gas gangren detail for emergency medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gas gangrene" AND "Clostridium" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full emergency medicine-focused answer.
Gas Gangrene (Clostridial Myonecrosis) - Emergency Medicine Reference
This is a true surgical emergency. Do not delay operative debridement for imaging or other workup.
Definition & Overview
Gas gangrene (clostridial myonecrosis) is a rapidly progressive, life-threatening soft tissue infection characterized by muscle necrosis, gas production in tissues, and fulminant systemic toxemia. It is one of the most fulminant gram-positive bacterial infections known. Without treatment it is 100% fatal. Even with ICU care, antibiotics, and surgery, tissue destruction can continue to advance several inches per hour.
- Incidence (USA): ~1,000-3,000 cases/year
- Mortality: 5-30% for extremity infections with best care; >50% when bacteremia is present; approaches 100% for truncal/visceral infection
Microbiology
Primary pathogen: Clostridium perfringens (~90% of cases) - anaerobic, spore-forming, Gram-positive rod
Other causative species:
- C. septicum - associated with spontaneous (non-traumatic) gangrene; marker for occult GI malignancy
- C. novyi, C. histolyticum, C. sordellii, C. bifermentans, C. tertium, C. fallax
- Note: Nonclostridial organisms are found in ~85% of gas gangrene infections (mixed infections are common)
Key toxins of C. perfringens:
| Toxin | Effect |
|---|---|
| Alpha (α) | Phospholipase C - myonecrosis, hemolysis, platelet/PMN destruction, capillary damage - major lethal factor |
| Theta (θ) | Hemolysis, cardiotoxicity, depresses myocardial contractility |
| Kappa (κ) | Collagenase |
| Nu (ν) | DNase |
| Mu (μ) | Hyaluronidase |
Pathophysiology: Toxins cause rapid, irreversible ischemic muscle necrosis. Intravascular aggregates of platelets and neutrophils form, blocking leukocyte migration into infected tissue - explaining the characteristic absence of inflammatory cells on histology. Shock is driven by myocardial depression and reduced vascular resistance.
Two Clinical Types
1. Traumatic Gas Gangrene
Triggers: Contamination of devitalized tissue with spores
Risk factors:
- Crush injuries, lacerations of large/medium arteries
- Open fractures of long bones contaminated with soil or clothing
- Penetrating abdominal trauma with bowel perforation
- Post-surgical (bowel/biliary surgery - ~30% of cases)
- Hip surgery, leg amputation for vascular disease (proximity to fecal flora)
- Subcutaneous injection of black-tar heroin
Incubation: As short as 6 hours, usually <4 days (mean <24 hours)
2. Spontaneous (Non-traumatic) Gas Gangrene
- Caused primarily by C. septicum
- Arises from hematogenous seeding of normal muscle from a GI portal
- Associated with: colonic malignancy, inflammatory bowel disease, diverticulitis, necrotizing enterocolitis, neutropenic enterocolitis (post-chemotherapy for leukemia)
- Bacteremia precedes cutaneous manifestations by several hours
- Higher mortality than traumatic form
Clinical Presentation
Early Signs (first hours)
- Sudden, excruciating pain at the wound site - disproportionate to appearance (most reliable early symptom)
- Tachycardia (often out of proportion to fever)
- Anxiety, sense of doom
Progression
- Wound: thin, serosanguineous "dishwater" discharge with foul-sweet odor and gas bubbles
- Brawny edema and tense induration
- Skin: pale → bronze → purple/red → dark discoloration
- Hemorrhagic bullae containing bluish to maroon-colored fluid
- Crepitus on palpation (gas in tissue)
- Tissue sloughing; muscle that fails to bleed or contract when stimulated intraoperatively
Late/Systemic Signs
- Refractory hypotension (unresponsive to fluids)
- Intravascular hemolysis (~15% bacteremic)
- Renal failure
- Multiorgan failure
- Septic shock
- Death
Warning (Campbell's): When suppuration, gas in soft tissues, and toxemia are all present, the condition is usually fatal within 48 hours.
Diagnosis
Diagnosis is primarily clinical - do not delay surgery for confirmatory tests.
Bedside/Lab
- Gram stain of wound drainage or tissue biopsy - characteristic: abundant large Gram-positive (or Gram-variable) rods, near-complete absence of inflammatory cells, widespread soft tissue necrosis (see histopathology below)
- Blood cultures - if spontaneous gas gangrene suspected (bacteremia precedes skin findings)
- CBC: leukopenia is a poor prognostic sign; leukocytosis common; hemolysis on smear
- Metabolic panel: renal failure, metabolic acidosis
Histopathology of Gas Gangrene
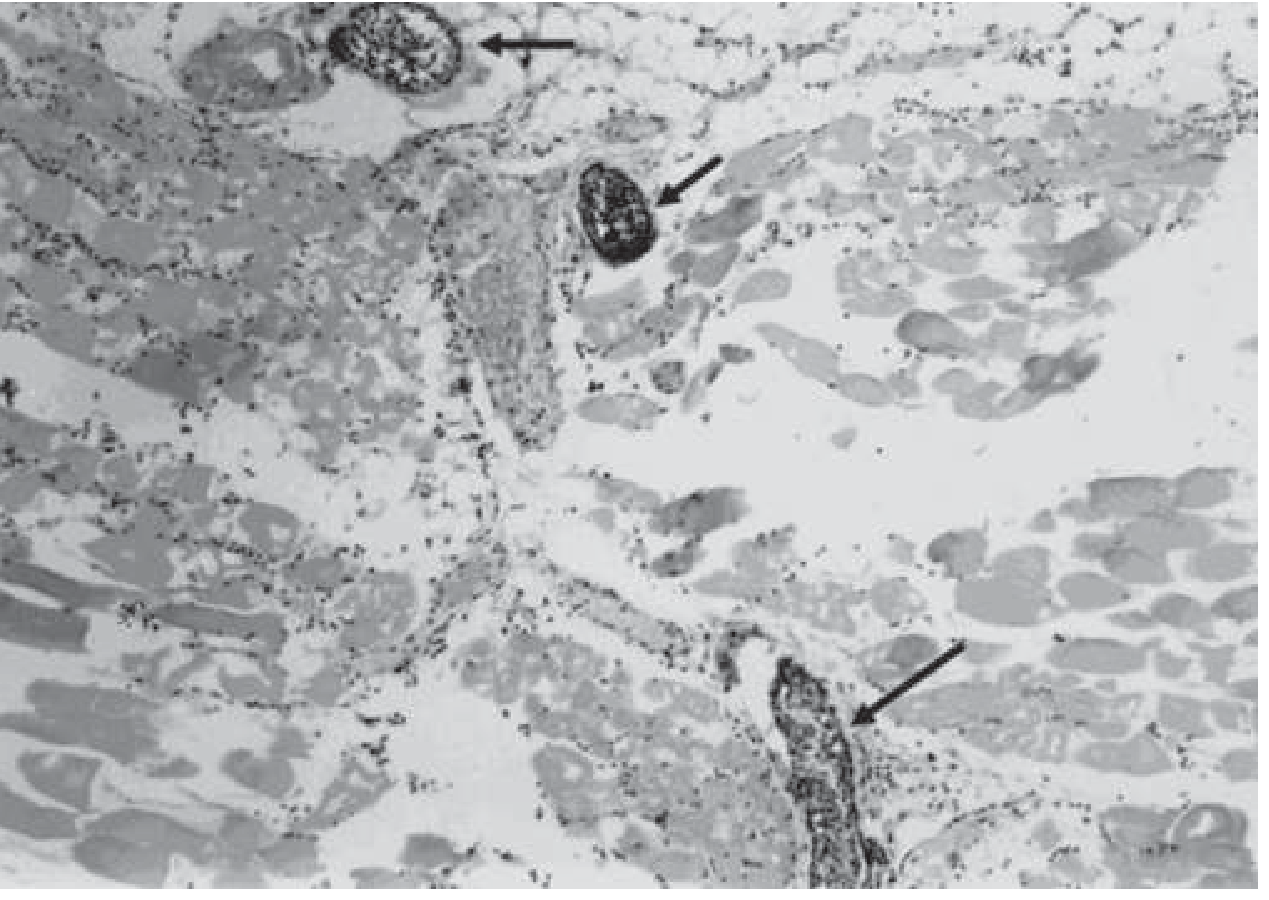
Widespread muscle necrosis with a paucity of leukocytes in infected tissue and accumulation of leukocytes in adjacent vessels (arrows) - due to alpha and theta toxin effects. - Harrison's 22E
Imaging (adjunct, do NOT delay surgery)
- Plain X-ray: gas in soft tissues - visible early, radiographic gas in fascial planes
- CT/MRI: determine extent, fascial plane spread, distinguish localized vs. spreading infection - but must never delay the OR
- Needle aspiration or punch biopsy: etiologic diagnosis in ~20% of cases
Radiographic appearance of gas gangrene:

Plain radiograph of left hand showing soft tissue gas in gas gangrene. - Campbell's Operative Orthopaedics 15E
Emergency Management: The Three Pillars
PILLAR 1 - IMMEDIATE SURGERY (Most Important)
This is the single best life-saving intervention.
- Emergent, wide surgical debridement - resect all devitalized tissue back to healthy, viable muscle and skin
- Muscle that does not bleed or contract is non-viable
- Repeat debridement every 24-48 hours based on wound condition
- Leave traumatic wounds and compound fracture wounds open for 5-6 days until confirmed infection-free
- Amputation when necessary to control spread and save life; radical amputation remains the definitive life-saving measure when extremity infection is advancing
- Fasciotomy if compartment syndrome co-exists
- All wounds with suspected clostridial infection (including amputation stumps) should be left open until infection is controlled
Never delay surgery for CT, MRI, or HBO transport. The margin of necrosis can advance inches per hour even on antibiotics.
PILLAR 2 - ANTIBIOTICS
| Scenario | Regimen |
|---|---|
| First-line (traumatic gas gangrene) | Penicillin G (high-dose IV) + Clindamycin for 10-14 days |
| Polymicrobial/mixed infection | β-lactam/β-lactamase inhibitor (e.g., piperacillin-tazobactam) or carbapenem + clindamycin |
| Penicillin-allergic | Clindamycin monotherapy (if susceptible) |
| C. tertium | Vancomycin 1 g IV q12h OR metronidazole 500 mg IV q8h |
| Open fractures (clean) | IV cephalosporin |
| Large dirt/grease-contaminated wounds | Cephalosporin + aminoglycoside |
| Crush/farm-contaminated wounds | Penicillin + cephalosporin + aminoglycoside |
Why clindamycin is added (despite penicillin being active):
- Inhibits bacterial protein/toxin production - reduces alpha-toxin synthesis
- Insensitive to bacterial inoculum size and growth phase
- Superior to penicillin alone in animal models
- Modulates host immune response
Resistance notes: C. perfringens is universally susceptible to penicillin; emerging clindamycin resistance (~3.8% of bloodstream isolates in Canadian data). Non-perfringens clostridia show ~14.2% penicillin resistance.
Alternative agents with activity: Metronidazole, tetracyclines, chloramphenicol
PILLAR 3 - SUPPORTIVE ICU CARE
- IV fluid resuscitation - but note refractory hypotension is common
- Vasopressors for septic shock
- Endotracheal intubation for severe cases with shock
- Monitor for hemolysis: serial CBC, LDH, haptoglobin, urinalysis (hemoglobinuria)
- Monitor renal function closely; prepare for dialysis
- Treat multiorgan failure aggressively
Hyperbaric Oxygen (HBO) - Adjunctive, Controversial
- Administered at 2-3 ATA, 3 times daily for acute infections
- Basic science: inhibits C. perfringens growth but NOT the more aerotolerant C. septicum
- Animal data: antibiotics alone are superior; HBO adds some benefit only if surgery and antibiotics precede it
- Never delay surgery or antibiotics for HBO
- May help stabilize limb amputations; some centers with co-located HBO units report benefit
- Decision: must weigh speed of treatment against time lost in transfer
Types of Clostridial Infection (Severity Spectrum)
| Type | Description |
|---|---|
| Type 1 | Clostridial contamination - positive culture without clinical signs |
| Type 2 | Clostridial cellulitis - foul gas-producing soft tissue infection, no systemic involvement |
| Type 3 | Gas gangrene proper - clostridial myonecrosis with systemic signs of severe infection |
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Necrotizing fasciitis (non-clostridial) | Mixed flora; fascia primarily affected; wooden-hard skin; gas less prominent |
| Anaerobic cellulitis | More gas than gas gangrene, but NO systemic toxicity and NO muscle involvement; pain and swelling less severe |
| Streptococcal myositis | PMNs present on Gram stain; pain very severe; less gas |
| Fournier's gangrene | Perineal/genital location; polymicrobial |
Prognosis
Favorable factors: Extremity involvement (vs. trunk/viscera), younger age, single limb, early aggressive debridement
Poor prognostic factors:
- Shock at time of diagnosis (40% mortality in shocked patients vs. 20% overall)
- Bacteremia (mortality >50%)
- Intravascular hemolysis
- Leukopenia
- Advanced age
- Spontaneous gas gangrene (especially C. septicum)
- Truncal or visceral involvement
Survivors commonly require multiple debridements and prolonged hospitalization and rehabilitation.
Prevention
- Prompt, thorough debridement of all traumatic wounds
- Removal of foreign bodies, dirt, necrotic tissue
- Drain hematomas
- Do not primarily close traumatic wounds or compound fractures
- Avoid prolonged tourniquet use
- Prophylactic antibiotics for contaminated open fractures
Emergency Summary Card
SUSPECT: Wound pain + gas in tissue + rapid systemic deterioration
CONFIRM: Gram stain (large GP rods, NO PMNs) + clinical picture
DO NOT DELAY SURGERY FOR IMAGING
1. SURGERY - emergent wide debridement ± amputation
2. ANTIBIOTICS - Penicillin G + Clindamycin IV
3. ICU - resuscitation, vasopressors, hemolysis monitoring
4. HBO - adjunct only, never delays above
Sources:
- Harrison's Principles of Internal Medicine, 22E (2025, McGraw Hill)
- Goldman-Cecil Medicine, International Edition (2022, Elsevier)
- Campbell's Operative Orthopaedics, 15E (2026)
- Clostridial Myonecrosis: A Comprehensive Review of Toxin Pathophysiology and Management Strategies - Hussain et al., 2024, Microorganisms [PMID: 39065232]
violance in emergency department detail for emergency medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"workplace violence" AND "emergency department"
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the key content. Let me compile the comprehensive answer.
Violence in the Emergency Department - Emergency Medicine Reference
(Source: Rosen's Emergency Medicine: Concepts and Clinical Practice, 9th Edition, Chapter 185)
Scope of the Problem
The ED is one of the highest-risk environments in all of healthcare for workplace violence. Key statistics:
- The assault-injury rate in healthcare occupations is nearly 10 times that of the general sector
- Over half of all healthcare providers will be victims of some form of violence during their careers
- Emergency care providers are more likely than any other healthcare group to experience violent events - verbal threats, physical assaults, or confrontations outside the workplace
- In a 2018 ACEP poll of 3,539 emergency physicians:
- Nearly 50% reported being assaulted while at work in the ED
- Over 70% had witnessed an assault in the workplace
- 97% of assaults were committed by the patient; in 28% of cases, family or friends acted as accessories
- Men and women face comparable risk of violence
- Violent incidents are far more likely to be verbal threats or acts of intimidation than physical assaults
- Consequences extend beyond physical injury: provider PTSD, lost productivity, and burnout
Why the ED is a High-Risk Environment
- Open 24 hours a day, 7 days a week
- High stress, illness, and prolonged waiting times
- Availability of potential hostages
- Accessibility to drugs or weapons
- Perceived gaps in communication
- Patients often brought in against their will
- Patients may be agitated, intoxicated, or mentally ill
Conditions Associated With Violence (Box 185.1)
Psychiatric Causes
| Condition | Notes |
|---|---|
| Schizophrenia | Delusions of persecution; auditory command hallucinations |
| Paranoid ideation | May act preemptively against perceived threat |
| Catatonic excitement | Unpredictable |
| Mania | Emotional lability - pleasantness can turn to aggression rapidly |
| Personality disorders (borderline, antisocial) | Maladaptive behavior patterns |
| Delusional depression | |
| PTSD | Triggered by trauma cues |
| Decompensating OCD |
Organic (Medical) Causes - ALWAYS consider these
| Condition | Examples |
|---|---|
| Neurological | CVA, CNS infection (meningitis/encephalitis), neoplasm, seizure, vascular malformation, dementia |
| Metabolic | Hypoglycemia, hypoxia, electrolyte abnormalities, hypothermia/hyperthermia, anemia |
| Endocrine | Thyroid storm, Addisonian crisis |
| Infectious | HIV/AIDS-related encephalopathy |
| Drugs/intoxicants | Alcohol intoxication AND withdrawal, stimulants (cocaine, methamphetamine), PCP, hallucinogens |
| Medications | Unanticipated reactions, especially in injured or elderly patients |
| Vitamin deficiency/toxicity | e.g., hypervitaminosis D |
| Situational | Fear of illness, fear of dependence/rejection, miscommunication, mutual hostility |
Neurobiology: The serotonin system largely controls aggression and inhibition. Diminished serotonergic function disinhibits aggression. Generalized brain dysfunction from any cause can impair impulse control.
Distinguishing Organic From Functional Causes
| Clinical Feature | Delirium (Organic) | Dementia (Organic) | Functional (Psychiatric) |
|---|---|---|---|
| Onset | Acute | Gradual | Gradual |
| Age at onset | Any | >50 years | <40 years |
| Alertness | Altered | Normal | Normal or hyperalert |
| Orientation | Impaired | May be impaired | Normal |
| Hallucinations | Common; visual, auditory, tactile | None | Auditory (schizophrenia); otherwise uncommon |
| Symptom picture | Fluctuating | Stable | Stable |
| Abnormal vital signs | Common | Uncommon | Uncommon |
| Prior psychiatric history | No | No | Yes |
Key rule: Patients aged 40+ with new-onset psychiatric symptoms are more likely to have an organic cause. Always rule out organic causes first.
Violence Risk Assessment
Warning Signs of Impending Violence (Box 185.3)
- Angry demeanor
- Loud, aggressive speech
- Tense posturing (gripping arm rails tightly, clenching fists)
- Pacing or frequently changing body position
- Aggressive acts (pounding walls, throwing objects, hitting oneself)
- Mounting agitation or resistance to authority
Risk Escalation Pattern
Anger → Resistance to authority → Confrontation → Violence
Clinicians should trust their "gut feeling" - if a dangerous situation seems to be developing, take precautions. However, violence can erupt without warning (especially organic brain syndrome), so avoid overconfidence.
Patient Factors That Increase Risk
- History of prior violent behavior (strongest predictor of serious injury)
- Known psychiatric illness (especially schizophrenia, mania)
- Substance abuse or drug-seeking behavior
- Intoxication (alcohol, stimulants, PCP)
- Prolonged waiting time in the ED
ED Preparedness and Prevention (Box 185.2 - Three Tiers)
General Physical/System Factors
- Prominently displayed warning signs prohibiting weapons; alert all entering that they may be screened
- Nondiscriminatory policy for weapon inquiries and searches, with clear policies for contraband disposal
- Panic/alarm system to activate hospital security or police
- Dedicated phone with direct line to police or security
- Controlled ED access - limit to 1-2 entrances; consider buzzer access systems; bulletproof glass or metal bar barriers at front desks
- Secure examination room: solid ceiling, shatterproof lights, heavy indestructible chairs, secured restraint bed, two outward-swinging doors lockable from outside, emergency distress button, video monitoring
Primary Prevention - Reduce Frustration/Aggression
- Minimize waiting times to the extent feasible
- Optimize waiting room environment (comfort, communication)
- Visible surveillance cameras
- Trained, visible security force reflecting local community violence prevalence
Secondary Prevention - Pre-violent Agitation
- Recognition of risk (pre-violent patients AND companions)
- Implementation of de-escalation techniques
- Minimize treatment delays for pre-violent individuals
- Ongoing staff training in violence management
Tertiary Prevention - Once Violence Occurs
- Use of physical and chemical restraints
- Appropriate security and police intervention
- Apply familiar predetermined protocols
The Interview Environment - Safety Setup
Before interviewing any potentially dangerous patient:
- Station security strategically; leave the door open
- Patient and interviewer seated roughly equidistant from the door, OR interviewer between patient and door
- Do NOT block the door (traps both parties)
- Examination room doors should swing outward; more than one exit is ideal
- Clinician maintains unrestricted access to the door
- Remove heavy or throwable objects from the room
- Establish a code word/phrase to summon security (e.g., "I need 'Dr. Armstrong' in here")
- Remove from yourself: earrings, necklaces, neckties, stethoscope, scissors
- Be aware of objects on the patient (pens, watches, cell phones, belts, key chains) that could be weaponized
Management: Step-by-Step Approach
Step 1: Verbal De-Escalation (First-Line)
Try verbal techniques BEFORE physical or chemical restraint whenever the patient is cooperative enough to engage.
Ten Elements for Verbal De-Escalation (AAEP Project BETA Consensus):
| # | Element | Practical Tip |
|---|---|---|
| 1 | Respect personal space | Maintain ≥2 arm's lengths; provide easy exit for both parties |
| 2 | Avoid provocation | Hands relaxed, non-confrontational posture, avoid staring |
| 3 | Establish verbal contact | The first person to successfully connect should lead |
| 4 | Use concise, simple language | Impaired people cannot process complex or technical terms |
| 5 | Identify feelings and desires | "What are you hoping for?" |
| 6 | Listen closely | Restate what patient said: "Tell me if I have this right..." |
| 7 | Agree or agree to disagree | "Yes, everyone should be treated with respect." |
| 8 | Set clear limits | "Violence or abuse cannot be tolerated here." |
| 9 | Offer choices and optimism | Patients feel empowered if given some choice |
| 10 | Debrief patient and staff | Include opportunity for both to speak afterward |
Additional verbal tips:
- Calm, soothing tone of voice
- Acknowledge the obvious: "You look angry" - opens emotional sharing
- If agitation escalates: "You seem to want to do the right thing. How can we come up with a solution together?"
- Address violence directly: ask about suicidal/homicidal ideation, weapon possession, history of violence, current intoxicants
- Offer medication or restraints respectfully before further escalation
Counterproductive approaches to avoid:
- Arguing, threats, deception, or condescension
- Open threat to call security (invites aggression)
- Transference of clinician's own anger
- Deliberate deception (false promises - will be discovered, endangering the next provider)
- Denial or downplaying of threatening behavior
To prevent escalation: Remove the patient from contact with other agitated companions. Expedite triage and evaluation - increased waiting times correlate directly with violent behavior.
Step 2: Physical Restraints
Indicated when verbal techniques fail, or when the patient is immediately violent.
Indications:
- Imminent harm to patient, others, or the environment
- Part of an effective ongoing behavioral treatment program
Patient categories:
- Organic disorder - restraints facilitate evaluation
- Functional psychosis - verbal techniques less effective; restraints allow neuroleptic administration
- Personality/other disorders - verbal techniques ineffective
Contraindications to seclusion:
- Unstable patients requiring close monitoring
- Suicidal patients (unless continuous observation is possible)
- Self-abusive or self-mutilating patients
- Patient who has ingested drugs or poisons
Restraint Application Protocol:
- Follow a predetermined ED protocol - ideally activated when the examiner leaves the room after failed verbal de-escalation
- Treating clinician should avoid active participation in restraint application to preserve the therapeutic relationship
- Restraint team: minimum 5 people (one leader + four limb holders)
- Leader (physician, nurse, or security officer) experienced in restraints
- Leader briefs the team beforehand: outlines protocol, identifies dangerous objects in room
- All team members remove personal objects that could be weaponized against them
- Use a mixed-gender team to mitigate potential allegations
- Team engages as a group with a professional, non-threatening attitude - many patients calm down upon seeing the team
- Once secured, chemical sedation should be administered promptly to allow restraint removal as soon as possible
- Document specific indications for restraint (e.g., "Patient stated he would beat me and then took a swing at me" - not just "patient was violent")
- Restrained patients require ongoing monitoring: respiratory status, circulation at restraint sites, vital signs
Step 3: Chemical Sedation (Pharmacological Restraint)
Drug Selection by Clinical Scenario
The Severely Violent Patient:
- Droperidol 2.5-5 mg IM/IV, titrate as needed
- OR Midazolam 2.5-5 mg IM/IV, titrate as needed
- OR Midazolam 2.5-5 mg + Droperidol 2.5-5 mg IM/IV
- OR Haloperidol 2.5-5 mg + Lorazepam 1-2 mg IM/IV
- OR Ketamine 1-2 mg/kg IV / 4-5 mg/kg IM
Undifferentiated Severely Agitated Patient or Stimulant Intoxication:
- Lorazepam 1-2 mg IM/IV
- OR Midazolam 2.5-5 mg IM/IV
- OR Haloperidol 5 mg IM/IV + Lorazepam 2 mg IM/IV
CNS Depressant Intoxication (e.g., Alcohol):
- Haloperidol 2.5-5 mg IM/IV
- OR Droperidol 2.5-5 mg IM/IV
- OR Ketamine 1-2 mg/kg IV/IM
Known Psychotic/Psychiatric Disorder:
- Haloperidol 2.5-5 mg IM/IV
- OR Droperidol 2.5-5 mg IM/IV
- OR Haloperidol 2.5-5 mg + Lorazepam 2 mg IM/IV
- OR Ziprasidone 10-20 mg IM
- OR Olanzapine 5-10 mg IM
Cooperative but Agitated Patient:
- Lorazepam 1-2 mg PO
Key Drug Notes
Haloperidol (first-generation antipsychotic):
- Reliable, widely available, effective for psychosis-driven agitation
- Risk: QTc prolongation; extrapyramidal side effects
- Safe in alcohol intoxication (no respiratory depression)
Droperidol:
- Faster onset than haloperidol; effective and well-studied
- QTc concern historically; avoid in known QT prolongation
Lorazepam/Midazolam (benzodiazepines):
- First choice for stimulant intoxication, alcohol withdrawal, undifferentiated agitation
- Respiratory depression risk - monitor closely
- Midazolam: faster onset IM (peak ~5 min IM) vs. lorazepam
Ketamine:
- Dissociative anesthetic; rapid onset (1-2 min IV, ~4 min IM); ~20 min duration
- Good safety profile; useful after benzodiazepine/antipsychotic failure
- Dose: 1-2 mg/kg IV or 4-5 mg/kg IM
- Faster IM onset than other agents but requires repeat dosing or combination therapy
- Avoid in: elderly with acute agitated delirium, increased cardiovascular risk, schizophrenia
- Side effects: hypertension/tachycardia (usually transient), drooling, laryngospasm (rare), emesis, emergence reactions
- Prehospital ketamine associated with higher intubation rates vs. in-ED use
Rosen's recommendation for undifferentiated severely agitated patient:
Benzodiazepine (lorazepam) alone OR with first-generation antipsychotic (haloperidol)
Step 4: Armed/Weapons Situation
- If a weapon is displayed, do not approach
- Immediately clear the area of all other patients and staff
- Do not attempt to disarm the patient
- Attempt verbal resolution and de-escalation while awaiting security
- If a weapon is put down, do not reach for it - continue verbal resolution while awaiting security
- Request a hostage negotiator from legal authorities if needed
- Activate the department panic/alarm system
Post-Restraint Medical Evaluation
Once the patient is controlled, always screen for organic causes of agitation:
- Complete history (prior psychiatric history, medications, substance use)
- Vital signs: fever, hypertension, tachycardia, hypoxia point to organic cause
- Blood glucose (immediately)
- Targeted labs: BMP, CBC, toxicology screen, blood alcohol level, TSH, ABG if respiratory compromise
- Physical exam under sedation: head trauma, focal neurological signs, meningismus
- CT head if new-onset aggression, age >40, trauma, focal neurological findings
- ECG if antipsychotics used (QTc monitoring)
Never assume psychiatric cause without ruling out organic etiology, even in patients with known psychiatric disease.
Factors Contributing to Difficult Patient Encounters
ED Factors
- Lack of patient choice of facility or physician
- Time constraints, frequent interruptions
- Suboptimal privacy (hallway examinations)
- Long waiting times, department crowding
- Negative bias from other team members (triage, nursing, prehospital)
Clinician Factors
- Poor communication skills
- Difficulty expressing empathy; becoming easily frustrated
- Personal negative bias/prejudices
- Limited knowledge of patient's condition or psychosocial situation
- Overly rigid medical agenda
- Burnout, sleep deprivation, shift fatigue
Patient Factors
- Behavioral issues (argumentative, manipulative, non-compliant)
- Fear of abandonment
- Psychiatric conditions
- Low literacy
- Maladaptive behavior patterns that escalate in response to clinician reaction
Difficult patient encounters affect 15-30% of physician-patient encounters and are a major contributor to clinician dissatisfaction and burnout.
Consequences of ED Violence and Staff Wellbeing
- Physical injury to staff
- Provider PTSD symptoms
- Compassion fatigue
- Loss of work productivity
- Professional burnout (especially with high frequency difficult encounters)
- Compromised patient care for the violent patient and other ED patients
- Post-incident debriefing is an element of the formal de-escalation protocol
Summary Card for Practice
ASSESSMENT
- Identify organic vs. functional cause
- Recognize warning signs early (posturing, pacing, loud speech)
- History of violence = strongest predictor of serious injury
ENVIRONMENT
- Position yourself near exit; remove personal jewelry/accessories
- Code word to summon security unobtrusively
STEP 1: VERBAL DE-ESCALATION
- Calm tone, simple language, non-confrontational posture
- Offer choices; set limits; listen and restate
- Expedite triage to reduce waiting-time frustration
STEP 2: PHYSICAL RESTRAINT (if verbal fails)
- 5-person team; clinician avoids direct participation
- Document specific indications
- Follow immediately with chemical sedation
STEP 3: CHEMICAL SEDATION
- Undifferentiated/stimulant: Lorazepam ± Haloperidol
- Alcohol intoxication: Haloperidol or Droperidol
- Psychiatric: Haloperidol ± Lorazepam
- Refractory: Ketamine 1-2 mg/kg IV / 4-5 mg/kg IM
STEP 4: POST-RESTRAINT
- Rule out organic causes: glucose, vitals, neuro exam, labs
- Remove restraints as soon as chemical sedation is adequate
- Debrief staff
Source: Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 185 - The Combative Patient and Violence in the ED
Recent evidence supplement:
- Xie et al. (2025, J Adv Nurs) - Systematic review confirming ED crowding as a major contributing factor to patient-initiated violence against nurses [PMID: 39846503]
- Hou et al. (2024, J Adv Nurs) - Integrative review of violence against nurses by patients and visitors in the ED [PMID: 37658637]
- Fricke et al. (2023, Trauma Violence Abuse) - Scoping review of healthcare workplace violence guidelines and systematic reviews [PMID: 36341578]
toxic epidermal necrolysis for emergency medicine
Finding Sources
Finding Sources
Searching PubMed
"toxic epidermal necrolysis" AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative emergency medicine and dermatology textbooks. Let me compile the full answer.
Toxic Epidermal Necrolysis (TEN) - Emergency Medicine Reference
Overview and Classification
TEN and Stevens-Johnson syndrome (SJS) exist on a continuous spectrum of the same disease - a severe cutaneous adverse reaction (SCAR) representing an immune-mediated hypersensitivity reaction with keratinocyte apoptosis and epidermal detachment.
| Condition | BSA Epidermal Detachment | Mortality |
|---|---|---|
| SJS | <10% | ~5% |
| SJS/TEN overlap | 10-30% | ~10-15% |
| TEN | >30% | Up to 30% |
- TEN incidence: 0.4-1.2 per million person-years
- SJS incidence: 1.2-6.0 per million person-years
- Affects all age groups; no sex predilection
- HIV infection increases risk by an equivalent magnitude for both SJS and TEN
Etiology and Causative Agents
Medications are the most common cause (~50-70% of cases). The highest-risk period is the first 2 months of treatment.
High-Risk Drugs (most common triggers)
| Drug Class | Specific Agents | Risk Notes |
|---|---|---|
| Sulfonamides | TMP-SMX (1-3:100,000), sulfadoxine-pyrimethamine (10:100,000) | Most common antibiotic cause |
| Anticonvulsants | Carbamazepine (14:100,000), lamotrigine (1:1000), phenytoin, barbiturates, phenobarbital | Major cause; HLA-linked |
| Allopurinol | - | Currently most common cause in Europe |
| NSAIDs | Oxicam derivatives (highest risk), diclofenac (moderate), ibuprofen (no increased risk) | Oxicams especially dangerous |
| Antibiotics | Penicillins, cephalosporins, quinolones, tetracyclines, aminopenicillins | Lower individual risk but commonly used |
| Antiretrovirals | Nevirapine | High risk |
| Others | Aspirin, acetaminophen (especially in children) |
Other Causes
- Malignancy (lymphoma most common)
- HIV infection
- Idiopathic: 30-50% of cases
Genetic Risk Factors (HLA-linked)
- HLA-B*15:02 - carbamazepine-induced SJS/TEN in Han Chinese and other Asian populations (~10% prevalence) - HLA typing mandatory before starting carbamazepine in Asians
- HLA-B*58:01 - allopurinol-induced SJS/TEN
- Carbamazepine causes up to one third of TEN cases in Taiwan vs. only 5% in Europe
Pathophysiology
Keratinocyte death occurs through multiple mechanisms:
-
Immune-mediated pathway: Drug-tissue complex activates cytotoxic CD8+ T cells and NK cells → release of granulysin (key mediator), TNF-α, TRAIL, and perforin-granzyme B → widespread keratinocyte necrosis
-
Fas/FasL pathway: Elevated soluble Fas ligand (sFasL) in blood binds Fas (CD95/death receptor) on keratinocytes → apoptosis. sFasL levels correlate with BSA involvement
-
Effector memory CD8+ T cells, regulatory T cells, NK cells, and Th17 cells all play roles
-
The characteristic absence of inflammatory infiltrate in necrotic areas is due to toxin-mediated inhibition of leukocyte migration
-
Serum granulysin levels may correlate with disease severity - emerging as a biomarker
Clinical Presentation
Prodrome (1-2 weeks before skin signs)
- Fever, malaise, anorexia, arthralgias
- Sore throat, rhinitis, myalgias
- Upper respiratory tract infection symptoms
- Skin tenderness, pruritus, tingling, or burning may precede rash
Skin Phase - Sequence of Events
1. Initial: Warm erythema beginning on face, trunk, eyes, nose, mouth, and genitalia - then becoming generalized within hours
2. Target lesions: Deep-red/dusky macules, sometimes 2-zone or targetoid lesions (atypical targets, not true 3-zone targets), purpuric centers that coalesce
3. Bullae formation: Flaccid, ill-defined bullae appear within areas of erythema along the cleavage plane between epidermis and dermis
4. Epidermal detachment: Epidermis shed in large sheets - raw, denuded areas of exposed dermis
5. Nikolsky sign POSITIVE: Lateral pressure with a finger on apparently normal skin adjacent to a bulla dislodges the epidermis - hallmark sign
- Skin is exquisitely painful to touch (distinguishes from staphylococcal scalded skin syndrome where it is tender but less dramatic)
- Time from drug exposure to onset: typically 2 weeks (range 4-28 days)
- Cutaneous extension: unpredictable; can range from 24 hours to 15 days - some severe cases: extensive involvement within 24 hours
Clinical appearance of TEN:

Toxic epidermal necrolysis showing extensive epidermal detachment with denuded dermis - Rosen's Emergency Medicine
Mucosal Involvement (occurs in virtually all cases of SJS, common in TEN)
Examine all mucosal surfaces:
| Site | Manifestations |
|---|---|
| Oral | Perilabial blistering, erosive lesions, hemorrhagic crusting - impairs oral intake |
| Ocular | Purulent conjunctivitis, painful erosions, pseudomembrane formation - can cause permanent blindness |
| Anogenital | Erosions, dysuria, vaginal/rectal involvement |
| Respiratory tract | Cough, bronchitis, sloughing of airway/respiratory epithelium - can cause ARDS |
| GI tract | Diarrhea, GI erosions |
| Urinary tract | Hematuria, urethritis |
Symptoms guiding mucosal involvement: photophobia (ocular), dysphagia (oral/esophageal), dysuria (urethral/vaginal), cough (respiratory)
Complications
The two leading causes of death are:
- Sepsis/infection - Staphylococcus and Pseudomonas predominate; loss of skin barrier = open wound
- Hypovolemia and electrolyte disorders - massive insensible losses through denuded skin
Other serious complications:
- ARDS from respiratory mucosal involvement (mortality 70% when present)
- Acute renal failure
- Bacteremia
- Ocular scarring and vision loss (most common long-term sequela)
- Corneal scarring, permanent blindness
- Sicca syndrome (dry eyes - even without acute ocular involvement)
- Cutaneous scarring, nail abnormalities, hair loss, sweating abnormalities
- Eruptive melanocytic lesions
Prognostic Scoring - SCORTEN
The SCORTEN (Severity-of-Illness Score for Toxic Epidermal Necrolysis) - calculate on admission and at day 3:
| Prognostic Factor | Points |
|---|---|
| Age > 40 years | 1 |
| Heart rate > 120 beats/min | 1 |
| Cancer or hematologic malignancy | 1 |
| BSA involved > 10% | 1 |
| Serum urea > 10 mM (28 mg/dL) | 1 |
| Serum bicarbonate < 20 mM | 1 |
| Serum glucose > 14 mM (252 mg/dL) | 1 |
| SCORTEN | Predicted Mortality |
|---|---|
| 0-1 | 3.2% |
| 2 | 12.1% |
| 3 | 35.8% |
| 4 | 58.3% |
| ≥5 | 90% |
Note: Respiratory tract involvement (not included in SCORTEN) is also a major independent poor prognostic factor - associated with 70% mortality when ARDS develops.
Diagnosis
Clinical Diagnosis
- Diagnosis is primarily clinical based on morphology, distribution, and Nikolsky sign
- Always seek the offending drug - review medication history carefully, timing (4-28 days before onset)
Investigations (not for diagnosis but for management/prognosis)
- CBC: Leukopenia (poor prognosis), eosinophilia (suggests DRESS overlap)
- BMP: BUN/urea, bicarbonate, glucose (SCORTEN components), electrolytes
- LFTs: Hepatitis may indicate DRESS/DIHS overlap
- Blood cultures: If infection suspected
- Urinalysis: Hematuria, proteinuria
- Chest X-ray: ARDS, pneumonia
Skin Biopsy (confirm in atypical cases)
- Frozen section on blister roof or sloughed skin - fastest
- Histology: Lymphocytic infiltrate at dermoepidermal junction (DEJ), full-thickness keratinocyte necrosis, cellular necrosis out of proportion to the infiltrate
- Direct immunofluorescence (DIF) to exclude paraneoplastic pemphigus and bullous pemphigoid
- TEN and SJS are histologically indistinguishable from each other
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Staphylococcal scalded skin syndrome (SSSS) | Child <5, cleavage subcorneal (not full epidermis); mucous membranes spared; responds to anti-staphylococcal antibiotics |
| Pemphigus vulgaris | Autoimmune; positive DIF; oral involvement common; older adults |
| Bullous pemphigoid | Tense bullae; less mucous membrane involvement; older adults; DIF positive |
| Erythema multiforme major | True 3-zone target lesions; acral distribution; usually HSV-triggered; <10% BSA; mucositis usually 1 site |
| DRESS syndrome | Prominent eosinophilia, lymphadenopathy, visceral involvement; skin less severe |
| Kawasaki disease | Children; fever >5 days; no epidermal detachment; no blisters |
| Graft-vs-host disease | Transplant patient; identical histology; follicular involvement may favor GVHD |
Emergency Management
IMMEDIATE PRIORITIES
1. STOP THE OFFENDING DRUG IMMEDIATELY
- The single most important intervention
- Review all medications - identify and stop the causative agent
- Use the ALDEN score to establish drug causality if multiple medications
- Do NOT rechallenge (dangerous)
2. AIRWAY ASSESSMENT
- Assess for respiratory mucosal sloughing - can cause acute airway obstruction
- Early intubation threshold should be low if respiratory involvement is suspected
- Sloughing of airway epithelium can occur rapidly
- Do not delay - ARDS from respiratory involvement carries 70% mortality
3. IV ACCESS AND RESUSCITATION
- Place IV lines at uninvolved skin sites
- Fluid resuscitation: approximately two-thirds of Parkland formula for equivalent burn BSA (metabolic demands are less than true burns)
- Parkland formula: 4 mL/kg/% BSA burned (24 hrs, half in first 8 hrs) - apply at 2/3 rate for TEN
- Correct hypovolemia and electrolyte abnormalities
- Monitor urine output closely
4. BURN UNIT / ICU ADMISSION
- TEN requires immediate transfer to a burn unit (preferred) or ICU
- Consult burn center before applying any topical dressings
- Multidisciplinary team: dermatology, ophthalmology, intensivist, ID
Skin Wound Care
| Principle | Specifics |
|---|---|
| Minimize trauma | Avoid tape-to-skin contact |
| IV line placement | Uninvolved skin only |
| Keep skin moist | Promotes healing |
| Dressings | Non-stick dressings; silver-impregnated dressings acceptable |
| Involved epidermis | Leave in place as a natural biologic dressing - do NOT debride |
| Eroded mucosal surfaces | Separate with non-stick dressings to prevent adhesion and scarring |
| Skin substitutes | May be explored for large denuded areas |
Specialist Consultations (Mandatory)
| Specialist | Reason |
|---|---|
| Ophthalmology (urgent) | Ocular involvement - prevent permanent blindness; may use amniotic membranes |
| Dermatology | Wound care, immunomodulatory therapy guidance, biopsy |
| Burns team | Fluid management, wound care protocols |
| Gynecology/Urology | Severe vaginal/urethral involvement - prevent adhesions |
| Nutrition/Dietetics | Nutritional support - hypercatabolic state |
| Infectious disease | Antibiotic guidance, infection surveillance |
Ocular Management (Wills Eye Manual)
Assess at every encounter - ocular sequelae are the most common long-term complication:
- Ocular surface inflammation: Topical steroid drops (prednisolone acetate 1% or difluprednate 0.05%) 4-8x/day
- Tear deficiency: Preservative-free artificial tears, gels, ointments aggressively; topical cyclosporine 0.05-2%; punctal occlusion; moisture chambers; tarsorrhaphy
- Iritis: Topical steroids + cycloplegia (atropine 1% BID)
- Infections: Treat as bacterial keratitis
- Conjunctival/eyelid margin defects: Daily pseudomembrane removal
- Severe cases: Amniotic membrane transplantation (early placement)
Infection Management
- Prophylactic systemic antibiotics NOT recommended
- Monitor closely for signs of sepsis - major cause of death
- Obtain cultures (blood, wound) with any signs of infection
- Prompt, aggressive antibiotic treatment for suspected or documented infection
- Staphylococcal and Pseudomonal species predominate
- Avoid agents known to cause TEN when treating
Immunomodulatory Therapy
No definitive consensus exists - significant controversy remains. Options include:
| Agent | Dose | Notes |
|---|---|---|
| Cyclosporine | 3-6 mg/kg/day divided | Preferred in many European centers; inhibits T-cell activation; emerging evidence supports use |
| IVIG | 1 g/kg/day x 4 days | Used in USA; mechanism: blocks sFasL-Fas interaction; evidence mixed |
| Etanercept | Variable | Randomized study from Asia showed benefit; TNF-α blocker |
| Corticosteroids | High-dose short course | Controversial - may help early in disease course; avoid later (increases infection risk) |
| Plasmapheresis | - | In consultation with specialist; considered in refractory cases |
Emergency physician's role: Stop the drug, stabilize, admit. Immunomodulatory decisions are made by dermatology/ID specialists.
Nutritional Support
- Patients are in a hypercatabolic state
- Early enteral nutrition preferred
- Oral intake often severely impaired by oral mucosal erosions
- Nasogastric feeding may be required
After the Acute Phase - Sequelae
- Average time for epidermal regrowth: 3 weeks
- Most common long-term complication: Ocular scarring and vision loss
- Severity of acute ocular involvement is the only predictor of eventual visual complications
- Sicca syndrome (dry eyes) - can develop even without clinical ocular involvement during acute episode
- Cutaneous scarring, hyperpigmentation/hypopigmentation
- Nail dystrophy, hair abnormalities, altered sweating
- Altered taste
- Eruptive melanocytic nevi
- Vaginal/urethral adhesions and stenosis
Emergency Summary Card
TEN = SJS/TEN spectrum with >30% BSA epidermal detachment
Mortality up to 30% (SCORTEN ≥5 = 90%)
IMMEDIATE (ED):
1. STOP THE DRUG - most important intervention
2. Assess AIRWAY - low threshold to intubate (mucosal sloughing)
3. IV access at UNINVOLVED sites - fluid resuscitation (2/3 Parkland)
4. Calculate SCORTEN - prognostication
5. Consult OPHTHALMOLOGY - prevent blindness
6. Transfer to BURN UNIT/ICU
WOUND CARE:
- Leave epidermis in place (natural biologic dressing)
- Non-stick dressings only
- No tape-to-skin
- Keep moist
ANTIBIOTICS:
- NO prophylaxis
- Treat documented/suspected infection aggressively
- Staph + Pseudomonas predominate
IMMUNOTHERAPY (specialist-directed):
- Cyclosporine 3-6 mg/kg/day (Europe)
- IVIG 1g/kg/day x4 days (USA)
- Etanercept (emerging evidence)
- Corticosteroids - controversial
SCORTEN:
Age >40 + HR >120 + Malignancy + BSA >10% +
BUN >28 + Bicarb <20 + Glucose >252
Score 0-1=3.2% | 2=12.1% | 3=35.8% | 4=58.3% | ≥5=90%
Sources:
- Rosen's Emergency Medicine, 9th Edition, Chapter 107
- Tintinalli's Emergency Medicine, Chapter 249
- Andrews' Diseases of the Skin, Chapter 6
- Fitzpatrick's Dermatology, Table 44-2 (SCORTEN)
- Wills Eye Manual - Ocular SJS/TEN Management
Recent evidence: Shah et al. (2024), Am J Clin Dermatol - Update on SJS/TEN diagnosis and management [PMID: 39278968] | Hung et al. (2024), Nat Rev Dis Primers - Severe cutaneous adverse reactions comprehensive review [PMID: 38664435]
This is a shared conversation. Sign in to Orris to start your own chat.