What do you think of this movement for my shoulder pain? I lie down prone, internally rotate my arm and flex elbow to 90° in a manner that it's on my back now and fully adducted, then I lift my arm off my back and the shoulder that pains feels unstable af and also tight, other shoulder is also tight but not as much, and I hold it in that lifted position for 10s approx and stop, did it 3 times
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Based on what I've gathered from the orthopaedic literature, here's a clinical breakdown of what you're doing and what it likely means:
The Movement You're Describing
What you're doing is essentially a prone internal rotation + adduction arm lift — the arm is placed behind your back (internally rotated, elbow at 90°, fully adducted), then lifted off your back. This passively loads several structures simultaneously:
- Subscapularis (primary internal rotator)
- Posterior capsule (stretched in internal rotation across the back)
- Inferior glenohumeral ligament complex
- Rotator interval (the space between subscapularis and supraspinatus)
What the "Instability" Feeling Tells You
Feeling instability when lifting the arm off your back in this position is a notable finding. In clinical orthopaedics, the arm-behind-back position in internal rotation is used diagnostically:
- It tests subscapularis integrity — the lift-off test (Gerber's test) is exactly this: prone or standing, arm behind back, lifting off against resistance. Inability or pain with lift-off = subscapularis pathology (partial or full tear, or weakness).
- The instability sensation specifically suggests the humeral head is not being well-held in the glenoid during this motion — consistent with rotator cuff dysfunction (subscapularis and/or the inferior GHL complex) or posterior/multidirectional shoulder instability.
- Bilateral tightness (but worse on the symptomatic side) points toward posterior capsule tightness, which is extremely common in overhead athletes and people with shoulder impingement. A tight posterior capsule forces the humeral head to migrate anterosuperiorly, worsening impingement and instability.
Is This a Good Exercise/Test for You?
Mixed assessment — be cautious with this specific movement:
What it might be doing usefully:
- You're accidentally performing something close to a subscapularis activation/assessment and posterior capsule stretch simultaneously.
- Holding the lifted position can build subscapularis endurance, which is a legitimate rehab target.
Why to be careful:
- If the shoulder truly feels unstable (not just effortful or tight, but a sense the joint is "giving"), loading it in this position for 10 seconds under muscle fatigue is risky. An unstable glenohumeral joint under load in a vulnerable position risks labral stress, capsular stretch, or subluxation.
- This position (full internal rotation + adduction + loading) is not a standard therapeutic exercise — it's more of a clinical provocation/test.
- The fact that it feels significantly worse on the painful side compared to the other (which is "also tight but less so") suggests an asymmetric pathology, not just general tightness.
What You Likely Have (Based on the Presentation)
The combination of:
- Shoulder pain
- Instability with internal rotation lift-off
- Bilateral posterior capsule tightness (asymmetric)
...fits a pattern of rotator cuff dysfunction with posterior capsular tightness, possibly with glenohumeral instability (anterior or multidirectional). In younger, active people this commonly tracks to a GIRD pattern (Glenohumeral Internal Rotation Deficit) or early subscapularis/supraspinatus pathology.
Practical Advice
- Stop loading the unstable position until you have a diagnosis — the 10-second holds in an unstable position aren't helping and could stress already-compromised structures.
- The posterior capsule tightness is real and worth addressing — but with a sleeper stretch (lying on the painful side, internally rotating the forearm down toward the table with the opposite hand), which is safer and well-validated.
- Get a proper assessment: a Gerber lift-off test done by a physio/orthopod, along with Hawkins-Kennedy and apprehension/relocation tests, will clarify whether this is primarily impingement, subscapularis weakness, or instability.
- MRI (or at minimum shoulder ultrasound) if there's ongoing pain — subscapularis tears and posterior labral pathology are often missed without imaging.
The bottom line: what you're feeling is clinically meaningful, not nothing — but the exercise as you're doing it is more diagnostic provocation than therapeutic movement. Get it properly evaluated.
How to fix subscapularis pathologies
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
That image is exactly what's needed. Here's a comprehensive breakdown:
Fixing Subscapularis Pathology
The approach depends entirely on what kind of pathology you have — weakness/tendinopathy vs. partial tear vs. full tear. The textbook lays this out clearly by grade.
Classification & Treatment by Type
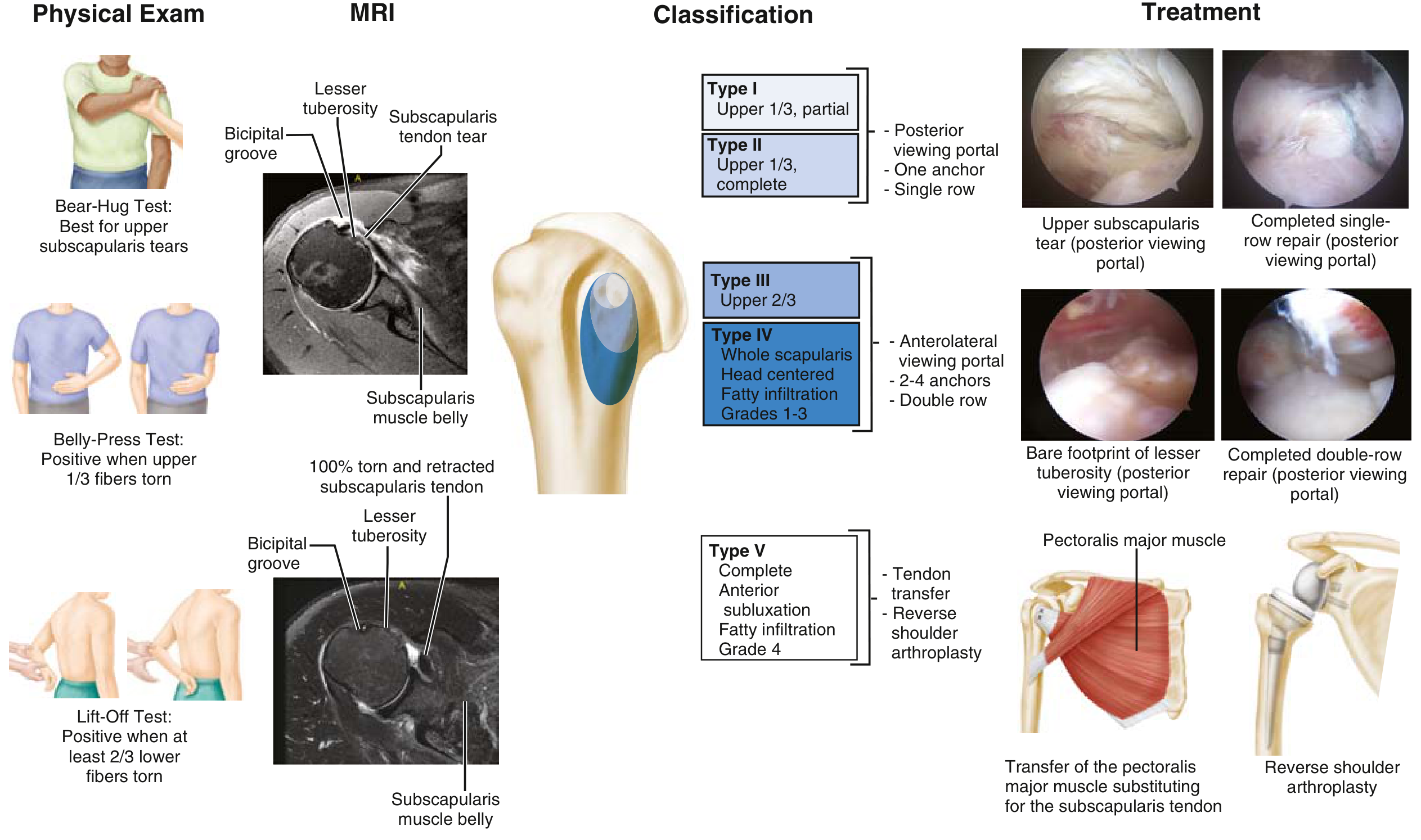
| Type | Extent | Surgical Treatment |
|---|---|---|
| I | Upper 1/3, partial | Posterior viewing portal, 1 anchor, single row |
| II | Upper 1/3, complete | Same |
| III | Upper 2/3 | Anterolateral portal, 2–4 anchors, double row |
| IV | Whole, fatty infiltration grades 1–3 | Same double-row repair |
| V | Complete + anterior subluxation, fatty infiltration grade 4 | Pectoralis major tendon transfer OR reverse shoulder arthroplasty |
Conservative (Non-Surgical) Management
For subscapularis tendinopathy, weakness, or minor partial tears (no structural failure), this is the first-line approach:
1. Activity modification
- Avoid aggressive internal rotation under load
- Avoid reaching behind the back with force
- No overhead pressing until pain-free
2. Strengthening progression
The subscapularis is the primary internal rotator and the main anterior stabilizer of the glenohumeral joint. Rehab targets it specifically:
- Internal rotation with band/cable — arm at side, elbow 90°, rotating inward against resistance (the most direct subscapularis exercise)
- Belly-press — standing, pressing palm into abdomen with wrist extended, holding elbow forward — isometric subscapularis activation, low load
- Bear-hug — hugging a medicine ball or resisted — loads upper subscapularis fibers specifically
- Low-to-high diagonal pulls (PNF D2 pattern) — incorporates subscapularis in functional arc
- Prone IR hold (your movement, modified) — only appropriate if the joint is stable and used at low load, not as a full lift-off; if you feel instability, skip this
3. Scapular stabilization
Subscapularis function depends on a stable scapular base. Weak serratus anterior or lower trapezius undermines all subscapularis work:
- Serratus push-ups / wall slides
- Scapular retraction with low rows
- Y-T-W raises prone
4. Posterior capsule stretching
Tightness there (which you have bilaterally) forces the humeral head forward and overloads the subscapularis:
- Sleeper stretch — lie on the painful side, elbow at 90°, press the forearm toward the table with the other hand; hold 30s, repeat 3x
- Cross-body stretch — pull the arm across the chest to stretch the posterior capsule
5. Anti-inflammatories / injection
- Short course NSAIDs for acute flares
- Subacromial or glenohumeral corticosteroid injection for persistent pain, but avoid within 6 months of any planned surgery as it increases repair failure rates
When Surgery Is Indicated
Per the orthopaedic literature:
- Failure of conservative management after a genuine 3–6 month trial
- Full-thickness tears (Types III–V) — surgical repair is generally indicated; chronic full tears don't heal on their own
- Acute complete tear — repair early before retraction and fatty atrophy set in (this process accelerates quickly)
- Type V (complete tear + severe fatty infiltration grade 4 + anterior subluxation) — beyond repair; pectoralis major tendon transfer or reverse total shoulder arthroplasty
The key prognostic factors for surgical failure are: age ≥65, massive tear, >50% fatty infiltration of the muscle belly on MRI, tear retraction to glenoid level, diabetes, and smoking.
Your Situation Specifically
Given that you have:
- Pain + instability sensation on one side
- Positive-ish lift-off (the movement you described)
- Bilateral posterior capsule tightness
You're most likely looking at early subscapularis dysfunction or partial pathology, not a full tear (full tears present with much more obvious weakness and external rotation excess). The conservative program above — especially internal rotation strengthening, scapular stability work, and sleeper stretches — is the correct first move. But get imaging (shoulder ultrasound or MRI) to rule out a structural tear before loading it aggressively.
This is a shared conversation. Sign in to Orris to start your own chat.