replaced by fine, chaotic fibrillatory (f) waves at 350–600 bpm; best seen in V1 and lead II
- QRS: Usually narrow unless aberrant conduction/BBB
- Rate: Ventricular response typically 100–160 bpm (uncontrolled); < 100 bpm if controlled or on rate-limiting drugs
- Look for: ST changes (ischaemia?), LVH (hypertensive cause?), large P mitrale in old traces (mitral stenosis)
Clues to cause:
- Rheumatic mitral stenosis → P mitrale in sinus rhythm, left atrial enlargement
- Hyperthyroidism (very common in India) → also causes AF; check for tachycardia, tremor history
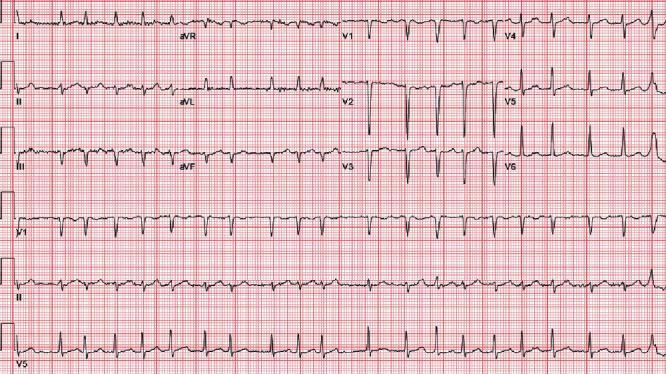
ECG 4: Left Ventricular Hypertrophy (LVH)
Why common in India: Hypertension affects ~28% of Indians; also CKD, aortic stenosis.
Step-by-step diagnosis:
Voltage criteria (pick one):
| Criterion | Formula | Positive if |
|---|---|---|
| Sokolow-Lyon | S in V1 + R in V5 or V6 | > 35 mm |
| Cornell | R in aVL + S in V3 | > 28 mm (men), > 20 mm (women) |
| aVL alone | R wave in aVL | > 11 mm |
Strain pattern (indicates LVH with pressure overload):
- ST depression + T-wave inversion in lateral leads (I, aVL, V5, V6)
- Asymmetric: downsloping ST with gradual upward T wave
Additional features:
- Left axis deviation
- Widened QRS (but < 120 ms)
- P mitrale (left atrial enlargement) — notched P in II, biphasic in V1
⚠️ Note: Sokolow-Lyon has lower sensitivity in obese Indian patients — Cornell voltage more reliable.
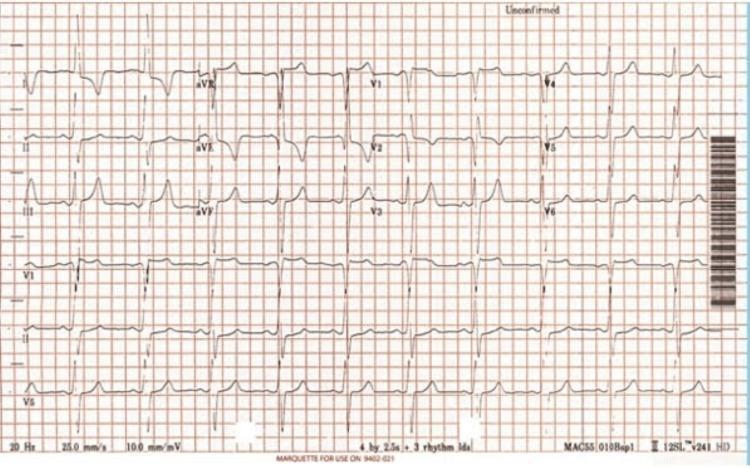
ECG 5: Left Bundle Branch Block (LBBB) / Right Bundle Branch Block (RBBB)
Why common in India: LBBB seen in dilated cardiomyopathy, hypertension, acute MI. RBBB common in PE, RV strain, congenital heart disease, and incidentally in older patients.
Step-by-step diagnosis:
Step 1 — Confirm BBB: QRS duration ≥ 120 ms (3 small squares)
Step 2 — Identify RBBB vs LBBB:
| Feature | RBBB | LBBB |
|---|---|---|
| V1 morphology | rSR' ("rabbit ears") | Broad, notched S (QS pattern) |
| V6 morphology | Wide S wave | Broad, notched R (no S wave) |
| Lead I | Wide S wave | Broad notched R |
| T wave | Discordant in V1–V2 | Discordant in V5–V6 |
LBBB Rule: In new LBBB with chest pain → treat as STEMI equivalent (Sgarbossa criteria apply)
Sgarbossa Criteria for MI in LBBB:
- ST elevation ≥ 1 mm concordant with QRS (highly specific) — 5 points
- ST depression ≥ 1 mm in V1–V3 — 3 points
- ST elevation ≥ 5 mm discordant with QRS — 2 points ≥ 3 points = significant for MI
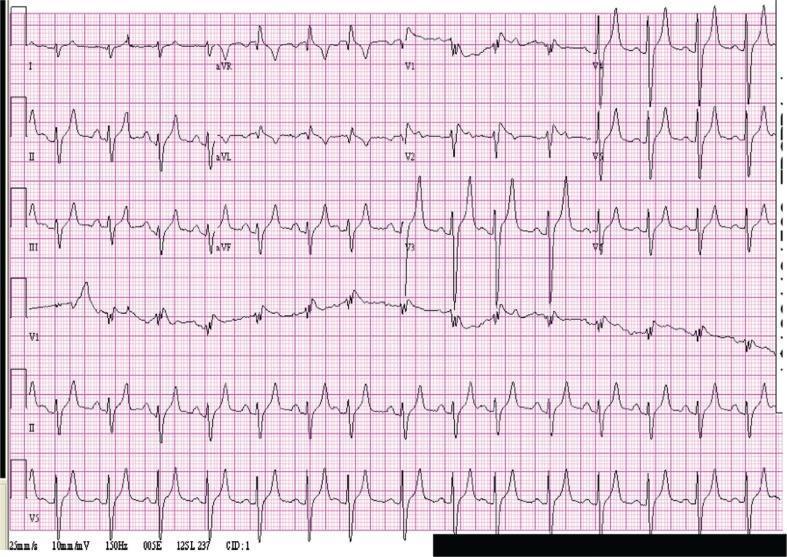
ECG 6: Ventricular Tachycardia (VT)
Why common in India: Seen in ischaemic cardiomyopathy (post-MI), dilated cardiomyopathy, electrolyte disturbances (common with CKD/diarrhoeal illness in India).

Step-by-step diagnosis:
- Wide complex tachycardia (WCT): Rate > 100, QRS ≥ 120 ms
- Rule VT vs SVT with aberrancy using Brugada algorithm:
| Question | If YES → |
|---|---|
| Is there RS complex absent in ALL precordial leads? | = VT |
| RS interval > 100 ms in any precordial lead? | = VT |
| AV dissociation present? | = VT |
| Classic LBBB or RBBB morphology criteria for VT? | = VT |
- Features strongly suggesting VT:
- AV dissociation (P waves marching independently — pathognomonic)
- Fusion beats (partially conducted sinus beat)
- Capture beats (normal narrow QRS amid wide complexes)
- QRS concordance in V1–V6 (all +ve or all –ve)
- Northwest axis (negative in I and aVF)
⚠️ Rule of thumb: In India, if you see WCT in a patient with known heart disease → treat as VT until proven otherwise.
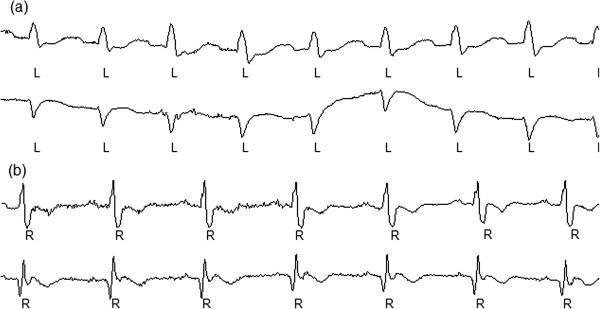
ECG 7: Complete Heart Block (Third-Degree AV Block)
Why common in India: Inferior STEMI (RCA occlusion), rheumatic heart disease, idiopathic fibrosis of conduction system (Lenegre/Lev's disease), digoxin toxicity.
Step-by-step diagnosis:
- Bradycardia — ventricular rate typically 30–45 bpm
- P waves present — regular P-P interval (atrial rate normal, 60–100 bpm)
- QRS present — regular R-R interval (but different from P-P rate)
- NO relationship between P and QRS — PR interval varies completely ("marching through" — P waves appear before, within, and after QRS)
- QRS morphology:
- Narrow (junctional escape) → block at AV node level
- Wide ≥ 120 ms (ventricular escape) → block below Bundle of His — more dangerous
Compare with other AV blocks:
| Degree | PR interval | Dropped beats? |
|---|---|---|
| 1st | > 0.20 sec, constant | None |
| 2nd Mobitz I (Wenckebach) | Progressive lengthening | Periodic drop |
| 2nd Mobitz II | Constant, then sudden drop | Yes |
| 3rd (Complete) | No relationship | AV dissociation |
⚠️ Inferior STEMI + complete heart block = usually transient (AV node ischaemia, responds to atropine). Anterior STEMI + complete heart block = distal block, often permanent — needs emergency pacing.
ECG 8: Sinus Tachycardia
Why common in India: Fever (extremely common — malaria, typhoid, dengue, TB), anaemia, hypovolaemia, sepsis, thyrotoxicosis, pain, anxiety.
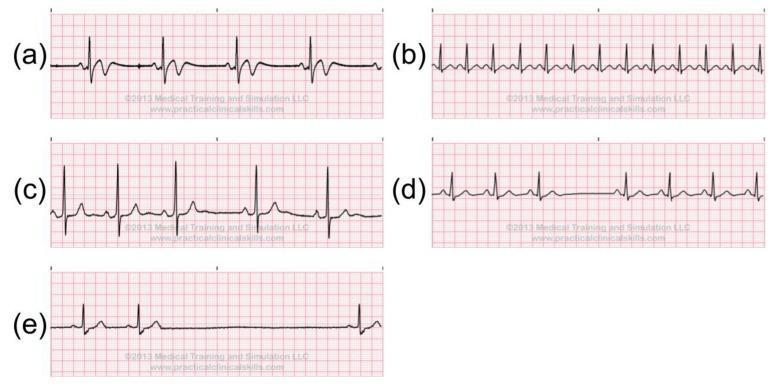
Step-by-step diagnosis:
- Rate: > 100 bpm (in sinus tachycardia)
- P wave: Upright in lead II, inverted in aVR — before every QRS
- PR interval: Normal (0.12–0.20 sec)
- QRS: Narrow, regular
- Gradual onset/offset (vs sudden onset of SVT/AF)
Sinus Tachycardia vs SVT:
| Feature | Sinus tachycardia | SVT/AVNRT |
|---|---|---|
| Rate | 100–150 bpm | 150–250 bpm |
| P wave | Visible, upright in II | Buried in/after QRS, retrograde |
| Onset | Gradual | Abrupt (paroxysmal) |
| Vagal | No termination | Often terminates |
Sinus Bradycardia (< 60 bpm): Common in athletes, inferior MI, hypothyroidism, drugs (beta-blockers, digoxin). Same P-wave criteria as NSR, just slower.
ECG 9: Pulmonary Embolism (PE) — Right Heart Strain Pattern
Why common in India: DVT from prolonged immobility, post-surgical states, malignancy, antiphospholipid syndrome; increasingly recognised in Indian hospitals.

Step-by-step diagnosis:
Classic but non-specific findings:
- Sinus tachycardia — most common ECG finding in PE (~44%)
- S1Q3T3 pattern:
- S1 — Deep S wave in lead I
- Q3 — Q wave in lead III
- T3 — Inverted T wave in lead III
- Right axis deviation (axis > +90°)
- Incomplete or complete RBBB — new, in the context of PE
- T-wave inversions in V1–V4 — right precordial T inversions = severe RV strain
- P pulmonale — tall peaked P in II (> 2.5 mm) = right atrial strain
⚠️ S1Q3T3 is only present in ~20% of PE cases — a normal ECG does NOT exclude PE. Most sensitive ECG finding = sinus tachycardia. Correlate with clinical Wells score, D-dimer, and CT-PA.
ECG 10: Hyperkalemia
Why common in India: CKD is epidemic (diabetic nephropathy, IgA nephropathy, FSGS); also dehydration, Addison's disease, ACE inhibitor overuse, rhabdomyolysis.
Step-by-step diagnosis — Progressive stages with K+ level:
| Potassium level | ECG change |
|---|---|
| 5.5–6.5 mEq/L | Tall, narrow-based, peaked ("tented") T waves — best seen in precordial leads V2–V5 |
| 6.5–7.0 mEq/L | P wave flattening/disappearance (sinoventricular rhythm) |
| 7.0–8.0 mEq/L | QRS widening — bizarre, slurred QRS |
| > 8.0 mEq/L | Sine wave pattern → ventricular fibrillation → asystole |
Key diagnostic features:
- Peaked T waves — tall, symmetrical, narrow base (unlike hyperacute T of STEMI which are broad)
- Flat/absent P waves
- Widened QRS
- Prolonged PR interval
- Sine wave = pre-terminal
⚠️ Emergency: Hyperkalemia + wide QRS → IV Calcium Gluconate 10 mL 10% over 2–3 min immediately (stabilises cardiac membrane).
Quick Reference Summary Table
| # | ECG | Rate | Rhythm | Key Feature | Indian Cause |
|---|---|---|---|---|---|
| 1 | Normal Sinus | 60–100 | Regular | P before every QRS | Baseline |
| 2 | STEMI | Variable | Usually regular | ST elevation in territory + reciprocal | CAD, young males |
| 3 | Atrial Fibrillation | Variable | Irregularly irregular | No P waves, f waves | Rheumatic MS, hypertension |
| 4 | LVH | Normal | Regular | Voltage criteria + strain | Hypertension, CKD |
| 5 | BBB | Normal | Regular | Wide QRS, rSR' (RBBB) or WiLLiaM/MaRRoW | DCM, PE, ischaemia |
| 6 | Ventricular Tachycardia | >100 | Regular | Wide complex, AV dissociation | Post-MI cardiomyopathy |
| 7 | Complete Heart Block | 30–45 | P & QRS independent | AV dissociation | Inferior MI, Lenegre's |
| 8 | Sinus Tachycardia | >100 | Regular | P upright in II, gradual onset | Fever, anaemia, sepsis |
| 9 | Pulmonary Embolism | >100 | Regular | S1Q3T3, T inv V1–V4, RBBB | DVT, post-surgical |
| 10 | Hyperkalemia | Variable | Variable | Peaked T → wide QRS → sine wave | CKD, DM nephropathy |
Memory Aid — "WiLLiaM MaRRoW" for BBB
- WiLLiaM = LBBB: W in V1, M in V6
- MaRRoW = RBBB: M in V1, W in V6
This guide covers the patterns you will encounter most frequently in Indian OPD, emergency, ICU, and ward settings. Master systematic reading first — then pattern recognition becomes reliable and fast.
This is a shared conversation. Sign in to Orris to start your own chat.