Sgarbossa score
Reading File
Finding Sources
Searching Images
Sgarbossa criteria ECG left bundle branch block
Reading File
Loading Image
Here is a comprehensive breakdown of the Sgarbossa Criteria — a scoring system for diagnosing acute MI in the presence of Left Bundle Branch Block (LBBB) or ventricular paced rhythm, where normal STEMI criteria don't apply.
Background
In LBBB, baseline ST-segment and T-wave changes are expected (discordant ST changes — opposite to the main QRS deflection). This makes diagnosing AMI on ECG challenging. Sgarbossa et al. derived three independent ECG predictors of AMI from the GUSTO-1 trial database (NEJM 1996).
Original Sgarbossa Criteria (Weighted Score)
| Criterion | Description | Points |
|---|---|---|
| 1. Concordant STE | ST elevation ≥ 1 mm in a lead where the QRS is positive (concordant) | 5 |
| 2. Concordant STD | ST depression ≥ 1 mm in leads V1–V3 (concordant — QRS mainly negative here in LBBB) | 3 |
| 3. Discordant STE | ST elevation ≥ 5 mm in a lead where the QRS is negative (discordant) | 2 |
Interpretation: A total score ≥ 3 achieves ~90% specificity for AMI.
- Criterion 1 alone (score = 5) → highly specific
- Criterion 2 alone (score = 3) → meets threshold
- Criterion 3 alone (score = 2) → does NOT meet threshold; needs additional criteria or workup
Modified Sgarbossa Criteria (Smith, 2012)
The original criterion 3 (discordant STE ≥ 5 mm) has poor sensitivity. The modified criteria replace it with a ratio-based rule:
ST/S ratio: Discordant ST elevation amplitude ÷ S-wave depth
- ST/S ratio ≤ −0.25 (i.e., STE is >25% of the S-wave depth) = diagnostic of AMI
- This removes the arbitrary 5 mm cutoff and accounts for QRS amplitude variation
- Increases sensitivity without significant loss of specificity
Visual Summary
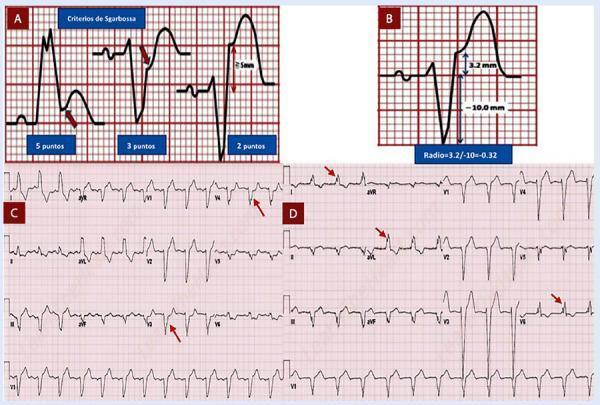
Panel A: Original three Sgarbossa criteria (5, 3, 2 points). Panel B: Modified Sgarbossa — ST/S ratio of 3.2/−10.0 = −0.32 (exceeds 0.25 threshold → AMI). Panels C & D: Real 12-lead ECG examples.
Key Clinical Points
- Applies to both LBBB and ventricular paced rhythm (pacemaker creates similar baseline ST distortion)
- New or presumably new LBBB in a patient with chest pain is high-risk even if Sgarbossa criteria are not met — treat as potential AMI
- A LBBB that does NOT meet Sgarbossa criteria is still a marker of significant cardiovascular risk
- Serial ECGs, echocardiography, and troponins are important adjuncts when ECG is non-diagnostic
- Sgarbossa criteria do not apply to RBBB (the repolarization pattern differs)
Practical Approach
- Is the ST change concordant? (same direction as main QRS deflection)
- STE ≥ 1 mm concordant → strong evidence of AMI (5 pts)
- STD ≥ 1 mm in V1–V3 concordant → moderate evidence (3 pts)
- Is there excessive discordant STE?
- Classic: ≥ 5 mm → weak evidence (2 pts)
- Modified: ST/S ratio ≤ −0.25 → positive (better rule)
- Score ≥ 3 or any single concordant finding → treat as STEMI equivalent, consider emergent cath
— ROSEN's Emergency Medicine: Concepts and Clinical Practice; The Washington Manual of Medical Therapeutics

Interpretation
ECG Interpretation
Patient details visible: HR ~91 bpm, BP 140/80 (handwritten), BSL 140 mg/dL, 12-lead ECG
Rhythm & Rate
- Rate: ~91 bpm (regular)
- Rhythm: Sinus rhythm
Key Findings
1. LBBB (Left Bundle Branch Block) ✅
- Wide QRS complexes (visually >120 ms)
- Broad monophasic R waves in I, aVL, V5, V6
- Deep S waves / rS pattern in V1–V3
- Discordant ST-T changes (expected in LBBB)
2. Machine Interpretation confirms:
- "Atrial Enlargement"
- "Atrial Infarction (Recent)"
- "Abnormality (Negative T)" — likely referring to T-wave inversions
Applying Sgarbossa Criteria (given LBBB)
| Criterion | Finding on this ECG |
|---|---|
| Concordant STE ≥ 1 mm | Possible in lateral leads (V5–V6, I) — look for STE in same direction as QRS |
| Concordant STD ≥ 1 mm in V1–V3 | V1–V3 show deep S waves; ST changes need careful measurement |
| Discordant STE ≥ 5 mm | Present in V1–V3 (expected in LBBB — need to assess if excessive) |
From the ECG image, there appear to be:
- Deeper-than-expected discordant ST changes in V1–V3 — assess ST/S ratio (Modified Sgarbossa)
- Lateral lead ST morphology — the ST segments in V5–V6 should be scrutinized for concordant elevation
Machine Diagnosis: "Atrial Infarction (Recent)"
This is an uncommon but recognized pattern — atrial MI can cause:
- PR segment elevation in aVR with PR depression in lateral leads
- Abnormal P wave morphology
- The machine flag warrants clinical correlation
Summary Interpretation
Sinus rhythm at ~91 bpm with LBBB (likely pre-existing or new — clinically critical to determine). Machine flags recent infarction. Sgarbossa criteria should be formally applied with caliper measurement.
⚠️ Clinical Bottom Line
Given the LBBB + machine flag of "recent infarction" + BSL 140 + BP 140/80:
- New LBBB in a chest pain patient = STEMI equivalent until proven otherwise
- Apply Modified Sgarbossa (ST/S ratio ≤ −0.25 in any lead = positive)
- Serial ECGs, troponins, and urgent cardiology review are mandatory
- Compare with any prior ECG to determine if LBBB is new
This ECG requires urgent clinical correlation — do not rely solely on machine interpretation.
Why this is not AIVR?
Great clinical question. Here's why this ECG is not AIVR:
AIVR vs LBBB — Key Differentiators
What is AIVR?
Accelerated Idioventricular Rhythm = ventricular escape rhythm that "accelerates" to 40–120 bpm, producing wide QRS complexes.
Why This ECG is NOT AIVR
1. P waves are present and conducting ✅
- In this ECG, P waves precede every QRS with a consistent PR interval
- AIVR is an AV-dissociated rhythm — P waves are either absent, dissociated, or retrograde
- Here, sinus node is in control → rules out AIVR by definition
2. Rate is 91 bpm
| Rhythm | Typical Rate |
|---|---|
| Idioventricular (escape) | 20–40 bpm |
| AIVR | 40–120 bpm |
| Ventricular tachycardia | >120 bpm |
- Rate of 91 bpm is within AIVR range numerically, but — the presence of conducted P waves excludes it
3. QRS morphology is LBBB-pattern, not typical ventricular origin
- AIVR typically originates from the right ventricle → produces an LBBB-like pattern (which can cause confusion)
- However, LBBB from a supraventricular origin has:
- Consistent QRS morphology beat to beat ✅
- Fixed PR interval ✅
- No fusion beats (fusion beats = hallmark of AIVR/VT)
- AIVR characteristically shows fusion beats at onset and termination as the ventricular focus competes with the sinus node
4. No AV Dissociation
- AIVR requires AV dissociation (ventricles fire independently of atria)
- This ECG shows 1:1 P:QRS relationship → purely supraventricular conduction with aberrancy (LBBB)
5. Clinical Context
- AIVR is classically seen in:
- Reperfusion (post-thrombolysis / post-PCI) — "reperfusion arrhythmia"
- Acute inferior MI
- Digoxin toxicity
- Cocaine use
- This patient has hypertension + elevated BSL — more consistent with a chronic LBBB substrate
Summary Table
| Feature | This ECG | AIVR |
|---|---|---|
| P waves | Present, conducting | Absent / dissociated |
| PR interval | Fixed, normal | None or variable |
| AV relationship | 1:1 | Dissociated |
| Fusion beats | None | Typically present |
| QRS origin | Supraventricular + BBB | Ventricular (ectopic focus) |
| Rate | 91 bpm (sinus-driven) | 40–120 bpm (ventricular-driven) |
Bottom line: The wide QRS in this ECG is due to aberrant conduction (LBBB) from a sinus-driven impulse — not a ventricular ectopic focus. The presence of conducted P waves with a fixed PR interval is the single most important distinguishing feature.
This is a shared conversation. Sign in to Orris to start your own chat.