Phylloed tumor in details
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced information from multiple authoritative surgical and pathology textbooks. Here is a detailed overview of phyllodes tumor:
Phyllodes Tumor
Definition & Overview
Phyllodes tumor is a fibroepithelial neoplasm of the breast arising from the intralobular stroma. The name comes from the Greek phyllodes ("leaf-like"), describing the characteristic gross and histologic appearance of leaf-like projections. It was historically called cystosarcoma phyllodes, a misnomer now largely abandoned because the majority of cases follow a benign course.
It accounts for <1–2.5% of all fibroepithelial breast lesions and is therefore uncommon.
Pathogenesis & Molecular Biology
Like fibroadenomas, the majority of phyllodes tumors carry mutations in:
- MED12 (part of the transcriptional regulator mediator complex)
- RARA (retinoic acid receptor alpha)
This shared mutational profile suggests a shared pathogenesis with fibroadenoma. However, phyllodes tumors are more likely to harbor additional driver mutations that distinguish them:
- TERT (telomerase gene) — associated with malignant transformation
- TP53 — tumor suppressor loss
- RB — cell cycle regulator loss
A key molecular distinction: stromal cells of fibroadenomas may be polyclonal or monoclonal, whereas those of phyllodes tumors are always monoclonal, confirming their neoplastic nature.
— Robbins, Cotran & Kumar Pathologic Basis of Disease
Gross Pathology
- Tumors vary from a few centimeters to massive lesions that may occupy the entire breast
- The cut surface shows bulbous, leaf-like protrusions — nodules of proliferating stroma covered by epithelium extending into cystic spaces
- Connective tissue composes the bulk of the tumor, with mixed gelatinous, solid, and cystic areas
- Cystic areas represent sites of infarction and necrosis
- The tumor is usually sharply demarcated from surrounding compressed breast tissue
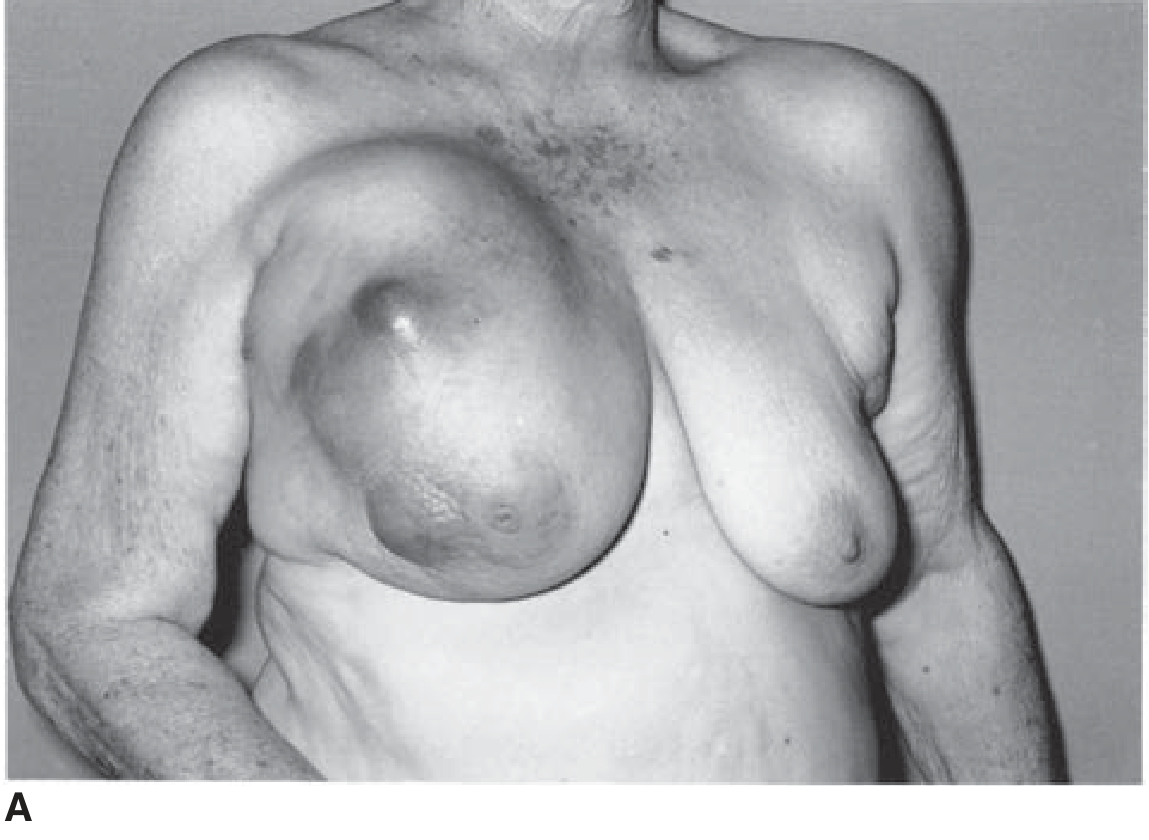
Clinical photo — Malignant phyllodes tumor (cystosarcoma phyllodes):
Histopathology
The defining histologic feature is a biphasic proliferation of stroma and mammary epithelium, with elongated epithelium-lined clefts creating the leaf-like architecture.
Histologic grading is based entirely on stromal features:
| Grade | Features |
|---|---|
| Benign | Cellular stroma, mildly increased mitotic activity; resembles fibroadenoma but more cellular |
| Borderline | More prominent stromal atypia, increased cellularity, and mitotic activity |
| Malignant | Widely infiltrative, marked stromal overgrowth with few residual epithelial elements; may be indistinguishable from pure sarcoma |
Malignant phyllodes tumors often contain liposarcomatous or rhabdomyosarcomatous elements rather than fibrosarcomatous elements. The number of mitoses and presence of invasive foci at the tumor margin help identify malignancy.
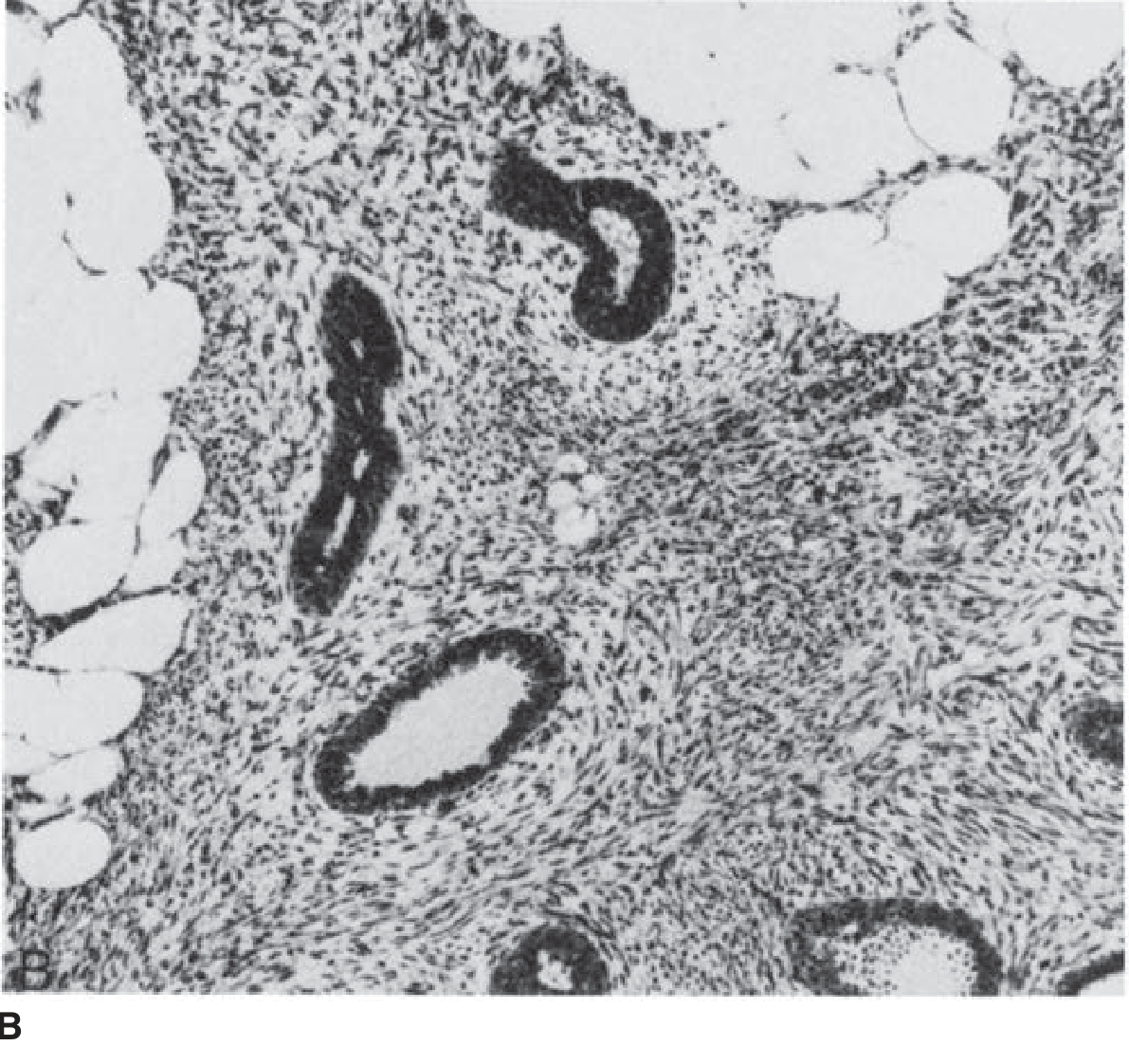
Histology — Malignant phyllodes tumor (H&E ×100):
— Schwartz's Principles of Surgery, 11th Ed.
Clinical Features
| Feature | Details |
|---|---|
| Age | Peak in the 5th–6th decade (10–20 years later than fibroadenoma) |
| Sex | Almost exclusively females |
| Presentation | Firm, lobulated, palpable mass; average size ~5 cm |
| Growth | Can be slow or rapidly growing |
| Suspicious features vs. fibroadenoma | Size >3 cm, rapid growth, older patient |
Up to 75% are benign cytologically.
Diagnosis
- Mammography: May show calcifications; cannot reliably distinguish benign from malignant, or from fibroadenoma
- Core needle biopsy (CNB): Preferred over fine-needle cytology; however, classifying grade on limited sampling is difficult — a CNB reported as "cellular fibroepithelial lesion" could represent either fibroadenoma or phyllodes tumor
- Excisional biopsy: Gold standard for definitive diagnosis and grading when CNB is equivocal
— Sabiston Textbook of Surgery; Berek & Novak's Gynecology
Behavior & Prognosis
| Grade | Local Recurrence | Metastasis | Notes |
|---|---|---|---|
| Benign | Occasional | None | Margin status is the key predictor of recurrence |
| Borderline | Increased risk | Rare | Greater potential than benign |
| Malignant | High | ~1/3 of cases (hematogenous) | Metastases contain only stromal component |
- Lymph node spread is rare regardless of grade
- Metastases occur via hematogenous spread, most commonly to the lungs
- Most recurrences occur within the first 2 years after excision
— Robbins, Cotran & Kumar; Sabiston Textbook of Surgery
Management
Surgery (Cornerstone)
| Grade | Surgery |
|---|---|
| Benign | Local/excisional biopsy with clear margins — curative (similar to fibroadenoma) |
| Borderline / Malignant | Wide local excision with ≥1–2 cm margins to reduce local recurrence |
| Large tumors | Total mastectomy may be required when tumor size is disproportionate to breast size |
- Axillary lymph node dissection is contraindicated — lymphatic spread is exceedingly rare and axillary staging is not indicated
Adjuvant Therapy
- Radiation: May be considered for borderline or malignant phyllodes undergoing breast-conserving surgery
- Chemotherapy: For metastatic malignant phyllodes — treated as sarcoma (limited benefit); common regimens follow sarcoma protocols
Follow-Up
- Close surveillance with physical examination and imaging, especially in the first 2 years post-excision
— Sabiston Textbook of Surgery; Schwartz's Principles of Surgery; Mulholland & Greenfield's Surgery
Phyllodes vs. Fibroadenoma — Key Distinctions
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age | 20s–30s | 40s–60s |
| Size | Usually <3 cm | Often >3 cm |
| Growth | Slow | Can be rapid |
| Stroma | Less cellular, polyclonal or monoclonal | Always monoclonal, more cellular |
| TERT/TP53/RB mutations | Absent | Present in malignant forms |
| Behavior | Benign, no excision required | Excision always required |
| Axillary spread | None | Rare but possible (malignant) |
Sources:
- Robbins, Cotran & Kumar — Pathologic Basis of Disease
- Schwartz's Principles of Surgery, 11th Ed.
- Sabiston Textbook of Surgery
- Mulholland & Greenfield's Surgery, 7th Ed.
- Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.