Distal radius fractures displacements
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
distal radius fracture Colles Smith Barton displacement types
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have enough material for a comprehensive answer. Here's a structured overview of distal radius fracture displacements:
Distal Radius Fracture Displacements
Normal Radiographic Anatomy ("11-22-11" Rule)
Before assessing displacement, know the baseline:
- Radial height: 11 mm
- Radial inclination: 22°
- Volar tilt: 11°
Acceptable post-reduction parameters: radial shortening <3 mm, dorsal tilt <10°, intra-articular step-off <2 mm.
— Miller's Review of Orthopaedics, 9th Ed.
Eponymous Fracture-Displacement Patterns
1. Colles Fracture — Dorsal Displacement
- Mechanism: Fall on an outstretched hand (FOOSH) — the most common pattern
- Pattern: Transverse fracture of the distal radial metaphysis, extra-articular
- Displacement: Distal fragment displaced and angulated dorsally (apex volar); produces the classic "dinner fork" deformity
- Key: The carpus follows the displaced fragment
"A Colles fracture is a transverse fracture of the distal radial metaphysis, which is dorsally displaced and angulated." — Rosen's Emergency Medicine, 10th Ed.
Lateral X-ray — Colles fracture (dorsal displacement):

2. Smith Fracture ("Reverse Colles") — Volar Displacement
- Mechanism: Fall on the dorsum of the hand, or direct blow to the dorsum
- Pattern: Transverse metaphyseal fracture, usually extra-articular
- Displacement: Distal fragment displaced and angulated volarly (apex dorsal); produces a "garden spade" deformity
- Key: Opposite direction to Colles
"A Smith's fracture is a reverse Colles fracture, usually extra-articular and volarly displaced." — Schwartz's Principles of Surgery, 11th Ed.
Smith fracture X-ray (volar displacement, AP and lateral views):

3. Barton Fracture — Intra-articular Rim Fractures with Subluxation
- Pattern: Intra-articular fracture; the fracture line exits through one cortical rim of the distal radius
- Two subtypes:
- Dorsal Barton: Fracture exits through the dorsal cortex → dorsal radiocarpal subluxation/dislocation
- Volar (Reverse) Barton: Fracture exits through the volar cortex → volar radiocarpal subluxation/dislocation
- Key feature: The carpus subluxates with the fracture fragment (distinguishes it from Colles/Smith)
"The Barton fracture refers to an intra-articular distal radius fracture extending through the dorsal cortex of the radius, often with dorsal subluxation or dislocation of the radiocarpal joint." — Rockwood and Green's Fractures in Adults, 10th Ed. (2025)
4. Chauffeur Fracture (Hutchinson Fracture) — Radial Styloid
- Mechanism: Originally from engine backfire cranking; now from direct trauma or transmitted force via the scaphoid
- Pattern: Isolated intra-articular fracture of the radial styloid
- Displacement: Variable; may cause occult carpal (scapholunate) disruption
- Key: Always assess for carpal ligament injury
Summary Comparison Table
| Fracture | Articular Involvement | Direction of Displacement | Carpus |
|---|---|---|---|
| Colles | Extra-articular | Dorsal | Follows fragment |
| Smith | Usually extra-articular | Volar | Follows fragment |
| Dorsal Barton | Intra-articular | Dorsal rim + dorsal sublux | Subluxates dorsally |
| Volar Barton | Intra-articular | Volar rim + volar sublux | Subluxates volarly |
| Chauffeur | Intra-articular (styloid) | Variable | Risk of SL injury |
Treatment by Displacement Direction
| Displacement | Treatment |
|---|---|
| Minimal | Non-operative, cast immobilization |
| Dorsal (Colles) | ORIF (volar locking plate) — now standard |
| Volar (Smith, volar Barton) | ORIF with volar plate |
| Intra-articular step-off >2 mm | Surgical fixation |
"ORIF (volar) for volarly displaced fractures (Smith and volar Barton); also become standard for dorsally displaced fractures (Colles)." — Miller's Review of Orthopaedics, 9th Ed.
Associated Injuries to Rule Out
- Scaphoid fracture
- Scapholunate (SL) ligament injury
- Ulnar styloid fracture / TFCC injury → risk of DRUJ instability
- Acute carpal tunnel syndrome (median nerve dysfunction — most common complication overall)
- EPL tendon rupture (attritional, near Lister's tubercle)
— Miller's Review of Orthopaedics, 9th Ed.; Rockwood and Green's, 10th Ed.
Distal radius fracture post op x ray findings
Finding Sources
Finding Sources
Searching Images
distal radius fracture postoperative xray volar locking plate ORIF fixation
Reading File
Searching Images
distal radius fracture ORIF volar plate screw prominence dorsal penetration complication xray
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have excellent textbook content and images. Here is the comprehensive answer:
Distal Radius Fracture — Postoperative X-Ray Findings
Standard Postoperative Views
The standard series is PA, lateral, and oblique. Additional views are critical after fixation:
- Sigmoid notch view (true AP of the distal radius): confirms overlap of the volar and dorsal lips of the sigmoid notch into a single "sigmoid stripe" — verifies true AP positioning and articular reduction
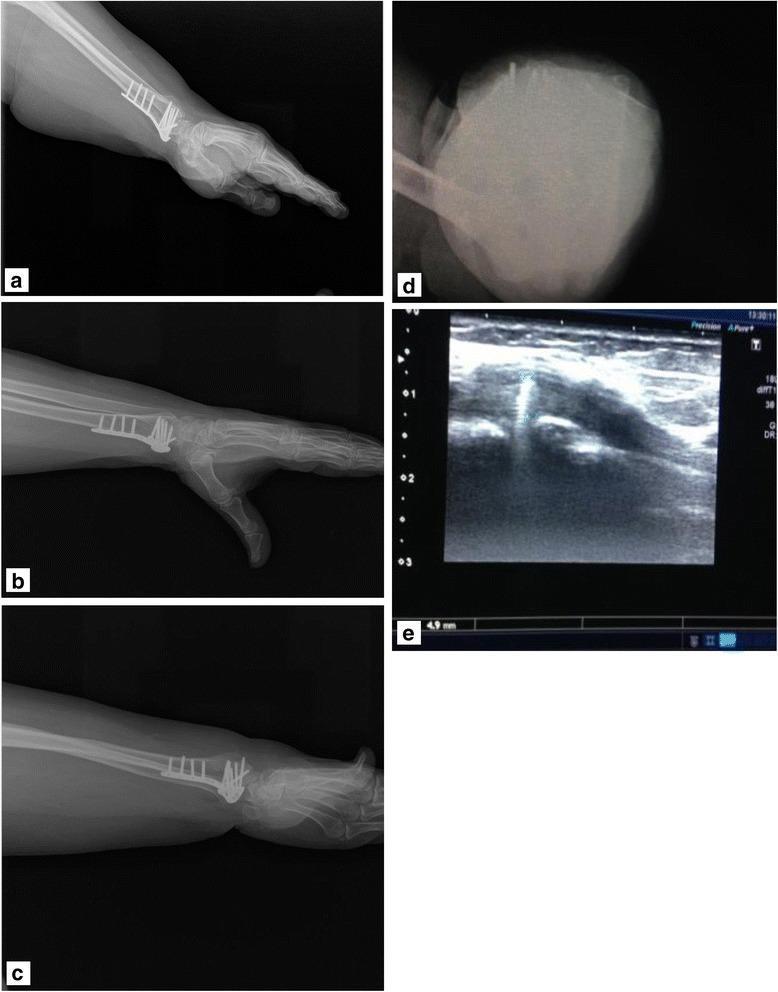
- Dorsal tangential view: wrist in maximal flexion with the dorsal cortex at a 15° incline to the X-ray beam — specifically designed to visualize screw tips relative to the dorsal cortex and detect dorsal screw penetration
- 45° pronation and 45° supination views: profile the 2nd and 4th extensor compartments respectively for subtle screw protrusion
"The dorsal tangential view is performed with the wrist in maximal flexion and the dorsal cortex of the radius at a 15-degree incline to the beam of the C-arm that allows visualization of the tip of the screws in relation to the dorsal cortex of the radius." — Rockwood and Green's Fractures in Adults, 10th Ed. (2025)
What to Assess on Postop X-Rays
1. Restoration of Radiographic Parameters
All measurements should be on a true lateral (radius and ulna superimposed) and true PA:
| Parameter | Normal Value | Acceptable Post-reduction |
|---|---|---|
| Volar tilt (lateral view) | 11–12° volar | ≤10° dorsal tilt (i.e., not >10° dorsal) |
| Radial height (PA view) | 11–12 mm | Shortening <3 mm |
| Radial inclination (PA view) | 22–23° | Maintained |
| Ulnar variance (PA view) | Neutral | Not significantly positive |
| Intra-articular step-off | 0 mm | <2 mm |
"Radial shortening less than 3 mm, dorsal tilt less than 10 degrees, intraarticular step-off less than 2 mm." — Miller's Review of Orthopaedics, 9th Ed.
Note on rotation: A 5° rotational change in forearm position causes a 1.6° change in measured volar tilt — always ensure true neutral forearm rotation before measuring.
2. Volar Locking Plate Position (Most Common Fixation)
The volar locking plate is placed via the FCR (modified Henry) approach. On postop X-rays, assess:
PA view:
- Plate positioned along the radial shaft proximally, with the distal row of screws targeting subchondral bone near the radiocarpal joint
- The distal locking screws should span the lunate facet radially
- Plate should not extend distal to the watershed line (risk of FPL rupture)
Lateral view:
- Plate lies against the volar cortex of the distal radius
- Distal screws directed toward the dorsal cortex — subchondral support without dorsal penetration
- Volar tilt should be restored (not dorsal tilt)
- Plate proximal to the watershed line of the volar radius
Volar locking plate — PA and lateral postop views:
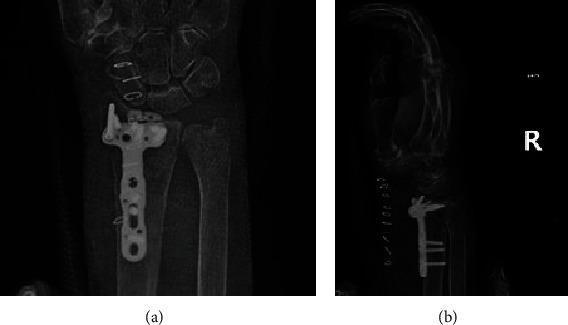
Postop PA view showing volar locking plate — variable-angle system:

3. Screw Position and Critical Findings
Key concern — dorsal screw penetration:
- The most common hardware complication on follow-up X-rays
- Screws protruding dorsal to the cortex → extensor tendon irritation or EPL rupture
- Standard lateral view may miss subtle penetration
- The dorsal tangential view (15° beam tilt with wrist flexed) and oblique views are used to detect this
Articular screw penetration:
- Screws must remain extra-articular — confirmed on sigmoid notch view and oblique views
- Any screw entering the radiocarpal joint space is a complication requiring revision
4. Loss of Reduction (Complication)
Seen in up to 30% of cases on follow-up. On X-rays look for:
- Re-displacement of the lunate facet (most clinically significant)
- Loss of volar tilt → dorsal angulation returning
- Increased ulnar variance (radial shortening)
- Intra-articular step-off reappearing

"PA and lateral radiographs of volar plate demonstrating loss of reduction of the lunate facet following inadequate fixation." — Rockwood and Green's, 10th Ed.
5. Carpal Alignment
On both PA and lateral views, assess the carpus:
- A line along the long axis of the capitate and a line along the radial shaft should overlap or intersect within the carpus
- If they intersect outside the carpus → carpal malalignment (compensatory carpal tilt or ligamentous disruption)
6. DRUJ Assessment
- On PA view: assess for ulnar styloid fracture and DRUJ congruency
- Kirschner wire (K-wire) may be seen across the DRUJ if instability was addressed intraoperatively
- Signs of DRUJ instability: coronal shift of distal fragment, >6 mm positive ulnar variance pre-reduction
7. Bone Healing on Serial X-Rays
| Timeframe | Expected X-ray Finding |
|---|---|
| Day 0–2 weeks | Hardware in place, fracture lines visible |
| 6 weeks | Early periosteal callus, fracture lines softening |
| 3 months | Bridging callus, fracture lines becoming less distinct |
| 6–12 months | Cortical remodeling, hardware may show osseointegration |
Summary: Postop X-Ray Checklist
| Item | What to Look For |
|---|---|
| Volar tilt | Restored to ~11°, not dorsal |
| Radial height | ≥11 mm, shortening <3 mm |
| Radial inclination | ~22°, symmetric to other side |
| Intra-articular step-off | <2 mm |
| Plate position | Proximal to watershed line, distal screws in subchondral bone |
| Screw tips (dorsal) | Not penetrating dorsal cortex — use tangential view |
| Screw tips (articular) | Extra-articular only |
| Lunate facet | Reduced, no step-off |
| Carpal alignment | Capitate–radius axis intersecting within carpus |
| DRUJ | Congruent, ulna not subluxed |
| Ulnar styloid / TFCC | Note if fractured; K-wire if stabilized |
— Rockwood and Green's Fractures in Adults, 10th Ed.; Miller's Review of Orthopaedics, 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.