Kidney stones
Reading File
search_medical_text
kidney stones nephrolithiasis etiology types pathophysiology
search_medical_text
nephrolithiasis diagnosis management treatment
search_medical_image
kidney stone CT scan imaging types
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive overview of kidney stones (nephrolithiasis):
Kidney Stones (Nephrolithiasis)
Overview
Nephrolithiasis is a common, painful, and costly condition in which crystals of lithogenic material aggregate in the upper urinary tract. Stones can migrate into the ureter, causing renal colic — widely reported as among the worst pain a patient can experience. While rarely fatal, it carries significant morbidity and economic burden. (Harrison's, p. 8691)
Stone Types
| Type | Frequency | Key Associations |
|---|---|---|
| Calcium oxalate | ~75% | Hypercalciuria, hyperoxaluria, hypocitraturia |
| Calcium phosphate | ~15% | Renal tubular acidosis, hyperparathyroidism |
| Uric acid | ~8% | Gout, low urine pH, metabolic syndrome |
| Struvite | ~1% | Urease-producing bacteria (e.g., Proteus), UTIs |
| Cystine | <1% | Cystinuria (autosomal recessive) |
| Drug-induced | Rare | Acyclovir, atazanavir, triamterene |
Many stones are mixed (e.g., calcium oxalate + calcium phosphate). (Harrison's, p. 8691)
⚠️ Struvite (infection) stones can lead to end-stage renal disease if not adequately treated.
Risk Factors
- Low urine volume (dehydration) — the single most modifiable risk factor
- High dietary sodium, animal protein, oxalate (spinach, nuts, chocolate)
- Low dietary calcium (paradoxically increases oxalate absorption)
- Obesity, metabolic syndrome, type 2 diabetes (→ uric acid stones)
- Inflammatory bowel disease / bowel resection (→ hyperoxaluria)
- Hyperparathyroidism (→ hypercalciuria)
- Recurrent UTIs with urease-producing organisms (→ struvite)
Clinical Presentation
- Renal colic: severe, cramping, colicky flank pain radiating to the groin ("loin to groin")
- Nausea, vomiting
- Hematuria (gross or microscopic) — present in ~85% of cases
- Dysuria, urgency if stone is at the ureterovesical junction
- Fever/chills if concurrent infection (urological emergency)
Diagnosis
Imaging
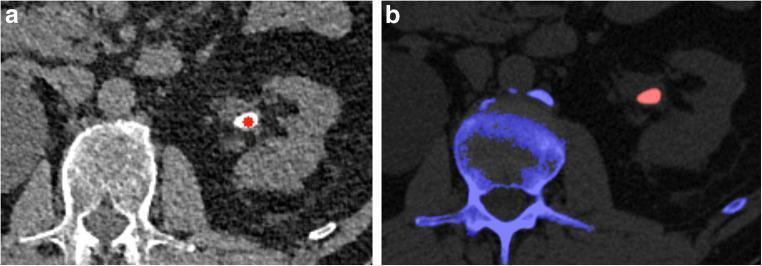
Non-contrast CT of the abdomen/pelvis is the gold standard — detects virtually all stone types, determines size and location.
- Ultrasound: preferred in pregnancy and children; lower sensitivity for small stones
- Plain X-ray (KUB): only detects radiopaque stones (calcium-based); misses uric acid and cystine stones
Labs
- Urinalysis: hematuria, crystalluria, pH (low pH → uric acid; high pH → struvite/calcium phosphate)
- BMP/CMP: creatinine, calcium, uric acid
- 24-hour urine collection (in recurrent stone formers): volume, calcium, oxalate, citrate, uric acid, sodium, pH
- Serum PTH if hypercalcemia is present
Management
Acute
| Situation | Action |
|---|---|
| Stone ≤5 mm | Medical expulsive therapy (MET): alpha-blockers (tamsulosin) + hydration + analgesia; ~80% pass spontaneously |
| Stone 5–10 mm | MET with close follow-up; ~50% pass spontaneously |
| Stone >10 mm | Likely requires intervention |
| Fever + obstruction | Urgent urology consult — infected obstructed kidney is a surgical emergency |
| Solitary kidney, bilateral obstruction, acute kidney injury | Urgent intervention |
Analgesia: NSAIDs (ketorolac) are first-line; opioids for refractory pain.
Interventional
- Shockwave lithotripsy (SWL): non-invasive; preferred for renal stones <2 cm
- Ureteroscopy (URS) with laser lithotripsy: highly effective for ureteral stones
- Percutaneous nephrolithotomy (PCNL): large stones (>2 cm) or staghorn calculi
Prevention (Stone-Type Specific)
Universal: Increase fluid intake to produce >2.5 L urine/day.
| Stone Type | Targeted Prevention |
|---|---|
| Calcium oxalate | Thiazide diuretics (↓ urinary calcium), potassium citrate (↑ citrate, ↑ pH), low-sodium/low-protein diet |
| Uric acid | Potassium citrate or sodium bicarbonate (alkalinize urine to pH 6.5–7), allopurinol if hyperuricosuria |
| Struvite | Complete stone removal + treat underlying infection; acetohydroxamic acid in refractory cases |
| Cystine | High fluid intake, alkalinization; D-penicillamine or tiopronin for refractory cases |
| Calcium phosphate | Thiazides, low-sodium diet; address underlying RTA or hyperparathyroidism |
Recurrence prevention should be personalized based on 24-hour urine metabolic workup and may be lifelong. (Harrison's, p. 8691)
Complications
- Urinary obstruction → hydronephrosis → AKI
- Urosepsis (infected obstructed system)
- Chronic kidney disease with recurrent/bilateral disease
- Chronic pain, reduced quality of life
Bottom line: Kidney stones are highly recurrent (~50% recurrence within 5–10 years without intervention), but recurrence is largely preventable with a proper metabolic workup and targeted dietary/pharmacologic measures tailored to stone type.
Can you make a diagnosis
I need a bit more information to help with a diagnosis. Could you tell me:
- What symptoms are you or the patient experiencing? (e.g., flank pain, blood in urine, nausea, fever)
- Where is the pain, if any? Does it radiate anywhere?
- Any relevant history — prior kidney stones, recent imaging, lab results, medical conditions?
- Any current medications or recent procedures?
The more detail you provide, the more useful I can be.
Pain in the big toe hurts while walking
Reading File
search_medical_text
gout podagra big toe diagnosis clinical presentation
search_medical_text
gout hyperuricemia treatment management acute flare
search_medical_image
gout podagra big toe swelling imaging
GradeResponse
GradeResponse
GradeResponse
Likely Diagnosis: Gout (Podagra)
The big toe is the most classic site for gout. The metatarsophalangeal (MTP) joint of the first toe is involved in 70–90% of cases, a presentation specifically called podagra. (Harrison's, p. 10430)
What Is Gout?
Gout is caused by chronic hyperuricemia (elevated uric acid in the blood), leading to the deposition of monosodium urate (MSU) crystals in joints. When crystals shed into the joint space, they trigger intense inflammation — an acute gout flare. (Harrison's, p. 10429)
This also connects to what was discussed earlier: high uric acid causes both gout and uric acid kidney stones.
Classic Features That Point to Gout
| Feature | Details |
|---|---|
| Location | First MTP joint (big toe) — most common site |
| Pain onset | Often starts at night or early morning |
| Joint appearance | Warm, red, tender, swollen — can mimic cellulitis |
| Duration | Flares typically resolve in 1–2 weeks on their own |
| Pattern | Attacks then symptom-free intervals (intercritical gout) |
Imaging in Chronic Gout
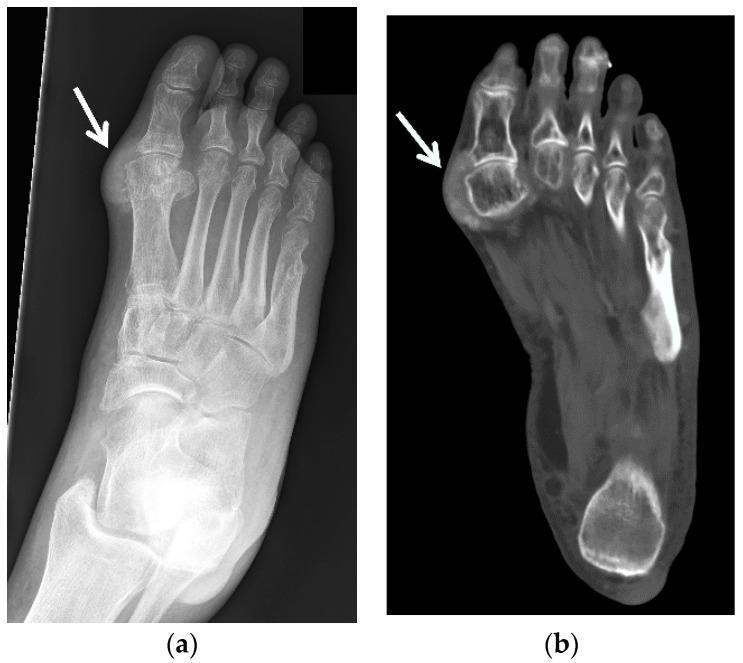
In early/acute gout, imaging may be normal. These findings develop with chronic, recurrent disease.
How to Confirm the Diagnosis
- Serum uric acid — often elevated, but can be normal during an acute flare
- Joint aspiration (arthrocentesis) — gold standard; shows needle-shaped, negatively birefringent MSU crystals under polarized light microscopy
- Ultrasound — can show "double contour sign" (urate coating cartilage)
- X-ray — normal early; punched-out erosions in chronic disease
Treatment
Acute Flare
- NSAIDs (e.g., indomethacin, naproxen) — first-line
- Colchicine — very effective if started early (within 24–36 hours of onset)
- Corticosteroids (oral prednisone or intra-articular injection) — if NSAIDs/colchicine are contraindicated
Long-Term (Urate-Lowering Therapy)
Started after the acute flare resolves, indicated for recurrent attacks, tophi, or uric acid kidney stones:
- Allopurinol — first-line; inhibits xanthine oxidase to reduce uric acid production
- Febuxostat — alternative xanthine oxidase inhibitor
- Probenecid — increases renal uric acid excretion (avoid if kidney stones present)
Target serum uric acid: <6 mg/dL (or <5 mg/dL with tophi)
Lifestyle
- Reduce red meat, organ meats, shellfish, alcohol (especially beer)
- Stay well hydrated
- Avoid fructose-sweetened beverages
- Lose weight if overweight
Important note: This is a clinical assessment based on the symptoms described. A formal diagnosis requires examination and likely blood work or joint fluid analysis by a healthcare provider. If the toe is also red, warm, and swollen — especially with fever — see a doctor promptly to rule out a joint infection (septic arthritis), which is a medical emergency.
This is a shared conversation. Sign in to Orris to start your own chat.