my patient is having pain on back of the thigh in piriformis region while external rotation of hip and also in adductor region the pain radiates down in the leg No numbness is there The pain initially is dull aching but its intensity increases if he remains in hip’s external rotation I have noticed slight piriformis tightning and more tfl tightning Give me detailed analysis and what can be possible diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Searching PubMed
piriformis syndrome diagnosis treatment
I now have comprehensive material to give a thorough clinical analysis. Let me compile the full answer.
Detailed Clinical Analysis
Patient's Presentation Summary
- Pain: posterior thigh (piriformis region) + adductor region
- Radiation: down the leg (sciatic distribution)
- Character: dull aching, worsens with sustained external rotation of hip
- No numbness (negative sensory deficit)
- Physical findings: piriformis tightness (slight), TFL tightness (more pronounced)
Anatomical Basis - Why This Pattern Makes Sense
The piriformis originates from the anterior sacrum and inserts on the medial aspect of the greater trochanter. It is a primary external rotator when the hip is extended, and an abductor when the hip is flexed. The sciatic nerve (L4-S3) normally passes below the piriformis through the greater sciatic foramen - in anatomical variants, it may pass through or above the muscle.
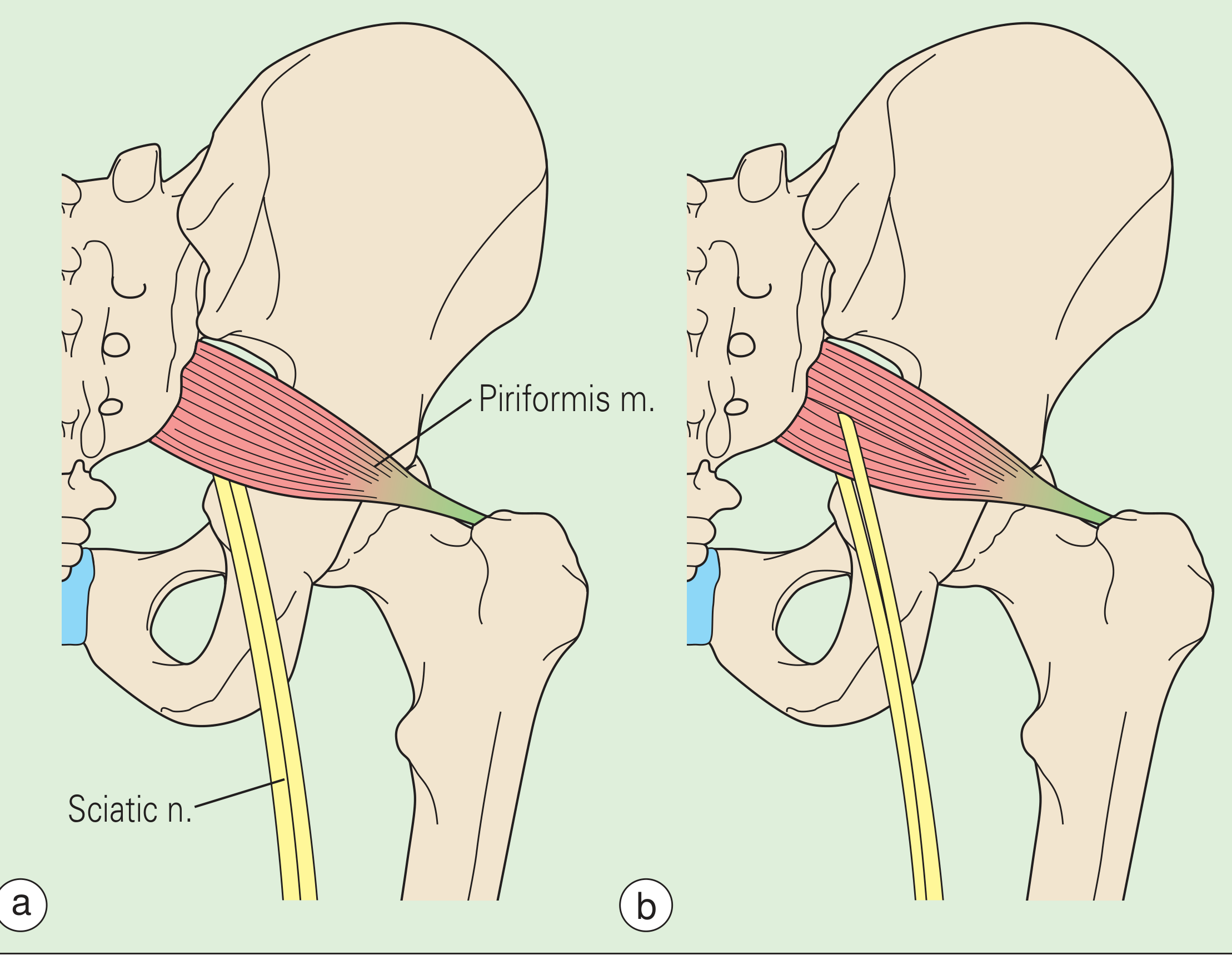
Piriformis and sciatic nerve relationship. (a) Normal: sciatic nerve passes below. (b) Anatomic variant: nerve traverses the muscle - increasing susceptibility to compression. (Rheumatology, 2-Volume Set, Elsevier)
The TFL originates from the ASIS and iliac crest, inserts into the IT band, and acts as a hip flexor, internal rotator, and abductor. Tightness here creates a biomechanical imbalance - when the TFL is overactive, the deep external rotators (including piriformis) are often inhibited and then compensatorily overloaded.
Most Likely Primary Diagnosis
Piriformis Syndrome (with secondary TFL overactivation)
This fits the presentation very closely. The key features from the textbooks:
| Feature | Your Patient | Piriformis Syndrome |
|---|---|---|
| Buttock / posterior thigh pain | ✅ | Classic |
| Pain radiating down leg | ✅ | Sciatic nerve irritation |
| No numbness | ✅ | Neurologic exam typically negative |
| Pain worsens with external rotation | ✅ | Muscle contraction stretches nerve at insertion |
| Piriformis tightness on exam | ✅ | Muscle spasm/tenderness |
| TFL tightness | ✅ | Compensatory mechanism |
Per Barash, Cullen, and Stoelting's Clinical Anesthesia 9e (p.4759), piriformis syndrome "comprises 5% of patients referred for treatment of back and leg pain." Pain extends from the sacrum to the greater trochanter, and sciatic irritation produces radiation to the ipsilateral leg. Importantly, neurologic examination is typically negative - matching your patient's absence of numbness.
Per Rheumatology, 2-Volume Set (p.771): "Maneuvers that internally rotate, flex, and adduct the hip often aggravate pain because such motion stretches the piriformis muscle." Note the inverse: if the piriformis is already tight and in sustained external rotation (i.e., contracted), nerve compression worsens as the muscle bulk increases around the nerve.
Why pain worsens with external rotation specifically:
- In the extended hip, the piriformis is an external rotator. Sustained external rotation keeps the piriformis in a contracted, shortened state - this increases intramuscular pressure, compresses the sciatic nerve against adjacent structures, and produces progressive aching that escalates with time.
- This is slightly different from the classical Freiberg sign (pain on forced internal rotation stretching the muscle), but makes sense as a pain-on-contraction pattern when the muscle is already in spasm or has active trigger points.
The adductor component:
The adductor pain and thigh radiation is best explained by:
- Referred pain from the obturator nerve - the obturator nerve (L2-L4) passes close to the posterior hip and can be irritated in deep gluteal/piriformis pathology. It innervates the adductors and refers medial thigh pain.
- Myofascial referral from piriformis trigger points - active trigger points in the piriformis classically refer pain to the sacroiliac joint, buttock, and posterior-medial thigh down the leg.
- Sciatic nerve has a common peroneal division that when irritated produces wide referral patterns including the anteromedial thigh via L2-L3 dermatomal overlap.
Differential Diagnoses to Consider
1. Deep Gluteal Syndrome (DGS)
This is a broader, more current term that encompasses piriformis syndrome plus entrapment of the sciatic nerve anywhere in the deep gluteal space (by gemelli, obturator internus, quadratus femoris, or fibrovascular bands). A 2023 systematic review (PMID: 37949567) specifically addressed conservative and surgical treatments for DGS, noting that piriformis syndrome may be a subset of this entity. Consider this if the patient doesn't respond to isolated piriformis treatment.
2. TFL / IT Band Myofascial Pain
Your finding of more TFL tightness than piriformis tightness is significant. Per Tintinalli's Emergency Medicine (p.1940), fascia lata syndrome causes lateral thigh pain with trigger points, and TFL enlargement occurs with overuse. A tight TFL pulls the pelvis into anterior tilt and causes internal rotation at the femur - this makes the external rotators (piriformis, obturator internus) work harder to stabilize, leading to their secondary tightening and eventual sciatic irritation.
Clinical implication: The TFL tightness may be the primary driver here, with piriformis involvement as a secondary/reactive phenomenon. This alters the rehabilitation approach substantially.
3. Obturator Nerve Entrapment
- Explains the adductor pain specifically
- Obturator nerve (L2-L4) runs along the lateral pelvic wall through the obturator canal
- Entrapment produces medial thigh pain, adductor weakness, and pain on resisted hip adduction
- Can co-exist with piriformis syndrome
4. Hamstring Proximal Tendinopathy / High Hamstring Syndrome
- Proximal hamstring insertional pain at the ischial tuberosity
- Dull aching posterior thigh pain
- Can mimic piriformis syndrome
- Worsens with sitting (compression of ischial tuberosity) and hip flexion
5. L4-L5 / L5-S1 Radiculopathy (Less Likely)
- Must always be excluded, especially when leg pain is present
- Your patient has no numbness and the pain is position-dependent (external rotation) - this argues against a central disc cause
- SLR and neurological exam should be normal in piriformis syndrome
- Per Rheumatology textbook: "it is unusual for patients with piriformis syndrome to have neurologic defects"
6. Sacroiliac Joint Dysfunction
- SI joint pain can refer to the posterior thigh and occasionally down the leg
- Should be ruled out by provocative SI joint tests (FABER, sacral compression, thigh thrust test)
Key Examination Tests to Perform / Confirm
| Test | What it Detects | Expected Finding |
|---|---|---|
| Pace Sign | Resisted hip abduction in seated position | Pain = piriformis syndrome |
| Freiberg Sign | Pain on forced internal rotation of extended thigh | Pain = piriformis irritation |
| FADIR test | Flexion-Adduction-Internal Rotation | Stretches piriformis; pain confirms |
| FAIR test (for EMG) | H-reflex delay with hip in FAIR position | Gold standard for piriformis syndrome |
| Straight Leg Raise | L4-S1 nerve root | Should be negative or mildly limited |
| Ober's Test | IT band / TFL tightness | Positive given your finding |
| Resisted adduction | Obturator nerve / adductor strain | If painful, suggests obturator involvement |
| SIJ provocation tests | FABER, thigh thrust | Rule out sacroiliac cause |
Proposed Diagnosis Hierarchy
- Primary: Piriformis syndrome - with myofascial component (possible trigger points)
- Contributing: TFL tightness with biomechanical overload - this may be causally upstream
- Associated: Possible obturator nerve irritation - explaining adductor pain
- Exclusion needed: L4-L5/L5-S1 radiculopathy, SI joint dysfunction
Management Approach
Phase 1 - Acute/Subacute
- NSAIDs for myofascial inflammation
- Muscle relaxants if significant spasm is present
- Avoid sustained external rotation postures (driver position, cross-legged sitting)
Phase 2 - Physical Therapy (Priority)
- TFL stretching first - since TFL is more tight, address this before the piriformis
- Standing hip flexor stretch with focus on lateral fascia
- IT band foam rolling
- Piriformis stretching - figure-4 stretch (supine or seated), pigeon pose variant
- Hip internal rotator strengthening to counterbalance the external rotator dominance
- Gluteus medius activation - weak glutes often cause TFL over-recruitment
- Core stabilization - reduces compensatory demand on hip rotators
Phase 3 - If Conservative Fails
- Ultrasound-guided piriformis injection (local anesthetic + corticosteroid) - well-supported in literature; equal efficacy for fluoroscopy and US guidance
- Botulinum toxin A (100 units) - if steroid injection gives only transient relief, BTX-A is effective (per Clinical Anesthesia 9e)
- Dry needling of TFL and piriformis trigger points
- Perisciatic steroid injection if there is significant sciatic nerve irritation
Imaging if Needed
- MRI pelvis - gold standard for detecting piriformis muscle changes, sciatic nerve relationship, and ruling out pelvic mass or disc herniation
- Dynamic ultrasound - useful for TFL/IT band assessment and guiding injections
Summary
Your patient most likely has piriformis syndrome with a significant TFL/IT band component as a biomechanical upstream cause. The absence of numbness, the position-dependent aching character, and the soft tissue findings on exam fit this diagnosis well. The adductor radiation suggests either myofascial referral from piriformis trigger points or secondary obturator nerve irritation. L4-L5/L5-S1 radiculopathy and SI joint dysfunction should be excluded by clinical testing.
The treatment priority should be TFL stretching first (given it is the tighter structure), followed by piriformis-specific therapy and sciatic nerve neural mobilization. If no response in 6-8 weeks, proceed to guided injection.
Sources: Rheumatology 2-Volume Set (Elsevier 2022), p. 771; Barash, Cullen & Stoelting's Clinical Anesthesia 9e, p. 4759-4760; Tintinalli's Emergency Medicine, p. 1940; Systematic Review on Deep Gluteal Syndrome (PMID 37949567); Piriformis Syndrome Systematic Review of Case Reports (PMID 41068685)

IMG_1074.jpg
How to perform these tests
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I have all the information needed. Here is the complete step-by-step guide for all 6 tests.
How to Perform These 6 Tests
1. PACE SIGN
Target: Piriformis muscle | Position: Seated
How to Perform:
- Patient sits on the edge of the examination table with hips flexed at ~90°
- Ask the patient to abduct both thighs simultaneously against your resistance
- Place your hands on the lateral aspects of both knees and apply inward (adduction) resistance
- Alternatively, test one side at a time by placing one hand on the lateral knee
Positive Sign:
Pain AND weakness on resisted hip abduction in the seated position = positive Pace sign
What it detects:
The piriformis is an abductor when the hip is flexed. Resisted contraction in the piriformis reproduces pain when it is in spasm or compressing the sciatic nerve.
"The Pace sign, wherein there is pain and weakness on resisted abduction of the hip in a patient who is seated with the hip flexed."
- Barash, Cullen & Stoelting's Clinical Anesthesia 9e
2. FREIBERG SIGN
Target: Piriformis muscle (stretching mechanism) | Position: Supine
How to Perform:
- Patient lies supine on the examination table
- Keep the test leg extended (flat on the table)
- Grasp the ankle/foot with one hand and place the other hand on the knee for control
- Apply forced passive internal rotation of the extended thigh
- The foot turns inward while the leg remains straight
Positive Sign:
Pain in the buttock / posterior thigh on forced internal rotation of the extended thigh = positive Freiberg sign
What it detects:
With the hip extended, the piriformis is an external rotator. Forcing it into internal rotation passively stretches the piriformis muscle, compressing the sciatic nerve if the muscle is tight or inflamed.
"The Freiberg sign, wherein there is pain on forced internal rotation of the extended thigh."
- Barash, Cullen & Stoelting's Clinical Anesthesia 9e
3. FADIR TEST
Target: Piriformis / deep gluteal space + hip impingement | Position: Supine

FADIR test: Flexion, Adduction, and Internal Rotation of the hip. (Campbell's Operative Orthopaedics 15th Ed)
How to Perform:
- Patient lies supine
- Flex the hip to 90 degrees (knee also flexed)
- Adduct the thigh across the midline (bring knee toward the opposite shoulder)
- Apply maximal internal rotation of the hip (turn the foot outward / laterally)
- Hold this combined position for a few seconds
Positive Sign:
Pain in the buttock or posterior thigh = piriformis / deep gluteal syndrome
Pain in the anterior groin = femoroacetabular impingement (FAI)
Key Point:
Compare internal rotation range with the contralateral side - there is significant individual variation. In piriformis syndrome, this position stretches the piriformis over the sciatic nerve, reproducing sciatic irritation.
"The hip is flexed to 90 degrees, with adduction across the midline, and maximal internal rotation of the hip."
- Campbell's Operative Orthopaedics 15th Ed 2026
4. FAIR TEST (for EMG/Clinical)
Target: Sciatic nerve at piriformis level | Position: Lateral decubitus
How to Perform (Clinical version):
- Patient lies in the lateral decubitus position with the affected side up
- The test leg is placed in hip Flexion + Adduction + Internal Rotation (FAIR position)
- Flex the hip to ~60°
- Allow the hip to fall into adduction (gravity assists)
- Internally rotate the hip (turn the knee downward)
- Maintain this position for 30-60 seconds
For EMG use:
The H-reflex of the tibial nerve is measured with the limb in FAIR position and compared to the normal anatomical position. A delay in H-reflex in the FAIR position vs. neutral = electrodiagnostic confirmation of piriformis syndrome (sciatic nerve conduction is slowed due to piriformis compression).
Positive Sign (Clinical):
Reproduction of buttock pain radiating down the leg in the FAIR position = positive test
What it detects:
This is the most sensitive and specific test for piriformis syndrome. The FAIR position places maximum stretch on the piriformis while simultaneously compressing the sciatic nerve, making it the gold standard for clinical and electrophysiologic diagnosis.
"Electromyography may detect myopathic and neuropathic changes, including a delay in the H-reflex, with the affected leg in a flexed, adducted, and internally rotated (FADIR) position as compared with the same H-reflex in the normal anatomic position."
- Barash, Cullen & Stoelting's Clinical Anesthesia 9e
5. STRAIGHT LEG RAISE (SLR / Lasègue Test)
Target: Sciatic nerve / L4-L5, L5-S1 nerve roots | Position: Supine

Step (a) of Lasègue's SLR test - initial passive hip movement assessment with knee bent. (Bailey & Love's Surgery 28th Ed)
How to Perform (3-step technique):
Step 1: With the patient supine, elevate the leg with the knee bent - this checks pain-free range of hip movement without nerve tension
Step 2: Straighten the knee while maintaining hip flexion - note the angle at which hamstrings allow the hip to flex. This is the baseline hamstring length
Step 3: Allow the hip to extend slightly until hamstring tension is relieved, then apply firm ankle dorsiflexion - this applies the final sciatic nerve tension
Positive Sign:
Pain radiating down the leg (below the knee, in a dermatomal pattern) = positive SLR
- Positive at 30-70° = most significant (nerve root tension)
- Positive at >70° = less specific (may be hamstring tightness)
- Normal individuals can raise to ~90° without pain
Interpretation for your patient:
In piriformis syndrome, the SLR should be negative or mildly limited (not strongly positive). A strongly positive SLR with leg pain below the knee suggests disc herniation at L4-L5 or L5-S1 rather than piriformis syndrome.
"With the patient supine, elevate the leg with the knee bent to check pain-free movement of the hip. Then, straighten the knee and note the angle at which the hamstrings allow the hip to flex. Finally, allow the hip to extend until tension is removed from the hamstring muscles and then the ankle is dorsiflexed firmly."
- Bailey & Love's Short Practice of Surgery 28th Ed
6. OBER'S TEST
Target: TFL / IT band tightness | Position: Lateral decubitus
How to Perform:
- Patient lies in the lateral decubitus position with the affected side up
- The bottom leg is slightly flexed at the hip and knee for stability
- Stabilize the pelvis with one hand to prevent pelvic tilt/rotation
- With the other hand, support the test leg at the knee
- Abduct and extend the hip slightly past neutral (hip extended, not flexed)
- Flex the knee to 90°
- Release the leg and allow it to fall toward the table under gravity
Positive Sign:
The leg fails to adduct (drop toward the table) or drops only slowly/with restriction = positive Ober test = IT band / TFL tightness
Two interpretations:
| Hip Position | Positive = Tight Structure |
|---|---|
| Hip extended past neutral | IT band / TFL tightness |
| Hip in neutral flexion/extension | Gluteus medius contracture |
For your patient:
Given your finding of more TFL tightness than piriformis, you should expect a clearly positive Ober test with the hip extended. This confirms the TFL/IT band is contributing to the biomechanical overload on the piriformis.
"With the patient in a lateral position, the hip is abducted with the knee flexed and then allowed to fall into adduction. A positive test is demonstrated by delay in adduction caused by gravity."
- Campbell's Operative Orthopaedics 15th Ed 2026
Quick Reference Summary
| Test | Position | Action | Positive = |
|---|---|---|---|
| Pace Sign | Seated | Resisted hip abduction | Pain + weakness |
| Freiberg Sign | Supine, leg extended | Forced passive IR of thigh | Buttock/posterior thigh pain |
| FADIR | Supine | Flex 90° + Adduct + IR | Posterior pain (piriformis) / Groin pain (FAI) |
| FAIR | Lateral / Supine | Flex + Adduct + IR, hold or EMG | Sciatic radiation; H-reflex delay |
| SLR | Supine | Passive leg raise + dorsiflexion | Radiating leg pain below knee |
| Ober's | Lateral | Abduct-extend-release | Leg fails to adduct (IT band tight) |
Clinical tip: For piriformis syndrome, Pace + FADIR + FAIR are the most diagnostically useful trio. Ober's test is crucial for your patient specifically given the prominent TFL tightness. SLR helps rule out a lumbar disc cause.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Bailey & Love's Surgery 28th Ed; Rheumatology 2-Volume Set (Elsevier 2022)
Treatment for piriformis syndrome with tfl tightness due to overload
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
piriformis syndrome treatment exercise injection
Reading File
Reading File
Finding Sources
Reading Article
PMID: 40016058
I now have comprehensive data from multiple authoritative sources. Here is the complete, structured treatment protocol.
Treatment: Piriformis Syndrome with TFL Overload
The key principle in this combined presentation is that TFL tightness is the upstream driver - it causes biomechanical overload on the piriformis and deep external rotators, which become secondarily reactive. Treatment must address both simultaneously, but in the right sequence.
PHASE 1 - Pain Control & Load Reduction (Week 1-2)
Activity Modification
- Avoid sustained external rotation postures (cross-legged sitting, "figure-4" resting position, driver's hip position) - these keep the piriformis in a contracted state and worsen nerve compression
- Avoid prolonged sitting (>30 min without a break) - pirifomis is compressed against the sciatic nerve in sitting
- Avoid activities that consistently aggravate: cycling, stair climbing (loads TFL heavily), and deep squats
Medications
- NSAIDs (e.g., ibuprofen 400-600 mg TDS with food, or diclofenac) - reduce myofascial inflammation
- Muscle relaxants (e.g., cyclobenzaprine, methocarbamol) - break the pain-spasm cycle in both piriformis and TFL
- Topical NSAIDs over the TFL/lateral thigh if systemic NSAIDs are not tolerated
"Physical therapy combined with medications such as muscle relaxants, anti-inflammatory drugs, and analgesics to reduce the spasm, inflammation, and pain."
- Barash, Cullen & Stoelting's Clinical Anesthesia 9e
PHASE 2 - Manual Therapy & Trigger Point Work (Week 1-3, alongside Phase 1)
TFL / IT Band - Address First (it's the tighter structure)
Foam rolling / soft tissue mobilization:
- Patient in side-lying position, upper affected leg resting on foam roller placed at the lateral thigh
- Roll slowly from ASIS (anterior superior iliac spine) down to just above the lateral knee
- Pause on any tender spots for 30-60 seconds
- Do this before any stretching - it reduces IT band stiffness and allows better stretch
Myofascial release of TFL:
- Direct pressure technique: therapist applies sustained pressure with thumbs or elbow just inferior and posterior to the ASIS where TFL originates
- Combined with active hip movement (patient slowly flexes and extends hip while pressure is maintained)
Piriformis - Trigger Point Therapy
- Cold spray and stretch technique: apply vapocoolant spray (ethyl chloride) along the piriformis in a sweeping motion (from sacrum toward greater trochanter), immediately followed by passive internal rotation stretch of the hip
- Trigger point massage / ischemic compression: sustained digital pressure on the tender nodule in the mid-buttock for 60-90 seconds until the pain referral eases
- Dry needling of piriformis trigger points: highly effective - studies show efficacy comparable to local anesthetic injection
"The management of myofascial pain syndrome includes repeated application of a cold spray over the trigger point in line with the involved muscle fibers, followed by gentle massage of the trigger point and stretching of the affected muscle."
- Barash, Cullen & Stoelting's Clinical Anesthesia 9e
PHASE 3 - Stretching Protocol (Week 2-4)
Step 1: TFL / IT Band Stretching (Priority - stretch the tighter structure first)
Standing TFL stretch (Cross-leg lean):
- Patient stands upright, affected leg crossed behind the other leg
- Lean the trunk laterally away from the affected side (toward the opposite shoulder)
- The arm on the affected side reaches overhead and across
- Hold 30-45 seconds, repeat 3-4 times
- This creates a lateral bow stretch that elongates the IT band and TFL
Side-lying TFL stretch (Modified Ober):
- Patient lies on unaffected side
- Top (affected) leg is extended at the hip and allowed to drop toward the floor behind the body (adduction in extension)
- Can apply gentle overpressure at the knee to increase the stretch
- Hold 30-45 seconds x 3 sets
Step 2: Piriformis Stretching
Supine Figure-4 stretch (most accessible):
- Patient lies supine, affected knee bent
- Cross the affected ankle over the opposite thigh (just above the knee) - this creates a figure-4 shape
- Clasp hands behind the opposite thigh and gently pull both legs toward the chest
- The piriformis is stretched in flexion + external rotation
- Hold 30-60 seconds x 3 repetitions
Seated piriformis stretch:
- Sit upright on a chair, cross the affected leg over the other knee (ankle resting on opposite thigh)
- Lean the trunk forward gently while keeping the back straight
- This is well tolerated even for patients who find floor stretches difficult
FADIR stretch (therapist-assisted):
- Patient supine, therapist passively takes the hip into flexion 90°, adduction across midline, and internal rotation
- Hold 20-30 seconds - this is the most specific piriformis stretch (same position as the FADIR test)
"Treatment consists of exercises that include prolonged stretching of the piriformis muscle by flexion, adduction, and internal rotation of the hip."
- Bradley and Daroff's Neurology in Clinical Practice
Step 3: Hip Flexor Stretching (since TFL is also a hip flexor)
- Kneeling lunge stretch: step one foot forward into a lunge position, drop the back knee to the floor, tuck the pelvis posteriorly (posterior pelvic tilt) to isolate the hip flexors rather than lumbar extension
- Hold 45-60 seconds x 3 sets per side
PHASE 4 - Strengthening & Biomechanical Correction (Week 3-6)
This is the most critical phase for preventing recurrence. TFL overload happens because the gluteus medius is weak - when it fails, the TFL compensates. Strengthen what should be working.
Priority 1: Gluteus Medius Activation
The glute medius is the true hip abductor and stabilizer. When it's weak, the TFL hijacks the abductor role and becomes chronically overloaded.
Clamshells:
- Patient side-lying with hips flexed ~45°, knees bent
- Open the top knee like a clamshell while keeping the feet together and pelvis stable
- Resistance band around the thighs as progression
- 3 sets x 15 reps, slow and controlled
Side-lying hip abduction:
- Top leg lifts straight upward (not forward) - keep the foot in slight internal rotation to isolate glute medius over TFL
- 3 sets x 12-15 reps
Single-leg stance progression:
- Start with single-leg balance 30 seconds
- Progress to single-leg mini-squat (small knee bend)
- Finally progress to single-leg step-downs from a step
- This trains the glute medius in a functional, loaded position
Priority 2: External Hip Rotator Strengthening (Piriformis Rehabilitation)
Prone hip external rotation with knee bent (ER in extension):
- Patient lies prone, knee bent 90°
- Rotate the foot outward (toward the floor) against gravity or a resistance band
- 3 sets x 12-15 reps - this strengthens the piriformis and deep rotators in a controlled, pain-free range
Seated external rotation with resistance band:
- Sit upright, band looped around both knees
- Push knees outward against the band resistance
- 3 sets x 15 reps
Priority 3: Core and Pelvic Stability
A weak core causes anterior pelvic tilt, which increases TFL and hip flexor demand and inhibits gluteals.
- Dead bug exercise - supine, lower back pressed flat, alternate contralateral arm/leg extension
- Bird-dog - quadruped position, alternate arm/leg extension with neutral spine
- Bridges - supine, feet flat, lift pelvis to form a straight line from knees to shoulders; add single-leg bridge as progression
Priority 4: Neural Mobilization (for sciatic nerve irritation)
- Sciatic nerve flossing: Supine, perform SLR to the point of mild tension, then add ankle dorsiflexion (to tension) and release (plantarflexion) rhythmically - 10-15 repetitions
- This restores nerve mobility within the deep gluteal space and reduces neural sensitivity
- Do this gently - should not reproduce sharp pain, only a mild pulling sensation
PHASE 5 - Interventional Options (if no adequate response in 4-6 weeks)
1. Ultrasound-Guided Piriformis Injection
- Injection contents: Local anesthetic (lidocaine 1%) + corticosteroid (triamcinolone 40 mg or methylprednisolone 40 mg) in 3-5 mL total volume
- Guidance: Ultrasound is preferred (equal efficacy to fluoroscopy, no radiation, real-time visualization)
- A positive response (significant pain relief for several weeks) also serves as diagnostic confirmation of piriformis syndrome
- Note: The RCT (Fu et al., 2026, PMID: 40016058) found that ESWT and USI showed similar improvement rates - no significant difference in efficacy between the two approaches
2. Extracorporeal Shockwave Therapy (ESWT)
- Effective for both piriformis and TFL/IT band pathology
- 1-3 sessions typically (radial or focused ESWT over the piriformis region and lateral thigh)
- Per the 2026 RCT, ESWT produced significant improvements in VAS pain and Oswestry Disability Index comparable to corticosteroid injection
- Advantage over injection: No systemic side effects, can be repeated, good for the TFL component simultaneously
3. Botulinum Toxin A (when steroid injection gives only transient relief)
- 100 units of BTX-A in 2-3 mL local anesthetic, injected into the piriformis under imaging guidance
- Produces prolonged (3-4 months) muscle relaxation, breaking the chronic spasm cycle
- Reserved for refractory cases
"If relief from the local anesthetic is transient, then the piriformis muscle may be injected with 100 units of botulinum toxin A in 2-3 mL of local anesthetic."
- Barash, Cullen & Stoelting's Clinical Anesthesia 9e
4. Perisciatic Steroid Injection
- When the sciatic nerve component is prominent (significant leg radiation)
- Steroid deposited around the sciatic nerve in addition to the piriformis injection
- Reduces perineural inflammation contributing to the radiating pain
5. TFL / IT Band Injection
- Ultrasound-guided local anesthetic + steroid into the TFL muscle belly or IT band region
- Useful when TFL remains persistently tight despite stretching
PHASE 6 - Surgical (Rarely Needed)
Reserved for cases with:
- Clear structural compression (anatomical variant where sciatic nerve pierces piriformis)
- Failure of all conservative measures + injections over 6+ months
- Neurological deficit developing
Procedure: Surgical sectioning (release) of the piriformis muscle at its insertion on the greater trochanter, allowing reattachment in a shortened position. MR neurography pre-operatively is ideal to confirm sciatic nerve involvement.
Complete Treatment Timeline
| Week | Focus |
|---|---|
| 1-2 | Activity modification, NSAIDs, muscle relaxants, soft tissue massage |
| 1-3 | TFL foam rolling, trigger point therapy (cold spray + dry needling), piriformis massage |
| 2-4 | TFL stretching (priority), piriformis FADIR stretch, hip flexor stretch |
| 3-6 | Gluteus medius strengthening (clamshells, side-lying abduction), core stability, neural mobilization |
| 4-6 | Progress to functional loading: single-leg stance, step-downs |
| 6+ | If inadequate response: USG injection or ESWT |
| 6m+ | Surgical evaluation only if all else fails |
Key Principle to Reinforce to the Patient
The TFL does not just need to be stretched - it needs to be unloaded by activating the gluteus medius. Until the glute med is strong enough to do its job, the TFL will keep tightening. Stretching alone without strengthening produces temporary relief that keeps recurring. Stretching + glute activation = lasting resolution.
Sources: Barash, Cullen & Stoelting's Clinical Anesthesia 9e, p.4759-4760; Bradley and Daroff's Neurology in Clinical Practice; Rheumatology 2-Volume Set (Elsevier 2022), p.771; Fu et al. 2026 RCT - ESWT vs USI in piriformis syndrome, PMID 40016058
This is a shared conversation. Sign in to Orris to start your own chat.