Eagle syndrome
"Eagle syndrome" styloid process
Eagle Syndrome
Definition and History
- Scott-Brown's Otorhinolaryngology, Vol 2, p. 6843
- K.J. Lee's Essential Otolaryngology, p. 7844
Epidemiology
- An elongated styloid process is found incidentally in approximately 4% of the general population
- Only about 4% of those with an elongated styloid process actually develop symptoms
- More common in women; usually presents in the 4th-5th decade
Anatomy and Pathophysiology
- Compress the hypoglossal nerve
- Impinge on or irritate the carotid vessels (internal or external carotid artery) - this is the vascular variant
- Cause inflammatory changes at the insertion of the stylohyoid ligament
- Irritate cranial nerves V, VII, IX, or X passing nearby
Clinical Variants
| Variant | Mechanism | Key Features |
|---|---|---|
| Classic (stylohyoid) syndrome | Nerve/soft tissue irritation | Throat pain, foreign body sensation, dysphagia, otalgia |
| Carotid artery syndrome | Styloid compresses carotid artery/periarterial sympathetics | Neck/face pain on head turning, pre-syncopal episodes, TIA risk |
Clinical Features
- Dull, aching pharyngeal pain - typically in the tonsillar fossa
- Radiation to the ipsilateral ear (otalgia)
- Foreign body sensation in the throat (like a fish bone)
- Odynophagia (pain on swallowing)
- Pain on jaw movement or head turning
- Unilateral headaches and neck pain
- The elongated styloid process may be palpable in the tonsillar fossa
- Palpation of the tonsillar fossa may reproduce and aggravate symptoms
- Local anaesthetic injection into this area provides temporary relief (diagnostic and therapeutic)
Diagnostic Criteria (ICHD-based, per Cummings)
- Pain provoked or worsened by digital palpation of the stylohyoid ligament
- Pain provoked or worsened by head turning
- Pain significantly improved by local anaesthetic injection into the ligament, or by styloidectomy
- Pain is ipsilateral to the inflamed stylohyoid ligament
Note: The International Headache Society has previously described this syndrome as "not sufficiently demonstrated," which reflects the ongoing controversy around its diagnosis.
Imaging
- Orthopantomogram (OPG/panoramic X-ray): First-line, shows elongated styloid process
- CT scan (with 3D reconstruction): Preferred for accurate measurement, surgical planning, and to assess vascular proximity
- Normal styloid length: ~2.5 cm; >3 cm is often considered abnormal; >4 cm is generally accepted as "elongated"
Management
Conservative (Medical)
- NSAIDs - first-line
- Anticonvulsants (e.g., carbamazepine) - used for neuropathic pain component
- Antidepressants (amitriptyline)
- Corticosteroid + local anaesthetic injection into the tonsillar fossa - both diagnostic and therapeutic, but effects are temporary
- Results are variable; surgery is generally considered definitive
Surgical (Styloidectomy)
| Approach | Notes |
|---|---|
| Transoral (via tonsillar fossa) | Less invasive, avoids external scar, limited exposure |
| External transcervical | Better exposure and visualization, preferred for vascular variant |
Recent Evidence (2023-2024)
| Study | Finding |
|---|---|
| Hassani et al., 2024 - Systematic Review/Meta-Analysis (PMID 38948209) | Neurological phenotypes in Eagle syndrome; meta-analyzed treatment outcomes |
| Campisi et al., 2024 (PMID 38290994) | Transoral robotic styloidectomy is feasible with good outcomes |
| Tadjer & Béjot, 2024 (PMID 39440251) | Vascular variant carries significant stroke/TIA risk; warrants early surgical intervention |
| Pagano et al., 2023 (PMID 38053694) | Updated comprehensive review of pathophysiology and management |
Key Points Summary
- Eagle syndrome = elongated styloid process (>4 cm) or calcified stylohyoid ligament
- Affects ~0.16% of population (4% have elongation, 4% of those are symptomatic)
- Classic: throat/ear pain, foreign body sensation, odynophagia
- Vascular variant: carotid compression - can cause stroke/TIA
- Diagnose with OPG or CT; palpation in tonsillar fossa reproduces pain
- Conservative treatment (NSAIDs, carbamazepine, steroid injections) offers partial relief
- Definitive treatment: styloidectomy (transoral or transcervical)
Oro antral fistula
"oroantral fistula" treatment closure
oroantral fistula classification causes repair techniques buccal flap palatal flap
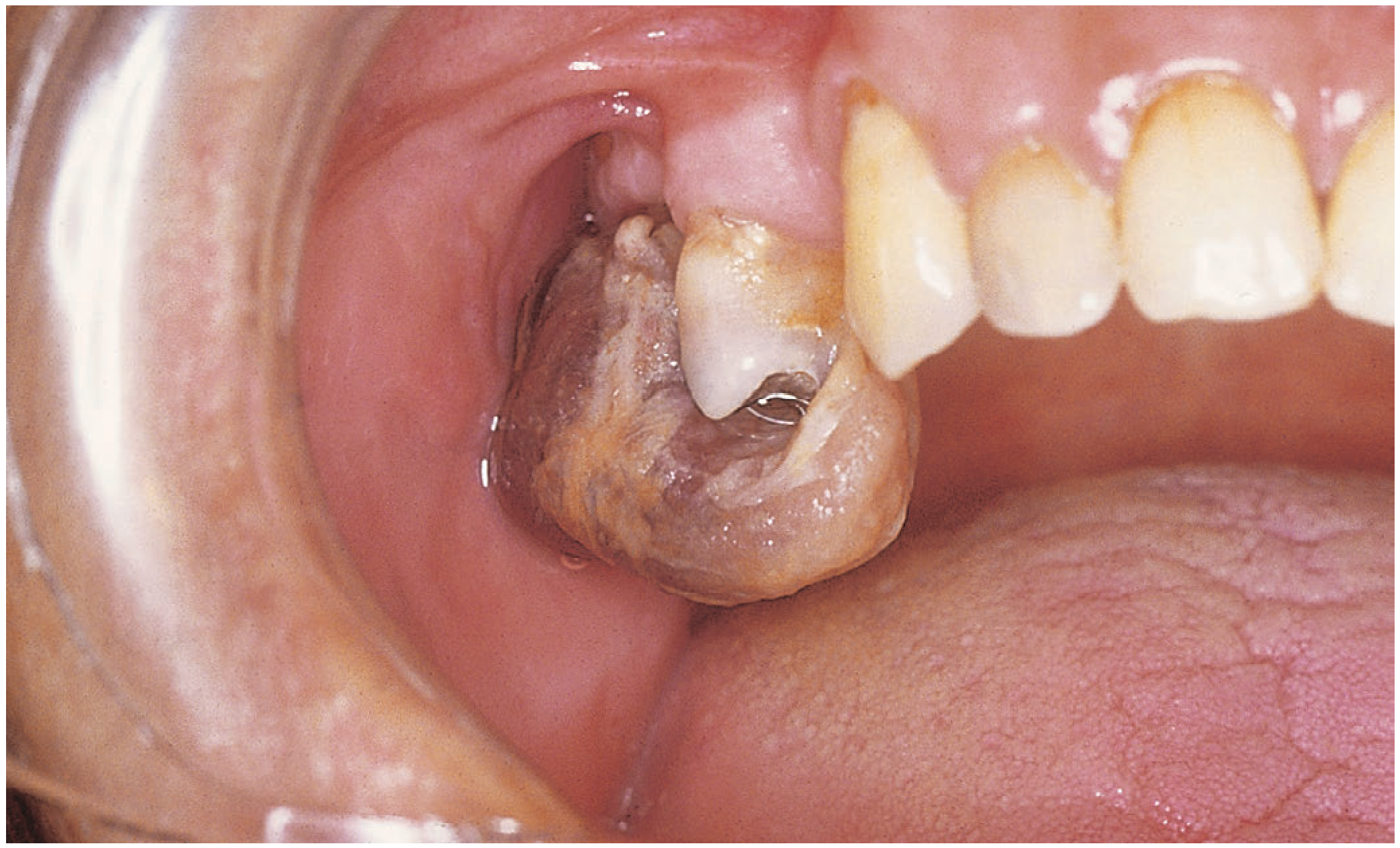
Oro-Antral Fistula (OAF)
Definition
Terminology: An acute, fresh opening is called an oro-antral communication (OAC); once epithelialized and chronic, it becomes an oro-antral fistula (OAF).
Anatomy - Why It Happens
Aetiology / Causes
| Category | Specific Causes |
|---|---|
| Iatrogenic (most common) | Tooth extraction (upper molars/premolars), dental implant failure, apicectomy, endodontic overfill |
| Infective | Periapical abscess, periodontitis, osteomyelitis of maxilla, actinomycosis |
| Pathological | Maxillary cyst (dentigerous, radicular) erosion into sinus, tumours (including maxillary antral carcinoma - important cause of OAF that must not be missed) |
| Traumatic | Facial fractures (Le Fort I), gunshot wounds |
| Iatrogenic - ENT | Caldwell-Luc procedure, sinus surgery |
| Radiation | Osteoradionecrosis |
Clinical Features
- Nasal regurgitation of fluids - pathognomonic; fluid taken orally passes into the nose
- Nasal voice (hyper-nasal speech)
- Unpleasant taste or smell (due to sinus secretions entering the mouth)
- Halitosis
- Pain/pressure over the cheek (associated sinusitis)
- Sense of air passing between mouth and nose on blowing
- Unilateral mucopurulent nasal discharge (odontogenic sinusitis)
- Reduced sense of smell
- Visible opening in the alveolar socket or mucosa
- Nose-blowing test (Valsalva): air passes from mouth into nose through the fistula
- Probe test: a blunt probe passes freely from the oral cavity into the sinus
- CT: loss of sinus floor continuity ± mucosal thickening or opacification of maxillary sinus
Investigations
- Clinical exam + probe test - identifies communication
- OPG (Orthopantomogram) - shows bone loss, relation of roots to sinus floor
- CT scan (fine-cut coronal) - gold standard for imaging; shows sinus floor defect, mucosal thickening, bony involvement; rules out malignancy
- Biopsy - mandatory if malignancy is suspected (carcinoma can present as OAF)
Classification (by size)
| Size | Management |
|---|---|
| Small (<5 mm) | May close spontaneously with conservative measures |
| Medium (5-10 mm) | Surgical closure usually required |
| Large (>10 mm) | Definitive surgical repair mandatory |
Management
Step 1: Manage Associated Sinusitis
- Antibiotics - broad-spectrum (amoxicillin-clavulanate; metronidazole for anaerobic coverage)
- Nasal decongestants - to improve ostial drainage
- Antral washout or FESS (functional endoscopic sinus surgery) if established chronic sinusitis is present
- Failure to treat sinusitis leads to flap failure
Step 2: Surgical Closure
A. Buccal Advancement Flap (Rehrmann Flap) - Most Common
- A trapezoidal mucoperiosteal flap is raised from the buccal (cheek) side
- Periosteum is incised at the base to allow advancement and tension-free closure
- Fistula edges are freshened, and the flap is advanced and sutured to the palatal mucosa
- Indications: Small to medium OAFs in lateral/anterior position
- Disadvantage: Reduces vestibular depth (may need vestibuloplasty later)
- Success rate: ~90%
B. Buccal Fat Pad (BFP) Flap - Increasingly Preferred
- The buccal fat pad (Bichat's fat pad) is mobilized through a small incision in the upper buccal sulcus
- Fat is laid into the defect and sutured to the margins; epithelializes in ~3-4 weeks
- Indications: Defects in the central/posterior alveolar crest; OAF >5 mm
- Advantages: Rich blood supply, abundant tissue, no donor site morbidity, does not reduce vestibular depth
- Success rate: ~98% (highest of all techniques)
- Can be combined with buccal advancement flap for large defects (double-layer closure)
C. Palatal Rotation-Advancement Flap
- A posteriorly-based palatal mucoperiosteal flap is rotated to cover the defect
- Based on the greater palatine artery
- Indications: Defects in the premolar region; posterior/palatal OAF location; when buccal flap is unsuitable
- Disadvantages: Leaves a raw donor area on hard palate (heals by secondary intention); technically demanding
- Success rate: ~86%
D. Other / Distant Flaps (for large/complex defects)
- Tongue flap (anteriorly or posteriorly based)
- Nasolabial flap
- Temporalis muscle flap
- Free flaps (radial forearm, anterolateral thigh) - for post-oncologic large defects
- Zygomatic implants - for post-maxillectomy oroantral defects
- Buccal flap: 40.1% of cases, 89.8% success
- Buccal fat pad: 28.6% of cases, 98.3% success
- Palatal flap: 19% of cases, 85.7% success
Flap Selection Algorithm
OAF identified
│
├── Size <5 mm → Conservative (gelatin sponge, suture, observe)
│
├── Size 5-10 mm
│ ├── Lateral/anterior location → Buccal advancement (Rehrmann) flap
│ ├── Central alveolar crest → Buccal fat pad flap
│ └── Palatal side / premolar → Palatal rotation flap
│
└── Size >10 mm
└── Buccal fat pad ± buccal advancement (double layer)
or distant/free flap for very large defects
Post-Operative Care
- Antral precautions: Avoid nose blowing, sneezing with closed mouth, use of straws, smoking for 2-4 weeks
- Antibiotics + nasal decongestants for 1-2 weeks
- Soft diet
- Follow-up to confirm closure at 3 months
Complications of Untreated OAF
- Chronic odontogenic sinusitis - most common; unilateral, anaerobic-predominant
- Antral polyp formation
- Ascending spread to other sinuses or orbit (rare)
- Persistent halitosis and social disability
Important: Always Exclude Malignancy
Recent Evidence
| Study | Finding |
|---|---|
| Alomari et al., 2025 (PMID 41091334) | Clinical decision-making algorithm for OAF management - comprehensive guide |
| Kheiri et al., 2025 (PMID 40301851) | Systematic review of dental implant outcomes at OAC sites |
| Kwon et al., 2020 (PMC7049762) | Review of local flap techniques: BFP has highest success rate for defects >5 mm |
Key Points Summary
- OAC = acute, non-epithelialized; OAF = chronic, epithelialized communication
- Most common cause: upper molar extraction (1st molar most at risk)
- Classic symptom: nasal regurgitation of fluids + nasal voice
- Diagnosis: clinical probe test + CT scan; always biopsy to exclude carcinoma
- Small (<5 mm): may close spontaneously
- Surgical repair: buccal fat pad flap has the highest success rate (~98%); choice guided by defect size and location
- Always treat associated sinusitis before/during repair
Radioactive thyroid scanning
"thyroid scintigraphy" radionuclide
Radioactive Thyroid Scanning (Thyroid Scintigraphy)
Overview
Key distinction: Thyroid scintigraphy (the image of the gland) is different from but adjunctive to the radioactive iodine uptake (RAIU) test (which simply measures the fraction of dose taken up at 24 hours as a number).
Radiotracers Used
| Radiotracer | Type | Half-life | Mechanism | Notes |
|---|---|---|---|---|
| Tc-99m pertechnetate | Gamma emitter | 6 hours | Trapped by thyroid (transport only, NOT organified) | Most commonly used; scan within 20-30 min of IV injection; less radiation; cheaper; one-day test; does NOT penetrate sternum - cannot assess substernal goiter |
| I-123 | Gamma/beta emitter | 13.2 hours | Trapped AND organified (full iodine pathway) | Oral administration; images at 4h and 24h; tests both transport and organification; more expensive, 2-day test; preferred for accurate RAIU measurement |
| I-131 | Beta + gamma emitter | ~8 days | Same as I-123 | Longer half-life; higher radiation dose; used for post-thyroidectomy remnant ablation and differentiated thyroid cancer staging; diagnostic dose 1-5 mCi; therapeutic dose 30-150 mCi |
- Cummings Otolaryngology, p. 3649; Mulholland & Greenfield's Surgery, p. 4030
Normal Scan Appearance
Nodule Classification
| Category | Definition | Malignancy Risk |
|---|---|---|
| Hot nodule (hyperfunctioning) | Uptake greater than surrounding thyroid tissue - autonomous function suppresses the rest of the gland | Very low (~4%); rarely malignant |
| Warm / isofunctioning nodule | Uptake equal to surrounding tissue | Low |
| Cold nodule (hypofunctioning/non-functioning) | Uptake less than surrounding thyroid tissue (photopenic area) | ~10-15% malignancy risk |
- Cummings Otolaryngology, p. 3647
- Goldman-Cecil Medicine, p. 3322
Scan Patterns in Thyrotoxicosis
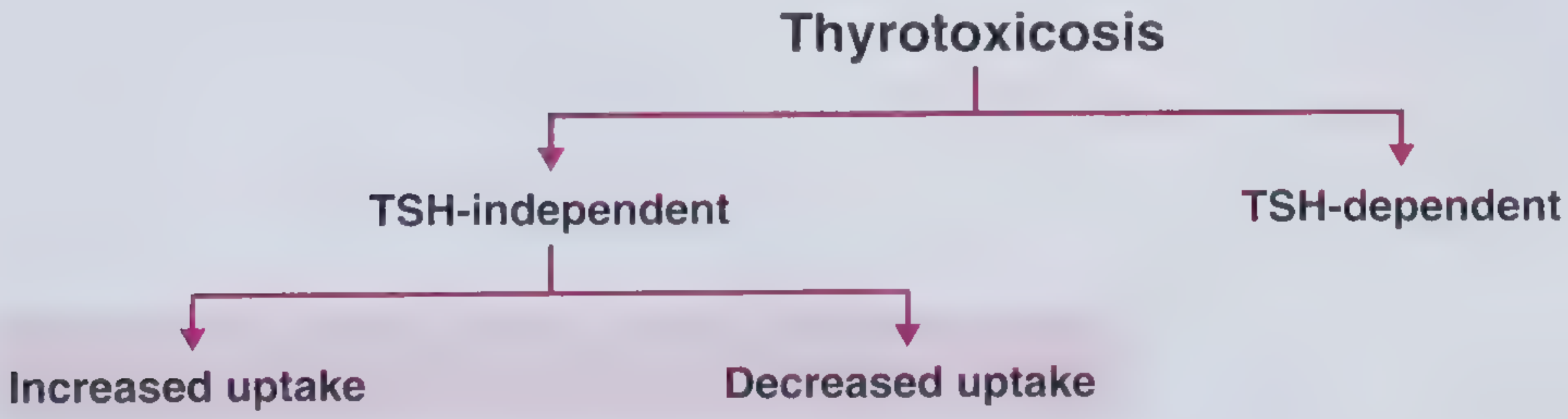
- True hyperthyroidism (thyroid overproducing hormone) = INCREASED RAI uptake
- Thyrotoxicosis without hyperthyroidism (hormone released from destruction) = DECREASED RAI uptake
Pattern 1: Diffuse Increased Uptake

Pattern 2: Focal Increased Uptake (Single "Hot" Area)

Pattern 3: Multiple "Hot" Foci
Pattern 4: Absent / Markedly Reduced Uptake
Summary Table: Scan Patterns in Common Conditions
| Condition | RAIU | Scan Pattern |
|---|---|---|
| Graves' disease | Increased | Diffuse uniform uptake, enlarged gland |
| Toxic adenoma | Increased | Single hot nodule; rest of gland suppressed |
| Toxic multinodular goiter | Increased | Multiple focal hot areas |
| Subacute thyroiditis | Decreased/absent | Near-zero uptake throughout |
| Silent/post-partum thyroiditis | Decreased/absent | Near-zero uptake |
| Thyrotoxicosis factitia | Decreased/absent | Near-zero uptake |
| Hashitoxicosis | Normal/increased (variable) | Variable (exception to the rule) |
| Struma ovarii | Decreased in neck | Uptake in pelvis |
| Post-thyroidectomy residual | Variable | Residual uptake in neck/possible metastases |
Indications for Thyroid Scanning
- Hyperthyroid patient with thyroid nodule - to distinguish toxic nodule from Graves' disease with co-existing cold nodule (Marine-Lenhart syndrome)
- Thyrotoxicosis workup - to differentiate causes (see table above)
- After indeterminate FNA cytology - an I-123 scan should be considered; if a concordant autonomously functioning nodule is found, surgery may be deferred
- Post-thyroidectomy differentiated thyroid cancer - I-131 whole-body scan for remnant ablation and detection of metastases
- Suspected substernal/ectopic thyroid - I-123 or I-131 (Tc-99m cannot penetrate sternum)
- Congenital hypothyroidism - to identify thyroid aplasia, ectopia, or dyshormonogenesis in neonates
When Thyroid Scanning is NOT Indicated / Limitations
- Routine evaluation of a thyroid nodule in a euthyroid patient: NOT recommended. FNA (fine-needle aspiration biopsy) guided by ultrasound has largely replaced scintigraphy here, as 95% of nodules are cold and the cold nodule classification is not specific enough.
- Pregnancy and breastfeeding: I-131 is absolutely contraindicated. I-123 is relatively contraindicated. Tc-99m pertechnetate is excreted in breast milk; breastfeeding should be suspended for 24 hours.
- Cannot assess anatomy (size, margins, vascularity) - use ultrasound for that
- Cold lesions may be obscured by overlying normal thyroid tissue; oblique views help
I-131 in Differentiated Thyroid Cancer
- Post-thyroidectomy, I-131 is used for remnant ablation (30-100 mCi) to destroy residual normal thyroid tissue and facilitate future serum thyroglobulin monitoring
- Diagnostic whole-body scan with a low dose (1-5 mCi) at 6-12 months post-ablation to detect functioning metastases
- Therapeutic doses (100-200 mCi or more) for known metastatic disease
- Requires TSH stimulation (either thyroid hormone withdrawal OR recombinant TSH/Thyrogen) to maximize I-131 uptake
- Poorly differentiated thyroid cancers and medullary carcinoma do not take up iodine - FDG-PET is used instead
Key Points
- Tc-99m pertechnetate: one-day test, low radiation, tests iodine trapping only; confirm hot nodules with I-123
- I-123: two-day test, tests transport + organification, preferred for RAIU measurement; best for scintigraphy
- I-131: therapeutic isotope; diagnostic whole-body scanning for differentiated thyroid cancer
- Hot nodules: rarely malignant (~4%); no FNA needed
- Cold nodules: 10-15% malignancy risk; FNA warranted if meets criteria
- 95% of all scanned nodules are cold
- Most useful clinical role today: differentiating causes of thyrotoxicosis and post-thyroidectomy cancer management
- Scan NOT needed for routine nodule evaluation in euthyroid patients - ultrasound + FNA is preferred
Powered instruments in ENT
"powered instrumentation" OR "microdebrider" ENT sinus surgery
Powered Instruments in ENT
Overview
- Microdebrider (powered shaver system) - used in rhinology, laryngology, and head & neck
- Powered drills (high-speed drills with burrs) - used in otology, skull base, and sinonasal surgery
- Other powered instruments - coblation, ultrasonic aspirator, etc.
1. The Microdebrider (Powered Shaver System)
Mechanism of Action
- A powered handpiece connected to a console
- A disposable hollow rotating blade at the tip
- Integrated suction that aspirates tissue into the port as the blade rotates
- Irrigation system in some configurations
Applications in Rhinology (FESS)
| Procedure | How microdebrider is used |
|---|---|
| Uncinectomy | Initial cut/removal of uncinate process |
| Anterior ethmoidectomy | Removal of bulla ethmoidalis and anterior ethmoid cells |
| Posterior ethmoidectomy | "A microdebrider, Kerrison's punch or through-biting instruments can be used to remove the partitions between the posterior ethmoid cells" - Scott-Brown's, Vol 1, p. 5217 |
| Nasal polypectomy | Rapid debulking of polyp tissue |
| Frontal recess dissection | Angled (40-90°) microdebrider blades used to remove fronto-ethmoidal cells; curved blades for supraorbital ethmoid cells |
| Maxillary antrostomy | Enlargement of the natural ostium |
| Sphenoidotomy | Enlargement of sphenoid ostium |
- Simultaneous cutting and suctioning keeps the surgical field clear
- Precise, controlled tissue removal
- Reduces mucosal trauma and bleeding
- Faster dissection
- Reduces risk of polyp/tissue fragment dropping into the airway
Applications in Inferior Turbinate Surgery
- A submucosal tunnel is created via a small anterior incision
- The erectile tissue is partially resected from the medial and inferior turbinate
- Post-operative nasal packing is not necessary
- The microdebrider can be controlled to preserve all overlying mucosa - a key advantage
Applications in Adenoidectomy
- 20% faster than traditional curettage technique (RCT evidence)
- Precise removal under visual control; avoids the blind nature of traditional curette adenoidectomy
- Lower risk of velopharyngeal insufficiency when partial adenoidectomy is performed
- Reduced risk of inadvertent eustachian tube orifice trauma
- Disadvantage: High unit cost (microdebrider blade is expensive and single-use)
Applications in Tonsillectomy / Intracapsular Tonsillectomy
- The tonsil is debulked inside the capsule, leaving the capsule intact
- Preserves the fibrous capsule as a barrier against secondary haemorrhage
- Lower post-operative pain and faster return to normal activities vs. electrocautery
- Lower bleeding rates
- Risk of tonsil regrowth - especially in younger children
Applications in Laryngology
- No thermal trauma to surrounding tissue
- No laser plume - eliminates risk of viral aerosol transmission to operating room staff
- No risk of airway fire
- Shorter operative times
- Less post-operative pain
- Precise removal with minimal mucosal damage
- Round window (skimmer) blade - for soft, bulky lesions (papillomas, tracheal papilloma)
- Subglottic/tracheal blade - for fibrous scar (subglottic/tracheal stenosis)
- Smaller skimmer laryngeal blade - for true vocal fold lesions
- Internal laryngoceles
- Tumour debulking
- Removal of PTFE granulomas
- Subglottic and tracheal stenosis
- Tracheostomal granulation tissue
- Laryngeal cysts
- Reinke's oedema
2. Powered Drills in Otology and Skull Base Surgery
Types of Burrs
| Burr Type | Properties | Uses |
|---|---|---|
| Cutting burr | Serrated/fluted; removes bone rapidly | Initial cortical drilling, large area bone removal; zygomatic root and attic opening |
| Diamond burr | Smooth surface; safer near vital structures; generates heat (requires continuous irrigation) | Near facial nerve, dura, sigmoid sinus, ossicular chain, cochlea; haemostasis in bone |
Applications in Ear Surgery
| Procedure | Role of Powered Drill |
|---|---|
| Cortical/simple mastoidectomy | Cortical bone removal, opening mastoid air cell system |
| Canal wall up mastoidectomy | Attic dissection, posterior tympanomeatal flap |
| Canal wall down (radical/modified) mastoidectomy | Lowering facial ridge, meatoplasty |
| Cochlear implant surgery | Posterior tympanotomy, cochleostomy |
| Stapedectomy/stapedotomy | Oval window drilling (small diamond burr) |
| Exostoses removal | "Cases of severe exostoses may require meticulous surgical removal via a postaural approach using a high-speed drill." - Scott-Brown's, Vol 2, p. 9598 |
| Facial nerve decompression | Diamond burr to skeletonize fallopian canal |
| Cholesteatoma dissection | Bone removal to access and exteriorize disease |
Applications in Rhinology and Skull Base
- Endoscopic skull base surgery: High-speed drill for removal of bony partitions, sella turcica, clivus, orbital apex
- Frontal sinus trephine / drill-out (Lothrop procedure): Powered drill for bony frontal floor removal
- Orbital decompression: Orbital apex decompression using high-speed drill for optic neuropathy in compressive thyroid eye disease
- Sinonasal tumour surgery: Bone removal for access and resection margins
3. Other Powered Instruments
| Instrument | Mechanism | ENT Use |
|---|---|---|
| Coblation (bipolar RF) | Bipolar radiofrequency creates cold plasma field (85°C) - dissolves tissue then induces fibrosis | Tonsillotomy/tonsillectomy, turbinate reduction, adenoidectomy, RRP |
| Endoscopic ultrasonic aspirator (CUSA) | Ultrasonic fragmentation + irrigation + suction | Skull base tumour removal (endoscopic) |
| Powered laryngeal shaver | Same principle as microdebrider, adapted for larynx | RRP, laryngeal tumour debulking |
Advantages of Powered Instruments - Summary
| Feature | Benefit |
|---|---|
| Simultaneous cutting + suction | Clear operative field; faster surgery |
| Controlled tissue removal | Precise; preserves adjacent structures |
| No thermal spread (microdebrider) | Less collateral mucosal damage vs. diathermy/laser |
| No airway fire risk (vs. laser) | Safer in oxygen-rich airway |
| No laser plume | Protects OR staff from viral/tumour aerosol |
| Oscillating blade control | Adjustable rpm for different tissue types |
| Angled/curved blades available | Access to difficult anatomical sites (frontal recess, subglottis) |
Disadvantages
- High unit cost - blades are single-use and expensive (limits use as sole technique for adenoidectomy)
- Learning curve - especially for angled blades
- Suction removes all tissue - no specimen for histology in some techniques (important in tonsillotomy)
- Risk of mucosal stripping if not used carefully - can cause adhesions, stenosis (especially in frontal recess)
- Relative contraindication near vascular structures (laryngeal microdebrider)
- Drill heat generation (diamond burr) - requires continuous suction-irrigation to prevent thermal bone/nerve injury
Key Points Summary
- Microdebrider = cutting + suction in one instrument; gold standard for laryngeal papillomatosis (RRP) and widely used in FESS and turbinate surgery
- In FESS: straight and angled (40-90°) blades for different sinus regions; circumferential frontal recess injury must be avoided
- In adenoidectomy: 20% faster than curette; preserves direct vision
- Intracapsular tonsillectomy with microdebrider: less pain, faster recovery, but risk of regrowth
- Drill in otology: cutting burr for rapid cortical bone removal; diamond burr near vital structures (facial nerve, ossicles, dura, sigmoid)
- Diamond burr also achieves haemostasis from mastoid bone marrow
- Coblation: alternative powered technique operating at lower temperature (85°C), less thermal spread than diathermy
Intra tympanic therapy
"intratympanic" therapy inner ear drug delivery
"intratympanic steroids" sudden sensorineural hearing loss
Intratympanic (IT) Therapy
Concept and Rationale
Anatomical Basis: The Round Window Membrane
- It is a three-layered, dynamic biological structure capable of both active and passive transport
- The three layers: outer epithelium (middle ear side), middle fibrous connective tissue layer, inner epithelium (perilymph side)
- It is semipermeable - allows selective passage based on molecular size, charge, and lipid solubility
- Method of delivery (injection vs. sustained release vs. catheter)
- Permeability of the substance applied (lipid-soluble agents penetrate better)
- Rate of clearance from the perilymph (Eustachian tube drainage)
- Adhesions over the RWM - can significantly reduce drug delivery; some surgeons advocate microscopic removal of adhesions (e.g., round window plug) before therapy
- Patient head position after injection - affects pooling near the RWM
Drugs Used in Intratympanic Therapy
| Drug | Mechanism | Primary Indication |
|---|---|---|
| Dexamethasone | Anti-inflammatory, immunomodulatory | SSNHL (salvage), Meniere's disease (vertigo control) |
| Methylprednisolone | Anti-inflammatory, immunomodulatory | SSNHL (primary or salvage) |
| Gentamicin | Vestibulotoxic aminoglycoside | Meniere's disease (vertigo ablation) |
| Streptomycin | Vestibulotoxic (historical) | Meniere's (now rarely used due to cochleotoxicity) |
IT Technique (Procedure)
Steps:
- Patient reclined with head turned ~45° to the treated side (to fill the inferior middle ear near the RWM)
- Topical anaesthesia applied to the TM (e.g., EMLA cream, phenol, or iontophoresis)
- Injection with a fine-gauge needle (25-27 gauge) through the anteroinferior or posteroinferior quadrant of the TM
- Drug is slowly instilled into the middle ear (~0.3-0.5 mL)
- A separate ventilation hole is sometimes made in the anterosuperior quadrant for pressure equalization as the drug is injected
- Patient asked to remain still with head tilted for 20-30 minutes to maximize drug contact with the RWM; should avoid swallowing (closes Eustachian tube temporarily)
- Patient instructed not to blow the nose immediately after
Delivery Variants:
- Single injection - most common outpatient approach
- Repeated injections - multiple sessions (e.g., 3-4 injections over 2 weeks for SSNHL)
- Tympanostomy tube-based delivery - drug instilled through an existing grommet (no injection needed; can be done by patient at home)
- Silverstein MicroWick - a thin wick placed through a myringotomy tube to the RWM niche for continuous drug delivery
- Microcatheter / round window catheter - placed surgically at the RWM for continuous or controlled drug release; used in trials for severe SSNHL
- Sustained-release formulations (gel-based, e.g., hyaluronic acid or poloxamer gels) - under development; prolongs contact time at the RWM
1. IT Steroids
For Sudden Sensorineural Hearing Loss (SSNHL)
- Primary treatment - when systemic steroids are contraindicated (diabetes, hypertension, peptic ulcer, immunocompromised patients)
- Salvage/rescue treatment - when SSNHL has not responded to initial oral/IV steroid course (most common indication; administered 2-6 weeks after onset)
- RCT evidence shows IT methylprednisolone improves hearing in patients who failed oral steroids for SSNHL (Cummings, p. 70)
- "Strong data support the use of IT steroids as salvage therapy after failure to respond to oral steroids. Results are best when steroids are applied as early as possible." - Cummings, p. 4905
- A 2025 systematic review (PMID 40734818) confirms IT steroids as the leading salvage strategy for refractory SSNHL
- Reduces endocochlear inflammation
- Upregulates Na-K-ATPase in stria vascularis (maintains endocochlear potential)
- Immunomodulation if autoimmune aetiology
- Possible anti-apoptotic effects on cochlear hair cells
For Meniere's Disease (Vertigo Control)
- Small RCT: 82% complete resolution of vertigo with dexamethasone vs. 57% with saline (Cummings, p. 144)
- Scott-Brown's (recommendation grade A): "Repetitive intratympanic injections of dexamethasone enable substantial and long-term vertigo control in 80% of refractory cases without significant hearing loss." - Scott-Brown's, Vol 2, p. 6344
2. IT Gentamicin
Mechanism
Indications
- Meniere's disease - refractory to medical therapy AND after failure of IT dexamethasone
- End-stage / Tumarkin crises (drop attacks) - even in patients with poor hearing, as hearing preservation is less of a concern
- Recommendation grade A (Scott-Brown's): Used when IT dexamethasone has failed
Protocols (Titration vs. Fixed)
| Protocol | Approach | Notes |
|---|---|---|
| Fixed-dose | 1 injection/week × 4 weeks | Simple; higher cumulative dose; higher hearing loss risk |
| Titration (as-needed) | Single injections given at intervals until vertigo controlled | Lower total dose; preferred by most to minimize HL risk |
| Low-dose | Single or few injections, wait for response | Preserves more hearing; may need repeat |
Efficacy
- Meta-analysis (Huon et al., 2012): 87.5% Class A and B vertigo control
- RCT (intratympanic gentamicin vs. dexamethasone): 93.5% vs. 61% substantial vertigo control at 2-year follow-up (Scott-Brown's, p. 6334)
- Effective for drop attacks (Tumarkin crises): IT gentamicin has demonstrated effectiveness (Scott-Brown's, p. 6341)
Risks
- Sensorineural hearing loss: 0-38.7% across series (highly variable; dependent on dose and protocol)
- Vestibular hypofunction / oscillopsia post-ablation
- Imbalance - patient may develop chronic disequilibrium
Decision Algorithm for Meniere's Disease
Meniere's disease - medical treatment failure
│
▼
IT Dexamethasone (Grade A recommendation)
→ 80% vertigo control; no significant HL risk
│
If refractory
▼
IT Gentamicin (Grade A recommendation) - "as-needed" titration
→ 87-93% vertigo control; risk of SNHL
│
If bilateral or further failure
▼
Surgical options: Endolymphatic sac surgery / Vestibular nerve section
Complications of IT Injection Procedure
| Complication | Notes |
|---|---|
| Persistent TM perforation | Usually heals spontaneously; rare persistent perforation (<1%) |
| Dizziness/vertigo | Transient; especially if cold solution used |
| Tinnitus exacerbation | Temporary |
| Pain | Usually mild with topical anaesthesia |
| Infection / otitis media | Rare; sterile technique important |
| Drug-specific: SNHL | With IT gentamicin (see above) |
| Round window membrane adhesions | May impair drug delivery; identifiable on otoendoscopy |
Emerging and Future Directions
- Sustained-release IT formulations (gel-based dexamethasone, OTO-104/OTO-313) - prolonged drug contact at RWM; in clinical trials
- Nano-formulations - nanoparticles for targeted cochlear drug delivery
- Gene therapy via IT route - delivery of vectors (AAV) to cochlea via round window; neurotrophins and hair cell regeneration genes
- IT aminoglycosides for tinnitus - investigational
- IT gels: A 2024 scoping review (PMID 38308599) documents growing clinical trial data for intratympanic gel formulations
Key Points Summary
- IT therapy bypasses the blood-labyrinth barrier; RWM is the primary drug entry route
- RWM is three-layered, semipermeable; adhesions over it reduce drug entry
- IT steroids: first-line for SSNHL in contraindications to systemic steroids; gold standard salvage for SSNHL after failed systemic steroids; dexamethasone for Meniere's vertigo (80% control, no HL risk)
- IT gentamicin: selective vestibulotoxic; 87-93% vertigo control in Meniere's; used after IT dexamethasone failure; risk of SNHL; titration protocol preferred over fixed dosing
- Complete caloric ablation is NOT the endpoint - associated with high SNHL rates
- IT dexamethasone is preferred when hearing is still useful; IT gentamicin for end-stage or refractory cases
- Drug delivery methods: single injection, grommet instillation, MicroWick, catheter, sustained-release gels
Direct laryngoscopy
"direct laryngoscopy" technique indications complications
Direct Laryngoscopy (DL) / Microlaryngoscopy
Definition and Terminology
- Direct laryngoscopy (DL): Visualization of the larynx by direct line-of-sight using a rigid laryngoscope, with the patient's oral, pharyngeal, and laryngeal axes aligned. Can be performed under general anaesthesia (operative/suspension DL) or with topical anaesthesia.
- Microlaryngoscopy (MLB / suspension laryngoscopy): Direct laryngoscopy under general anaesthesia with the laryngoscope suspended on a chest support, leaving both hands of the surgeon free to use microsurgical instruments or an operating microscope.
- Panendoscopy: Combined direct laryngoscopy + rigid oesophagoscopy + bronchoscopy performed under the same anaesthetic.

Historical Development
- Chevalier Jackson (1865-1958): Father of endoscopy; developed the tubular laryngoscope and systematic approach to laryngoscopy
- Kleinsasser (1968): Developed the wide-bore suspension laryngoscope and microlaryngoscopic technique
- Jako and Strong (1972): First described CO₂ laser surgery of the larynx using microlaryngoscopy
- Dedo: Developed the Dedo laryngoscope widely used for suspension microlaryngoscopy
Types of Laryngoscopes
For Intubation (Anaesthesia)
| Blade | Shape | Mechanism | Use |
|---|---|---|---|
| Macintosh (curved) | Curved | Tip placed in vallecula; indirectly lifts epiglottis by traction on hyoepiglottic ligament | Standard adult intubation |
| Miller (straight) | Straight | Tip placed posterior to epiglottis; directly lifts it | Children; anterior larynx; difficult airways; paraglossal technique |
| McCoy | Hinged tip | Tip flexes to improve view | Difficult airways |
For ENT/Operative Laryngoscopy
| Laryngoscope | Features | Use |
|---|---|---|
| Kleinsasser | Wide bore; oval cross-section; slotted design | Standard suspension microlaryngoscopy |
| Dedo | Long, slender, anterior commissure type | Suspension MLB; good for anterior commissure |
| Hollinger (anterior commissure) | Narrow neck with distal anterior flare | Anterior commissure lesions; difficult larynges |
| Lindholm | Wider bore; good for instruments | Subglottic and tracheal access |
| Benjamin-Lindholm | Paediatric variant | Paediatric laryngoscopy |
| Ossoff-Karlan | Slotted; designed for laser use | CO₂ laser microlaryngoscopy |
Patient Positioning
"Sniffing Position" (Jackson Position)
- Neck flexed on the thorax (pillow under occiput, ~8-10 cm)
- Head extended at the atlanto-occipital joint
- This aligns the three axes: oral axis, pharyngeal axis, and laryngeal axis into one straight line of sight
BURP Manoeuvre
Cormack-Lehane Grading of Laryngoscopic View
| Grade | View | Clinical Significance |
|---|---|---|
| Grade I | Entire glottis (vocal cords) visible | Easy intubation |
| Grade IIA | Partial view of glottis | Usually easy |
| Grade IIB | Arytenoids or posterior vocal cords only visible | Increased difficulty |
| Grade III | Epiglottis only visible; no glottic structures seen | Difficult intubation |
| Grade IV | No laryngeal structures visible (not even epiglottis) | Failed intubation; requires alternative |
Anaesthesia for Operative Microlaryngoscopy
Goals (Morgan & Mikhail, p. 776)
- Immobile surgical field - profound neuromuscular blockade
- Adequate masseter muscle relaxation for laryngoscope introduction
- Adequate oxygenation and ventilation
- Cardiovascular stability despite rapidly varying stimulation levels
Premedication
- Glycopyrrolate (0.2-0.3 mg IM): Minimises secretions to facilitate airway visualization; given 1 hour before surgery
- Avoid heavy sedation in patients with threatened airway obstruction
Neuromuscular Blockade
- Profound paralysis required until end of procedure
- Intermediate-duration agents: rocuronium, vecuronium, cisatracurium
- Sugammadex now allows reversal of profound rocuronium blockade → largely replaced succinylcholine infusions
- Morgan & Mikhail, p. 781
Ventilation Techniques
| Method | Description | Pros | Cons |
|---|---|---|---|
| MLT (Microlaryngeal tube) | Small-diameter (5.0-5.5 mm) long ETT with high-volume low-pressure cuff (Mallinckrodt MLT) | Protects airway; ETCO₂ monitoring; safe | Partially obscures posterior commissure / vocal folds; requires laser-safe tube if CO₂ laser used |
| Intermittent apnoea | Patient ventilated between surgical episodes; apnoeic during surgery | No tube in field | Hypercarbia risk; shorter operative windows (2-3 min) |
| Supraglottic jet ventilation (Venturi/Sanders) | High-pressure O₂ jet (30-50 psi) through laryngoscope side port; entrains room air (Venturi effect) | Best laryngeal exposure | Risk of barotrauma if expiration inadequate; CO₂ monitoring unreliable; risk of aspiration |
| Subglottic jet ventilation (Hunsacker Mon-Jet) | Small tube in posterior commissure below glottis; controlled jet ventilation | Better CO₂ monitoring; stable ventilation; good laryngeal exposure | More invasive; not for posterior commissure lesions |
| High-frequency jet ventilation (HFJV) | 80-300 breaths/min via small cannula | Quiet, still field | Complex; ETCO₂ unreliable |
Laser Precautions (when CO₂ laser used)
- Use a laser-resistant ETT (e.g., Laser-Flex, Lasertubus)
- Fill tracheal cuff with saline (not air) - saline acts as heat sink; add methylene blue to detect cuff puncture
- Pack throat with wet gauze to protect infraglottic structures
- Protect patient's eyes with wet gauze and tape
- Use minimum FiO₂ to support SpO₂ (minimize airway fire risk - avoid FiO₂ >0.3 with flammable gases)
Indications for Operative Direct Laryngoscopy / Microlaryngoscopy
Diagnostic
- Suspicious laryngeal lesion on flexible laryngoscopy requiring biopsy
- Assessment of dysplasia / carcinoma in situ with mapping biopsies
- Failure of indirect/flexible laryngoscopy to adequately visualize larynx
- Staging of laryngeal/hypopharyngeal malignancy (palpation of cricoarytenoid mobility, tumour extent)
Therapeutic / Operative
| Indication | Notes |
|---|---|
| Vocal fold polyps, nodules, cysts | Excision by microflap/cold instruments |
| Reinke's oedema (polypoid corditis) | Microsuction + microdebrider |
| Recurrent respiratory papillomatosis (RRP) | Microdebrider (gold standard); ± KTP/CO₂ laser |
| Laryngeal carcinoma (early T1/T2) | Transoral laser microsurgery (TLM) |
| Vocal fold granuloma | Excision (with acid reflux treatment) |
| Leukoplakia / dysplasia | Excision biopsy ± CO₂ laser |
| Subglottic/laryngotracheal stenosis | Cold instruments, laser, microdebrider; dilation |
| Laryngeal web | Division; keel insertion |
| Arytenoid granuloma, laryngocele | Excision |
| Subglottic cysts | Suspension MLB with excision/marsupialization |
| Vocal fold injection augmentation | For paralysis/paresis; Cymetra, fat, Restylane injection |
| Foreign body removal | From larynx, subglottis, trachea |
| Airway tumour debulking | Palliation of obstruction |
| Interarytenoid injection | May be performed at initial DL as diagnostic + therapeutic |
Procedure: Suspension Microlaryngoscopy
- Anaesthesia induction with TIVA (propofol/remifentanil) ± inhalational agents; profound NMB
- Patient positioned in Jackson (sniffing) position - shoulder roll, head ring
- Tooth guard applied to protect upper teeth/gums
- Laryngoscope introduced via the right side of the mouth, advanced along the right paraglossal gutter
- Tongue displaced to the left; laryngoscope advanced to visualize epiglottis
- Tip positioned in vallecula (Macintosh technique) or under epiglottis (Miller technique)
- Suspension apparatus attached to chest support - hands-free
- Operating microscope or 0°/30°/70° Hopkins rod telescopes used for magnification
- Systematic assessment: supraglottis → glottis → anterior commissure → posterior commissure → subglottis
- Arytenoid mobility palpated with a spatula
- Biopsies/operative procedures performed with cold instruments, laser, or microdebrider
- For discrete lesion: excision biopsy preferred over incisional biopsy (microflap technique for vocal cord lesions)
- For diffuse changes: representative biopsy from area that minimises voice impact (e.g., superior-lateral surface)
Microflap Technique (for Vocal Fold Surgery)
- A mucosal microflap is raised using a sickle knife
- The lesion is dissected from the superficial lamina propria
- The mucosa is replaced/trimmed conserving as much epithelium as possible
- Avoids injury to the vocalis muscle and preserves vibration of the vocal cord
- Minimises scarring and preserves voice quality
Post-operative Care
- Voice rest: 48 hours absolute voice rest; 7-10 days strict vocal rest (no control studies, but widely accepted practice) - Scott-Brown's, p. 892-899
- Gradual return to voicing under voice therapy guidance
- Proton pump inhibitors if laryngopharyngeal reflux suspected (reduces granuloma recurrence)
- Follow-up flexible laryngoscopy at 4-6 weeks
Complications
| Complication | Notes |
|---|---|
| Dental damage | Most common; chipped/avulsed upper teeth; tooth guard mandatory |
| Lip/tongue laceration | From laryngoscope pressure |
| Temporomandibular joint injury | From forced mouth opening |
| Tongue numbness (lingual nerve injury) | From compression |
| Vocal fold scarring/adhesion | Especially anterior commissure - avoid bilateral anterior commissure resection |
| Laryngeal oedema | Post-operative; may cause airway compromise |
| Laryngospasm | On recovery from anaesthesia |
| Airway fire | With laser; prevented by wet throat packs, laser-safe tube, minimising FiO₂ |
| Haemorrhage | Intra/post-operative |
| Failure to visualize | Difficult anatomy; short neck, limited mouth opening; micrognathia |
| Cervical spine injury | Rare; extreme hyperextension in osteoporotic patients |
| Broken laryngoscope suspension | Patient must never be left unattended |
Contraindications / Predictors of Difficult DL (LEMON Assessment)
- Look externally - micrognathia, prognathism, short neck, large tongue, obesity
- Evaluate the 3-3-2 rule - mouth opening <3 fingers; hyoid-chin distance <3 fingers; thyroid-floor of mouth <2 fingers
- Mallampati class III/IV
- Obstruction / Obesity
- Neck mobility - cervical spine disease, trauma, ankylosing spondylitis
Key Points Summary
- Direct laryngoscopy = direct line-of-sight visualization; microlaryngoscopy = DL + operating microscope with suspension
- Jackson (sniffing) position: neck flexed, head extended - aligns oral, pharyngeal, laryngeal axes
- Cormack-Lehane Grade I/IIA = easy; IIB/III = difficult; IV = failed - requires alternative
- BURP manoeuvre improves grade
- Anaesthesia: TIVA preferred; profound NMB; MLT tube (size 5.0-5.5) most common; jet ventilation when posterior commissure/vocal fold exposure needed
- Laser surgery requires laser-safe ETT + saline-filled cuff + minimum FiO₂
- Cold instrument microsurgery preferred for benign vocal fold lesions to preserve voice
- Microdebrider = gold standard for RRP
- Excision biopsy preferred over incisional for discrete lesions
- 48 hours absolute voice rest post-phonosurgery; 7-10 days strict rest
- Most common complication: dental trauma - always use tooth guard
Epiphora
"epiphora" lacrimal drainage obstruction management
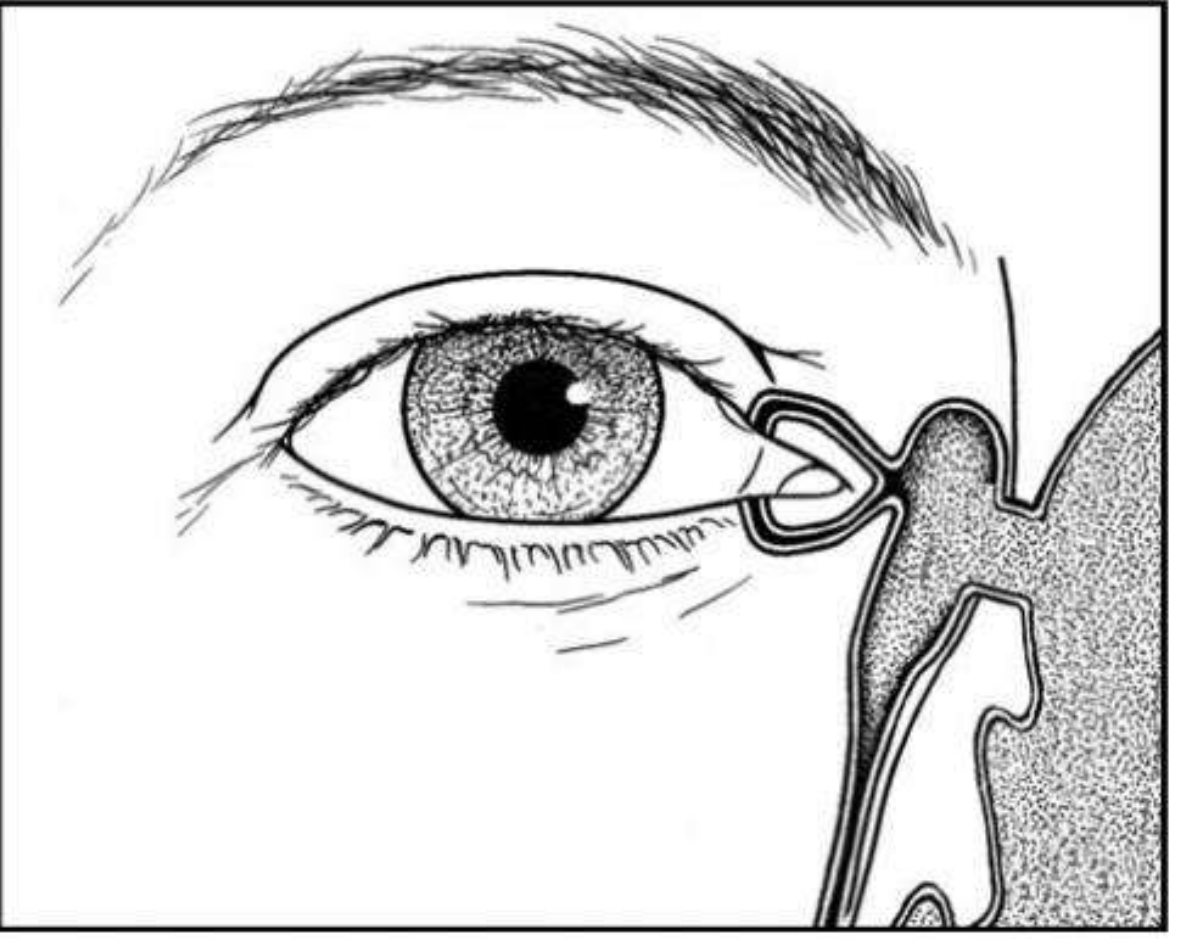
Epiphora
Definition
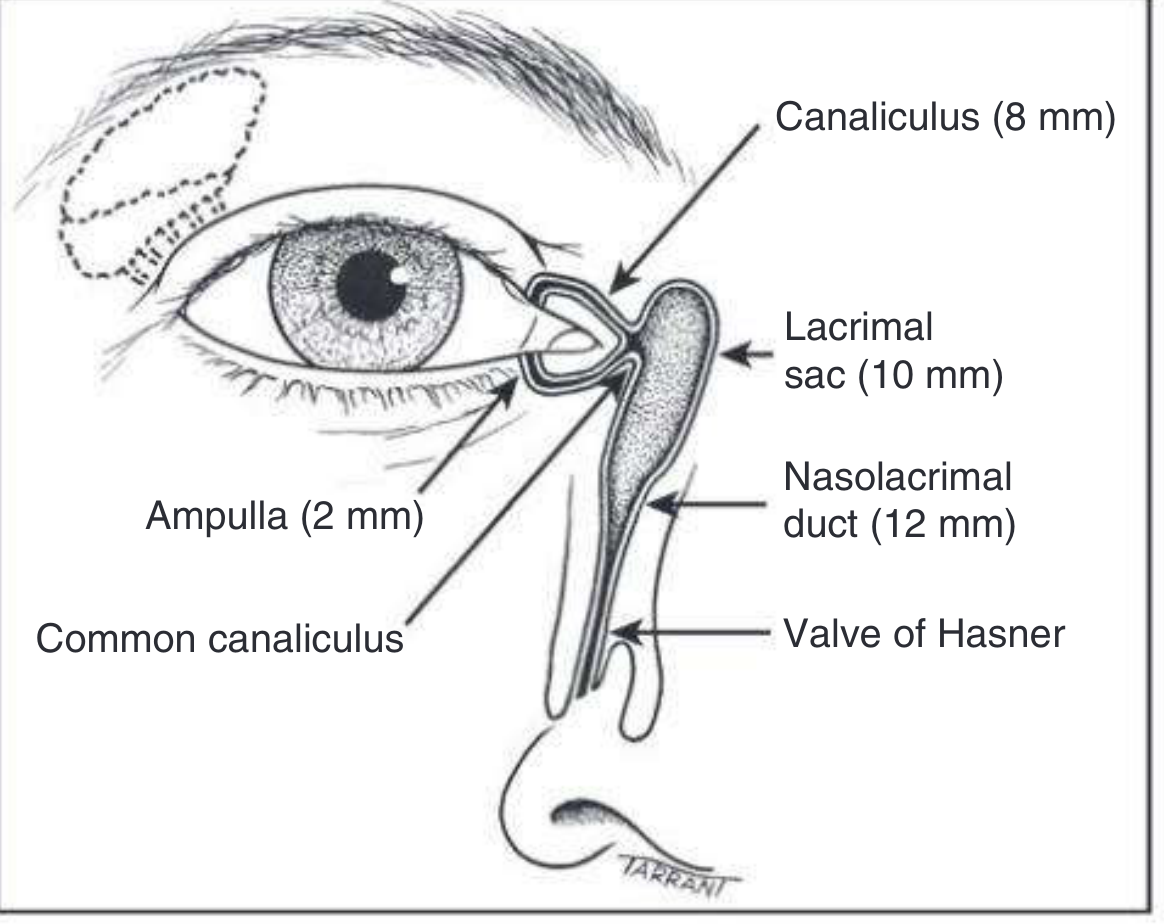
Anatomy of the Lacrimal Drainage System
| Structure | Size | Notes |
|---|---|---|
| Punctum (upper + lower) | ~0.3 mm diameter | Located on medial lid margin, ~6 mm from medial canthus |
| Ampulla | ~2 mm | Vertical dilated segment just below punctum |
| Canaliculus (upper + lower) | ~8 mm | Turns medially after ampulla |
| Common canaliculus | Short | Upper + lower canaliculi merge; enters lacrimal sac |
| Valve of Rosenmuller | - | Mucosal fold at canalicular-sac junction; prevents reflux |
| Lacrimal sac | ~10 mm | Lies in lacrimal fossa of lacrimal bone |
| Nasolacrimal duct (NLD) | ~12 mm | Runs through bony canal into inferior meatus |
| Valve of Hasner | - | Mucosal fold at distal NLD opening into inferior meatus |
Physiology of Tear Drainage (Lacrimal Pump)
- With each blink, the pretarsal orbicularis oculi compresses the ampullae and canaliculi and moves the puncta medially
- Contraction of the lacrimal part of orbicularis creates positive pressure, forcing tears down the NLD into the nose
- On eye opening, the canaliculi and sac expand creating negative pressure that draws tears from the canaliculi into the sac
- Kanski's, p. 4371-4373
Pathophysiology - Two Mechanisms of Epiphora
1. Hypersecretion (Overproduction)
- Secondary to anterior segment disease: dry eye (paradoxical watering), blepharitis, conjunctivitis, keratitis, foreign body, entropion
- Paradox: Dry eye stimulates reflex hypersecretion via the trigeminal-lacrimal reflex - the most common cause of watering eye overall
- Treatment is usually medical (addressing the underlying cause)
2. Defective Drainage (Lacrimal Outflow Failure)
- Malposition of puncta: ectropion, entropion, punctal eversion - "punctal abnormality is the most common cause of lacrimal drainage failure" - Kanski's, p. 4415
- Obstruction at any level from punctum to valve of Hasner
- Lacrimal pump failure: lower lid laxity, orbicularis weakness (facial nerve palsy)
Clinical tip: Drainage failure is exacerbated by cold/windy environments and least evident in warm, dry rooms. Tears overflowing onto the cheek = drainage failure (vs. hypersecretion which causes tears on the lower lid margin). - Kanski's, p. 4410
Causes at Each Level
| Level | Cause |
|---|---|
| Punctum | Punctal stenosis (primary - blepharitis, idiopathic; secondary - drugs [5-FU, docetaxel], radiation, cicatrizing conjunctivitis, HSV/HZV), punctal atresia, punctal ectropion, eyelash obstructing punctum, large caruncle |
| Canaliculus | Canaliculitis (Actinomyces israelii - most common cause), canalicular obstruction (scarring post-HSV, trachoma, pemphigoid), trauma |
| Common canaliculus | Dacryolith (lacrimal stone), trauma, post-radiation stenosis |
| Lacrimal sac | Dacryocystitis (acute/chronic), lacrimal sac tumour, dacryolith |
| Nasolacrimal duct | Idiopathic stenosis (most common acquired cause), trauma, nasal/sinus surgery, granulomatous disease (GPA, sarcoidosis), nasopharyngeal tumour infiltration, dacryolith, congenital obstruction (valve of Hasner) |
| Functional | Lacrimal pump failure (facial palsy, lid laxity), conjunctivochalasis |
Evaluation
History
- Unilateral vs. bilateral
- Age of onset (congenital vs. acquired)
- Discharge character (watery vs. mucoid vs. mucopurulent)
- Exacerbating factors (cold/wind → drainage failure)
- History of: trauma, nasal/sinus surgery, eye drops (especially glaucoma drops), systemic drugs, radiotherapy, granulomatous disease
Examination
- Slit-lamp examination of puncta (before any instrumentation - syringing temporarily dilates and masks stenosis)
- Assess for ectropion, entropion, lid laxity
- Fluorescein dye disappearance test (FDDT): Instil fluorescein; normal drainage = dye disappears from tear meniscus within 5 minutes; retained dye = drainage failure
- Tear meniscus height - elevated in drainage failure
- Regurgitation test: Digital pressure over lacrimal sac - if mucopurulent material regurgitates, indicates chronic dacryocystitis with NLD obstruction
Investigations
1. Lacrimal Syringing (Diagnostic Irrigation)
- Cannulate lower punctum → instil saline
- Normal: Saline tasted in throat = patent system
- Soft stop: Cannula meets resistance before entering sac = canalicular obstruction
- Hard stop: Cannula enters sac but fluid does not pass to nose; reflux through opposite punctum = NLD obstruction
- Reflux through the same punctum = lower canalicular obstruction; through upper punctum = common canalicular obstruction
- Kanski's, p. 4485-4498
2. Jones Dye Tests (for partial/functional obstruction)
- Jones I: Primary dye test - fluorescein instilled; recovered from nose on blowing = patent, functional drainage
- Jones II: Secondary dye test - after Jones I failure; syringe with saline; fluorescein in saline = punctum/canaliculus drains but pump fails; clear saline = canalicular obstruction
3. Dacryocystography (DCG)
- Contrast injection into canalicular system + X-ray/CT
- Shows site and extent of obstruction, sac size, filling defects (dacryoliths, tumour)
4. Lacrimal Scintigraphy (Nuclear DCG)
- Physiological test - radiolabelled technetium-99m drops instilled; gamma camera images
- Shows functional drainage (assesses pump mechanism as well as patency)
- "Nuclear lacrimal scintigraphy showing passage of tracer via the right lacrimal system but obstructed drainage in the left nasolacrimal duct" - Kanski's, Fig. 3.10
5. Nasal Endoscopy
- Assesses inferior meatus, valve of Hasner, septal deviation, nasal polyps, turbinate hypertrophy - important pre-DCR assessment
Dacryocystitis
Acute Dacryocystitis
- Sudden painful swelling at medial canthus below medial canthal tendon
- Red, tender, hot swelling in the region of the lacrimal sac
- Organisms: Staphylococcus aureus, Streptococcus pneumoniae
- Management: Systemic antibiotics (IV if severe); warm compresses; do NOT incise acutely (risk of fistula formation); DCR once infection resolved
Chronic Dacryocystitis
- Persistent epiphora + mucopurulent discharge
- Regurgitation of pus on pressure over lacrimal sac
- May present as a medial canthal swelling (mucocele/pyocele)
- Management: DCR is definitive
Congenital Nasolacrimal Duct Obstruction (CNLDO)
- Present in up to 20% of neonates
- Due to persistent membranous obstruction at valve of Hasner (last part to canalize)
- Natural history: Spontaneous resolution in majority; rapid in first year, continues beyond
- Presentation: epiphora + sticky eye from first month of life; increased tear meniscus; mucocele may develop
Treatment - Stepwise
- Conservative (< 12 months): Observation; Crigler massage (lacrimal sac massage) - 2-3x daily; topical antibiotics for infection
- Probing (12-24 months): Under GA; stepwise probing from punctum to Hasner valve; success rate ~90%
- Probing + silicone intubation: For failed probing or older children; stent left for 3-6 months
- Balloon dacryoplasty: For failed probing
- DCR: Rarely required in children - for persistent epiphora despite probing, bony atresia, upper NLD involvement
Dacryocystorhinostomy (DCR)
Three DCR Approaches (Success Rates - Cummings Table 49.1)
| Approach | Immediate Success | ~5-year Success |
|---|---|---|
| Endoscopic (endonasal) | 84-94% | 92% |
| External | 65-100% | 94% |
| Laser-assisted | 47-100% | 38% (poor long-term) |
A. External DCR
- Incision: vertical skin incision 10 mm medial to the inner canthus (avoiding angular vein)
- Medial canthal tendon and lacrimal sac exposed and reflected
- Intervening bone (anterior lacrimal crest + lacrimal fossa bone) removed
- Sac incised in an H-shaped manner to create anterior and posterior flaps
- Nasal mucosa incised; anterior and posterior flaps sutured together
- Silicone stents passed through canaliculi and NLD into nose (optional, 3-6 months)
- Success >90%
- Complications: Cutaneous scar, haemorrhage, angular vein injury, medial canthal structure injury, infection, CSF rhinorrhoea (if subarachnoid space entered), sump syndrome (ostium too high/small)
B. Endoscopic (Endonasal) DCR
- No skin incision → no external scar
- A light pipe through the canalicular system guides the endonasal approach
- Bone removed endoscopically; lacrimal sac marsupialized into middle meatus
- Transcanalicular laser/drill variants also exist
- Advantages: Less blood loss, no scar, shorter operative time, lower CSF risk, simultaneous nasal pathology addressed
- Disadvantages: Slightly lower success rate in some series; requires rhinological expertise; ~50% need additional nasal procedures
- "This concept allows outcomes of endonasal DCR to be equal or better than those of external DCR." - Cummings, p. 3776
C. Laser-Assisted DCR
- Laser (KTP, holmium, diode) creates ostium transcanalicularly
- Poor long-term results (38% at 5 years) - not recommended as primary approach
- Cummings, p. 3969
Adjunctive Measures
- Silicone stenting: Standard post-DCR; may be optional; little added benefit per recent data
- Mitomycin C / 5-FU: Antimetabolites to prevent scarring; evidence is mixed
- Grommet through medial sac wall / vertical slit without marsupialization: >65% failure rates - to be avoided
Management of Specific Situations
| Condition | Treatment |
|---|---|
| Punctal ectropion/stenosis | Punctoplasty (one/two/three-snip), mini-Monoka stent |
| Canaliculitis (Actinomyces) | Canaliculotomy + curettage + antibiotics (penicillin) |
| Lower canalicular obstruction | Jones tube (conjunctivodacryocystorhinostomy - CDCR) |
| Functional epiphora (pump failure) | Jones tube if severe; treat lid laxity; treat facial palsy |
| Conjunctivochalasis | Topical steroids; surgical excision/fixation |
| Dacryolith | Removal via DCR |
| NLD obstruction (acquired, adult) | Endoscopic or external DCR |
| Total canalicular obstruction | Lester Jones tube (CDCR) |
| Congenital NLD obstruction <12 mo | Conservative + massage |
| Congenital NLD obstruction >12 mo | Probing ± intubation |
Causes of Failed DCR / Recurrent Epiphora after DCR
- Sump syndrome - ostium too small and too high; lacrimal sac below the stoma retains secretions
- Unrecognized common canalicular obstruction (pre-existing, not addressed)
- Ostium stenosis/closure - scar tissue formation
- Inadequate sac marsupialization
- Nasal synechiae blocking ostium
- Residual functional failure - lacrimal pump dysfunction (ongoing despite patent system)
Key Points Summary
- Epiphora = tear overflow; two mechanisms: hypersecretion (dry eye, inflammation) vs. defective drainage
- Punctal abnormality = most common cause of lacrimal drainage failure
- Paradoxical watering from dry eye is the most common cause of a watering eye overall
- Lacrimal syringing is the key diagnostic test: hard stop + reflux = NLD obstruction; soft stop = canalicular obstruction
- Jones dye tests for functional/partial obstruction
- CNLDO: 20% neonates; observation until 12 months; probing after 1 year; DCR rarely needed
- DCR is definitive for NLD obstruction; external and endoscopic approaches have equivalent ~92-94% long-term success; laser DCR has poor long-term results (38%)
- Post-DCR failure: sump syndrome, canalicular obstruction, ostial scarring
- Canaliculitis (Actinomyces) presents with medial eyelid discharge, pouting punctum - treat with canaliculotomy
Photodynamic therapy
"photodynamic therapy" head neck cancer larynx
Photodynamic Therapy (PDT)
Definition
- A photosensitizing agent (photosensitizer)
- Light of a specific wavelength
- Molecular oxygen (O₂)
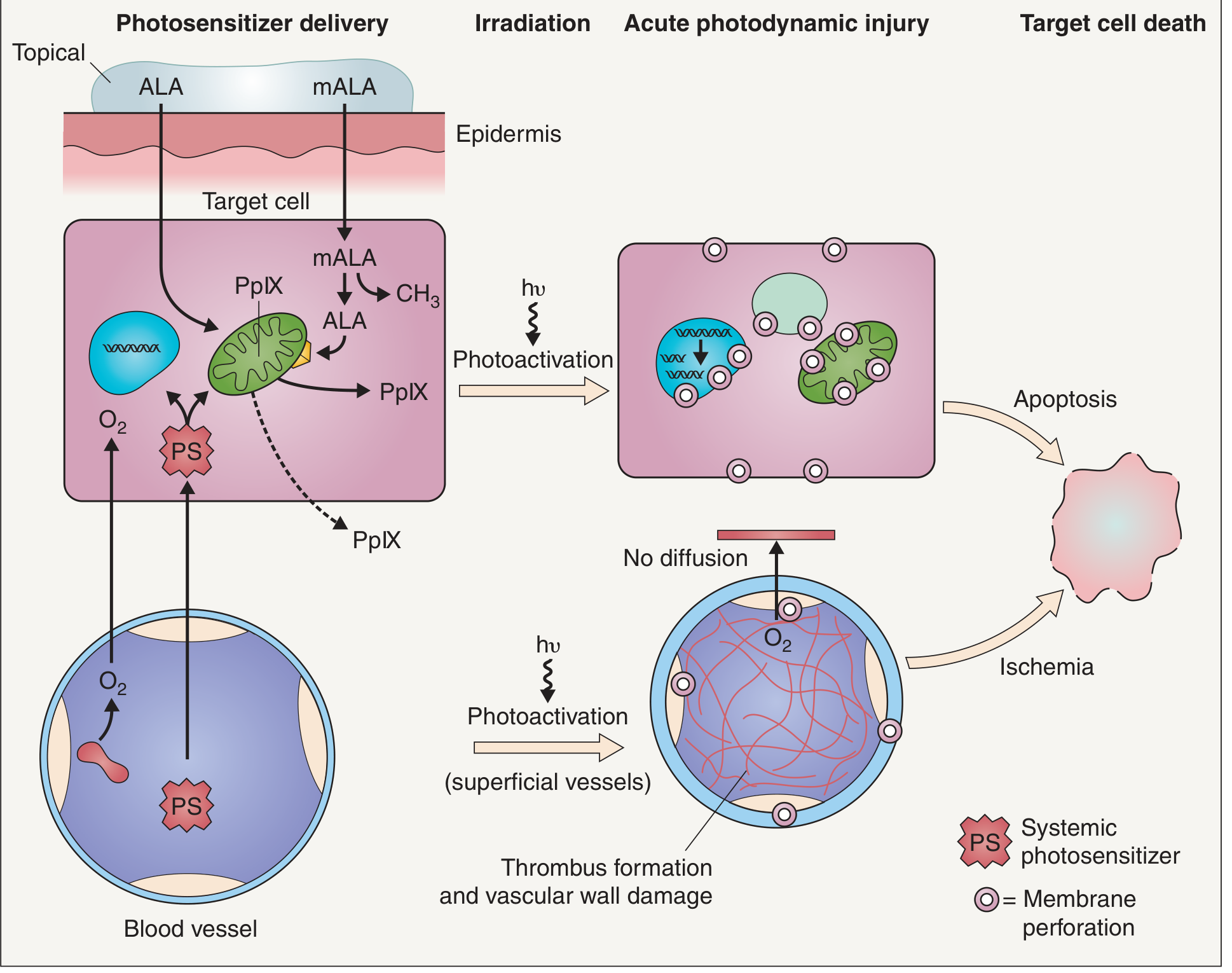
Mechanism of Action
Photochemical Steps (Jablonski Diagram)
- Photosensitizer delivered to target tissue (topically or systemically) - exists in ground state
- Light of appropriate wavelength absorbed → photosensitizer excited to singlet excited state (nanoseconds)
- Intersystem crossing → more stable triplet excited state (microseconds)
- Excited triplet photosensitizer transfers energy to molecular O₂ (Type II photochemical reaction):
Triplet PS + ³O₂ → Ground state PS + ¹O₂ (singlet oxygen)
- Singlet oxygen reacts with cellular biomolecules: lipids, proteins, nucleic acids
Two Pathways of Cell Death
| Pathway | Mechanism | Dominant in |
|---|---|---|
| Direct cellular injury | Singlet O₂ damages mitochondrial membranes, plasma membrane, endoplasmic reticulum → apoptosis | Topical PDT (ALA/mALA) |
| Vascular injury | ROS damages endothelial cells of tumour vasculature → thrombus formation → vascular collapse → ischemic necrosis | Systemic PDT (porfimer sodium) |
Why Is PDT Selective?
- Increased vascular permeability of tumour vessels (EPR effect)
- Tumour cells have abnormal metabolism with higher PpIX accumulation
- Reduced lymphatic drainage - photosensitizer not cleared quickly
- ALA/mALA penetrate better through abnormal stratum corneum overlying tumour
- Selectivity ratio: >10:1 (tumour vs. surrounding normal tissue) for ALA/mALA
Photosensitizers
First Generation (Systemic)
| Agent | Notes |
|---|---|
| Hematoporphyrin derivative (HpD) | First used (1970s); systemic IV administration |
| Porfimer sodium (Photofrin®) | Purified HpD; FDA-approved; systemic; activated at 630 nm; prolonged skin photosensitivity (4-6 weeks) - major disadvantage |
| Dihematoporphyrin ether (DHE) | Similar to porfimer; used in early head/neck trials |
Second Generation
| Agent | Notes |
|---|---|
| Temoporfin (mTHPC, Foscan®) | Meta-tetrahydroxyphenylchlorin; IV systemic; activated at 652 nm; more selective; shorter photosensitivity (2-4 weeks); used in head/neck cancer in Europe |
| Verteporfin (Visudyne®) | Benzoporphyrin derivative; IV; activated at 690 nm; photosensitivity ≤72 hours; primarily used in ophthalmology (age-related macular degeneration) |
Third Generation / Topical Prodrugs
| Agent | Notes |
|---|---|
| 5-Aminolevulinic acid (ALA) | Topical prodrug; converted intracellularly to protoporphyrin IX (PpIX) (active photosensitizer); naturally occurring intermediate in heme biosynthesis; activated at 417 nm (blue) or 630 nm (red) |
| Methyl aminolevulinate (mALA / Metvix®) | Methyl ester of ALA; more lipophilic → better skin penetration; greater selectivity for neoplastic cells |
ALA/mALA Mechanism:
- ALA bypasses the rate-limiting step (ALA synthase, feedback-inhibited by heme)
- Pharmacological ALA → overwhelming accumulation of PpIX in mitochondria → PpIX leaks to plasma membrane, ER
- Tumour cells: iron-deficient + rapidly proliferating → produce more PpIX than normal cells
Light Sources
| Source | Wavelength | Tissue Penetration | Use |
|---|---|---|---|
| Blue light (417-420 nm) | Soret band of PpIX | Superficial (<1 mm) | Actinic keratoses (epidermis) |
| Red light (630-635 nm) | Minor absorption peak of PpIX / porfimer | Deeper (up to 3 mm) | Dermal lesions, BCC, SCC, oesophageal/airway tumours |
| Near-infrared (652 nm) | Temoporfin activation | Deeper still | Head/neck tumours (Foscan) |
| 690 nm | Verteporfin activation | - | Choroidal neovascularization |
- Surface illumination: LED panels, lamp heads, diode lasers
- Optical fibres through flexible endoscope: For oesophageal, bronchial, bladder tumours
- Interstitial light propagation: Optical fibre needles inserted into tumour bulk - extends PDT to deeper tumours
- Diffuser tip fibres: For tubular structures (trachea, oesophagus)
Drug-Light Interval
- Systemic agents (porfimer, temoporfin): Drug-light interval 3-96 hours (allows washout from normal tissue)
- Topical ALA/mALA: Incubation 1-18 hours (allows selective accumulation in target cells)
PDT in ENT / Head and Neck Surgery
1. Early Laryngeal Cancer (T1/T2)
- Biel treated 25 patients with early SCC of the larynx using PDT; achieved complete response in all - notably in 17 patients in whom prior radiotherapy had failed
- Advantages: organ-preserving; repeatable; not compromised by prior RT, surgery, or chemotherapy
2. Oral Cavity and Oropharynx
- Karakullukcu et al. (170 patients, early-stage oral cavity/oropharynx): 90% response rate, 70% complete response (cure) rate
- Gluckman: oral cavity/oropharynx - 11/13 complete response, 2/13 partial response with dihematoporphyrin ether + 630 nm light
- "The endoscopic access to squamous tumours of the upper aerodigestive tract combined with the tendency to develop field cancerisation make these tumours good candidates for PDT" - Scott-Brown's, p. 3606-3610
3. Oesophageal Cancer
- Phase II RCT (218 patients): palliative PDT (porfimer sodium) vs. Nd:YAG laser
- Equivalent improvement in dysphagia
- Fewer perforations with PDT (1% vs. 7%, p<0.05)
- Barrett's oesophagus with dysplasia/early adenocarcinoma: PDT showed ablation in 43/55 patients
- Oesophageal stricture in 53% - significant complication
- Scott-Brown's, p. 3599-3604
4. Recurrent Respiratory Papillomatosis (RRP)
- Biel reported results of PDT for laryngeal papillomatosis with durable disease control
- Red Book 2021: photodynamic therapy listed as an adjuvant treatment option for RRP alongside interferon, indole-3-carbinol, bevacizumab
5. Endobronchial / Tracheobronchial Tumours
- PDT is an established bronchoscopic intervention for primary or metastatic tracheobronchial neoplasms
- Indications: malignant central airway obstruction, carcinoma in situ of bronchus
- Listed alongside laser, electrocautery, cryotherapy, brachytherapy in bronchoscopic armamentarium
- Fishman's Pulmonary Diseases, p. 3987 (Table 34-1)
6. Nasopharyngeal Carcinoma
- PDT trials for squamous carcinoma of the nasopharynx reported
7. Sinonasal Inverted Papilloma
- Non-malignant application; targeted due to recurrent nature
8. Oral Dysplasia / Leukoplakia (Pre-malignant)
- ALA/mALA-based PDT used for oral epithelial dysplasia
PDT in Ophthalmology
- IV verteporfin → selectively accumulates in neovascular endothelium
- Activated at 689 nm via low-power diode laser directed at CNV
- Causes thrombosis of choroidal new vessels without damaging overlying retina
- Kanski's Clinical Ophthalmology (dedicated section)
PDT in Dermatology
| Indication | Evidence |
|---|---|
| Actinic keratoses | ALA/mALA; clearance 50-70% single tx; up to 90% with repeat |
| Basal cell carcinoma (superficial) | FDA/EMA approved; 87-95% clearance |
| Bowen disease (SCC in situ) | mALA approved; high clearance rates |
| Superficial SCC | Approved in Europe |
| Acne vulgaris | ALA-PDT; reduces sebaceous gland activity |
| Photorejuvenation | ALA/mALA; cosmetic improvement of photoaged skin |
| Localised scleroderma | Systemic PDT |
| Cutaneous leishmaniasis | PDT trials |
Advantages of PDT
- Organ preservation - no ablative surgery needed for early lesions
- Selectivity - photosensitizer preferentially retained in tumour tissue
- No effect from prior treatments - not affected by prior radiotherapy, chemotherapy, or surgery (Scott-Brown's, p. 3562)
- Repeatable - can be given multiple times without cumulative toxicity
- Minimal long-term side effects
- Minimal scarring compared to surgery
- Can treat field cancerisation (wide area treatment)
- Suitable for patients on anticoagulation
- No dark toxicity - photosensitizer harmless without light activation
Limitations and Side Effects
| Limitation | Details |
|---|---|
| Skin phototoxicity | Major disadvantage of systemic agents; porfimer = 4-6 weeks sun avoidance; temoporfin = 2-4 weeks; verteporfin ≤72 hours |
| Limited tissue penetration | Light penetrates only 3 mm at 630 nm; limits treatment to superficial lesions without interstitial delivery |
| Intraoperative pain | Often intense at light exposure site; significant patient disincentive |
| Oesophageal stricture | 53% after PDT for Barrett's/oesophageal cancer |
| Tumour oedema | Post-treatment swelling can compromise airway |
| Cost | Commercial PDT systems are expensive |
| Variable drug-light dosimetry | Difficult to standardise; multiple permutations of dose/light |
| Requires oxygen | Hypoxic tumour cores may be resistant |
Key Points Summary
- PDT requires three components: photosensitizer + light + oxygen
- Mechanism: photosensitizer → excited triplet state → energy transfer to O₂ → singlet oxygen → cell death by apoptosis (topical) or vascular thrombosis/ischaemia (systemic)
- First-generation: porfimer sodium (Photofrin) - systemic; long phototoxicity; 630 nm
- Second-generation: temoporfin (Foscan) for head/neck; verteporfin for AMD
- Third-generation: ALA/mALA topical prodrugs → PpIX; used in dermatology
- Depth of light penetration: blue light (417 nm) = superficial (<1 mm); red light (630 nm) = deeper (up to 3 mm)
- Drug-light interval (3-96 h for systemic) allows normal tissue washout → selectivity
- ENT applications: early laryngeal SCC, oral cavity/oropharynx carcinoma, oesophageal cancer (palliative), RRP, endobronchial tumours
- PDT is not compromised by prior RT, surgery, or chemotherapy
- Major limitations: skin phototoxicity, limited penetration depth, pain, oesophageal stricture risk
Faucial diphtheria
"diphtheria" clinical management antitoxin
Bat ear
"prominent ear" otoplasty surgical technique
Bat Ear (Prominent Ear / Prominauris / Protruding Ear)
Definition
Anatomy of the Normal Ear
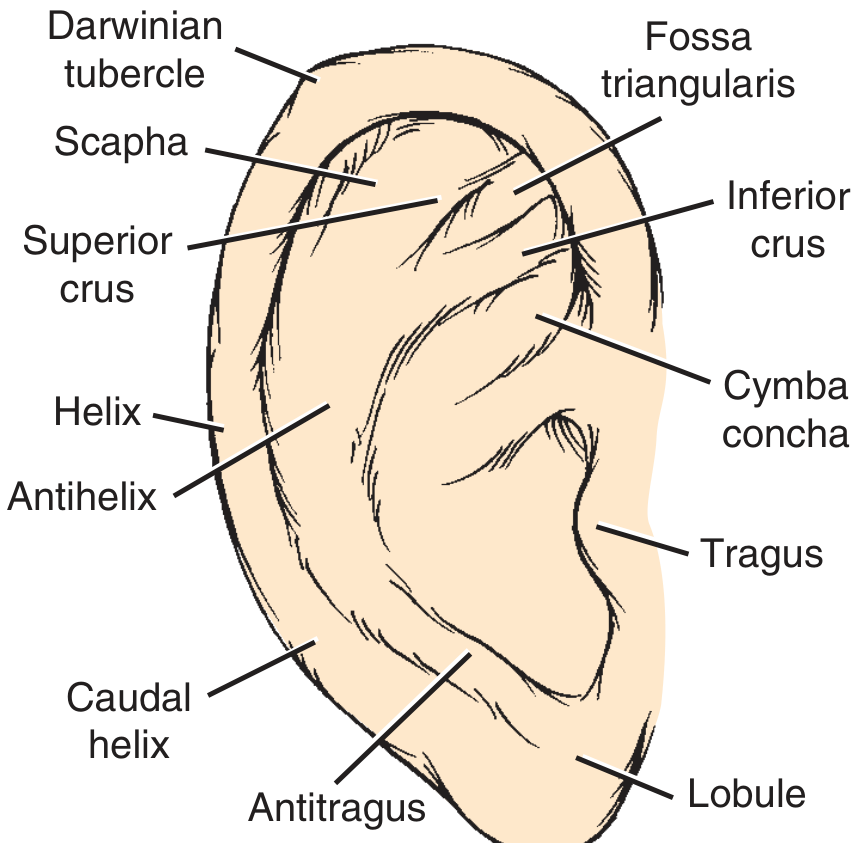
Key anatomical norms
| Measurement | Normal Value |
|---|---|
| Ear length (adult) | 5.5 - 6.5 cm |
| Ear width | 50-60% of length |
| Long-axis posterior rotation | 15-30 degrees |
| Superior helix level | Level of eyebrow |
| Lobule level | Level of subnasale (columella base) |
| Auriculocephalic angle | 20-35° (>40° = abnormal) |
| Scalp-helix distance: superior | 10-12 mm |
| Scalp-helix distance: mid-helix | 16-18 mm |
| Scalp-helix distance: caudal helix | 20-22 mm |
| Conchal bowl depth | ≤1.5 cm |
| Helix rim lateral to antihelix | 2-5 mm |
Embryology and Development
- The auricle develops from six hillocks of His on the first and second branchial arches, fusing during weeks 6-12 of gestation
- The antihelix furls during weeks 12-16; failure to do so results in protruding scapha (the most common cause of bat ear)
- The helix furls during the 6th month of gestation
- By age 3: 85% of auricular growth is complete
- By age 5: cartilaginous growth is nearly complete - suitable age for surgery
Aetiology (Anatomic Causes)
1. Underdeveloped (absent/poorly formed) antihelical fold - MOST COMMON
- Failure of the antihelix to furl produces a flat, featureless ear
- The scapha (flat area between helix and antihelix) flares outward
- Conchoscaphal angle >90° (normal = 90°)
2. Deep/large conchal bowl (conchal hypertrophy)
- A deep conchal bowl pushes the entire auricle laterally away from the head
- Conchal depth >1.5 cm is abnormal
- Conchomastoid angle >90° (normal = 90°)
3. Combination (both)
- Most patients have elements of both antihelical underdevelopment and conchal excess
4. Prominent lobule
- An inferiorly protruding lobule may accompany the above
Psychosocial Impact
- Significant psychological impact on children from teasing and bullying by peers, particularly after starting school (~age 5)
- "The entity has no significant otologic ramifications; rather, its importance is determined by the psychological disturbance endured by the patient." - Shambaugh Surgery of the Ear, p. 1725
- May lead to low self-esteem, social withdrawal, anxiety
Assessment
Clinical Evaluation
- Document both ears separately - asymmetry is common; each ear may need a different corrective plan
- Measure auriculocephalic angle and scalp-helix distance
- Identify whether the problem is: antihelix deficiency / conchal excess / both / lobule
- Preoperative photography is mandatory
Surgical Planning Priorities
- Correct protrusion of helix and lobe
- Create a smooth, natural-looking antihelical fold
- Avoid overcorrection (helix should remain visible lateral to antihelix on frontal view)
- Create bilateral symmetry
Treatment
1. Non-Surgical / Ear Moulding (Neonates)
- Indicated within the first few weeks of life while auricular cartilage is still pliable (maternal oestrogen maintains cartilage plasticity for 4-6 weeks post-birth)
- External splints, foam moulding devices, or adhesive tape applied to reshape the ear
- Most effective if started within the first 72 hours of birth
- By 3-4 months, the cartilage hardens and moulding becomes ineffective
- Does not require anaesthesia; avoids surgical risks
2. Surgical Otoplasty
Surgical Techniques
A. Suture-Based Techniques (Cartilage-Sparing)
Mustardé Technique (Most Widely Used)
- Principle: Horizontal mattress sutures placed through cartilage and anterior perichondrium to recreate the antihelical fold by rolling the scaphoid fossa toward the concha
- Approach: Postauricular (posterior auricular skin excision + mattress sutures)
- Steps:
- Preoperative ink markings define the crest of the new antihelix; marking sutures placed through anterior skin with ear folded into correct position
- Elliptical skin incision in postauricular sulcus
- Posterior auricular skin elevated to helical rim and triangular fossa (avoid nicking cartilage)
- Tissues elevated from conchal cartilage toward mastoid periosteum; intrinsic/extrinsic muscles divided
- 3-4 Mustardé sutures (5-0 or 6-0 non-absorbable, taper needle) placed as horizontal mattress sutures through cartilage and anterior perichondrium
- Each suture temporarily tightened to fold antihelix; all placed before tying
- Helix should remain visible lateral to new antihelix
- Conchomastoid sutures (4-0 or 5-0, >1 stitch): conchal cartilage tacked to mastoid periosteum to reduce conchal depth if needed
- Conchal cartilage may be thinned or excised if excessive
- Upper pole: stitch between triangular fossa and deep temporal fascia if needed
- Redundant posterior skin excised; wound closed
- Ear dressed with cotton packing in contours + mastoid pressure dressing
Incisionless Otoplasty (Fritsch / Merck Technique)
- Suture loop passed through small puncture sites - no skin incision
- 4-pass needle technique: horizontal pass through posterior skin and cartilage → under postauricular skin → second horizontal pass → exit through initial entry point
- Advantages: minimal scarring, faster recovery
- Suitable for mild-moderate deformity
B. Cartilage-Cutting / Scoring Techniques
| Technique | Description |
|---|---|
| Luckett (1910) | Single incision through posterior cartilage to recreate antihelical fold; first described technique |
| Converse-Wood-Smith | Parallel cartilage incisions (creates tube effect for antihelix) |
| Stenstrom scoring | Anterior surface cartilage abrasion/scoring to cause cartilage to curve away from scored side (Gibson's principle) |
- Gibson's principle: When one surface of cartilage is scored/abraded, it bends away from the scored surface (intrinsic cartilage memory released)
- Cartilage-cutting techniques have higher hematoma rates (~3%) than suture-only techniques
C. Conchal Reduction Techniques
- Conchal bowl shaving/excision: Direct excision of posterior conchal cartilage to reduce depth
- Conchomastoid (Furnas) sutures: Conchal cartilage sutured to mastoid periosteum - brings concha closer to head without excision
- Suitable when conchal hypertrophy is the main cause
Summary of Technique Selection
| Deformity | Preferred Technique |
|---|---|
| Absent/poor antihelical fold | Mustardé sutures ± scoring |
| Deep conchal bowl | Furnas (conchomastoid) sutures ± conchal excision |
| Both | Combined: Mustardé + Furnas |
| Prominent lobule | Cauda-concha suture or soft tissue excision |
| Neonatal (age <6 weeks) | Ear moulding splint |
Postoperative Care
- Dressing removed at postoperative day 1 to check for haematoma and pressure injury
- Dressing replaced for a few days
- Headband worn for 3-4 months post-surgery to maintain ear position during healing
- Frequent post-op review to check ear position
Complications
Early
| Complication | Notes |
|---|---|
| Haematoma | Most serious early complication; ~3% incidence (higher with cutting techniques); leads to cauliflower ear if untreated; treat by immediate drainage + pressure dressing + IV antibiotics |
| Pain | Worsening pain post-op = suspect haematoma |
| Infection | Organisms: S. aureus, E. coli, Pseudomonas; treat with drainage + antibiotics |
| Perichondritis | Follows infection/haematoma; IV antibiotics + debridement |
| Cartilage necrosis | From infection, haematoma, excess cautery, or tight dressings |
Late
| Complication | Notes |
|---|---|
| Suture extrusion/granuloma | Braided > monofilament; remove suture + granuloma |
| Relapse/recurrence | Cartilage overcomes suture fixation; use multiple redundant sutures + scoring |
| Overcorrection | Helix not visible behind antihelix on frontal view ("pinned-back" appearance) |
| Telephone deformity | Mid-ear over-corrected; upper and lower poles protrude; due to inadequate pole correction or excess conchal removal |
| Hypertrophic scar / keloid | Postauricular (less visible); risk in predisposed patients |
| Hypoaesthesia | Sensory loss due to nerve injury |
| Cold susceptibility | Altered circulation |
| Asymmetry | From different techniques applied to each ear |
Key Points Summary
- Bat ear = prominent ear = prominauris; most common congenital auricular deformity
- Two causes: absent antihelical fold (most common) + deep conchal bowl
- Auriculocephalic angle >40-45° is abnormal (normal 20-35°)
- Ear reaches 85% adult size by age 3; surgery safe at age 5-6
- Non-surgical: ear moulding within first few weeks of life
- Gold standard surgical technique: Mustardé horizontal mattress sutures to recreate antihelical fold (posterior approach, cartilage-sparing)
- Conchal excess: Furnas conchomastoid sutures ± conchal excision
- Most dreaded early complication: haematoma → cauliflower ear
- Most common late complication: relapse (suture failure)
- Notorious aesthetic complications: overcorrection (pinned-back ear) and telephone deformity
- Post-op headband worn for 3-4 months
Now delivering the full answer above - here is the compiled response:
Bat Ear (Prominent Ear / Prominauris)
Definition
Anatomy of the Normal Auricle
Normal measurements
| Parameter | Normal |
|---|---|
| Auriculocephalic angle | 20-35° |
| Scalp to superior helix | 10-12 mm |
| Scalp to mid helix | 16-18 mm |
| Scalp to caudal helix | 20-22 mm |
| Helix lateral to antihelix | 2-5 mm |
| Conchal bowl depth | ≤1.5 cm |
| Superior helix level | Level of eyebrow |
| Inferior lobule level | Level of subnasale |
| Long axis posterior rotation | 15-30° |
Embryology and Development
- Auricle arises from six hillocks of His (1st and 2nd branchial arches), fusing during gestation weeks 6-12
- Antihelix furls at weeks 12-16; failure causes protruding scapha - the most common cause of bat ear
- Helix furls at 6 months gestation
- 85% of auricular growth complete by age 3; cartilage growth nearly complete by age 5
- Surgery is safe at age 5-6 without hindering growth
Causes (Anatomic Defects)
| Cause | Angle Abnormality | Frequency |
|---|---|---|
| Absent/underdeveloped antihelical fold | Conchoscaphal angle >90° | Most common |
| Deep/hypertrophic conchal bowl | Conchomastoid angle >90° / conchal depth >1.5 cm | Second |
| Combination of both | Both angles abnormal | Common |
| Prominent lobule | - | Less common, often co-exists |
Treatment
1. Ear Moulding (Non-surgical - Neonates)
- Window: First few weeks of life (maternal oestrogen keeps cartilage pliable; best results within 72 hours of birth)
- External foam/silicone splints reshape the cartilage painlessly
- By 3-4 months, cartilage hardens and moulding becomes ineffective
- No anaesthesia, no scarring
2. Surgical Otoplasty
Surgical Techniques
A. Mustardé Suture Technique (Gold Standard)
- Marking sutures through anterior skin with ear manually folded into position to define new antihelix crest
- Elliptical postauricular skin incision and excision
- Posterior skin elevated to helical rim and triangular fossa; conchal cartilage elevated to mastoid periosteum
- Intrinsic/extrinsic auricular muscles divided
- 3-4 horizontal mattress sutures (5-0 or 6-0 non-absorbable monofilament, taper needle) placed through cartilage and anterior perichondrium - rolls the scaphoid fossa toward the concha, recreating the antihelical fold
- All sutures placed before tying; tied sequentially with repeated assessment
- After setting the antihelix, assess residual conchal depth
- Conchomastoid (Furnas) sutures added if needed: 4-0 or 5-0 non-absorbable stitch tacking conchal cartilage to mastoid periosteum
- Upper pole addressed with fossa triangularis-temporalis fascia stitch if prominent
- Lobule addressed if needed
- Redundant posterior skin excised; wound closed
- Pressure dressing with cotton conforming to auricular contours
B. Cartilage-Scoring / Cutting Techniques
| Technique | Principle |
|---|---|
| Luckett (1910) | Single full-thickness cartilage incision posteriorly to recreate antihelical fold; first historical technique |
| Converse-Wood-Smith | Two parallel cartilage incisions creating a tube for the antihelix |
| Stenstrom / anterior scoring | Abrasion of anterior cartilage surface → Gibson's principle (cartilage curls away from scored surface) |
- Gibson's principle: Cartilage bends away from a scored surface due to release of intrinsic stress
- Cutting techniques have higher haematoma rates (~3%) vs. suture-only
C. Incisionless Otoplasty
- No skin incision - sutures passed through puncture sites only
- 4-pass needle loop technique through posterior auricular skin and cartilage
- Suitable for mild-to-moderate deformity
- Minimal scarring, faster recovery
D. Conchal Reduction
- Furnas (conchomastoid) sutures: conchal cartilage sutured to mastoid periosteum
- Direct conchal bowl excision/shaving: for severe conchal hypertrophy
- Indicated when conchal depth >1.5 cm is the dominant problem
Technique Selection Summary
| Dominant Defect | Preferred Technique |
|---|---|
| Absent antihelical fold | Mustardé mattress sutures |
| Deep conchal bowl | Furnas conchomastoid sutures ± excision |
| Both | Combined Mustardé + Furnas |
| Neonatal (<6 weeks) | Ear moulding splint |
| Mild, any age | Incisionless suture technique |
Postoperative Care
- Dressing removed at day 1 to inspect for haematoma and pressure injury
- Dressing re-applied for a few days
- Headband worn for 3-4 months post-surgery to hold ear in position during healing
- Frequent follow-up to assess position
Complications
Early
| Complication | Key Points |
|---|---|
| Haematoma (~3%) | Most serious early complication; worsening pain is the first symptom; must be drained immediately; if untreated → cauliflower ear (fibrocartilaginous organisation) |
| Infection | S. aureus, Pseudomonas, E. coli; treat with drainage + broad-spectrum antibiotics |
| Perichondritis | Secondary to infection/haematoma; IV antibiotics + debridement |
| Cartilage necrosis | From infection, haematoma, excess cautery, or tight dressings |
Late
| Complication | Key Points |
|---|---|
| Relapse/recurrence | Cartilage spring overcomes sutures; use multiple redundant sutures + scoring to reduce |
| Overcorrection | Helix hidden behind antihelix on frontal view ("pinned-back" appearance) - sutures too tight |
| Telephone deformity | Upper and lower poles remain prominent while middle is over-corrected; due to inadequate pole treatment or excess mid-conchal removal |
| Suture granuloma / extrusion | Braided > monofilament; remove suture + granuloma |
| Keloid / hypertrophic scar | Postauricular location; less visible but problematic in susceptible patients |
| Hypoaesthesia | Nerve injury (great auricular nerve most at risk) |
| Cold susceptibility | Impaired circulation |
| Asymmetry | Different techniques used on each ear; different cartilage stiffness |
Key Points
- Bat ear = prominauris; auriculocephalic angle >40-45°; normal is 20-35°
- Two mechanisms: absent antihelical fold (most common) + deep conchal bowl
- Antihelix failure to furl (weeks 12-16 gestation) is the root cause in most cases
- No hearing impairment; psychological impact (bullying) drives treatment
- Surgery at age 5-6; non-surgical ear moulding if neonate (<6 weeks)
- Mustardé technique (posterior horizontal mattress sutures) is the gold standard for antihelical fold reconstruction
- Furnas technique (conchomastoid sutures) addresses conchal bowl excess
- Most serious early complication: haematoma (→ cauliflower ear)
- Classic late aesthetic complications: overcorrection (helix hidden) and telephone deformity (poles prominent, mid-ear flat)
- Headband worn for 3-4 months post-operatively
Give in detail about Monoclonal antibioty and its applications in ENT
"monoclonal antibody" "chronic rhinosinusitis" "nasal polyps" biologic
Monoclonal Antibodies (mAbs) and Their Applications in ENT
What Is a Monoclonal Antibody?
Nomenclature
| Suffix | Source | Example |
|---|---|---|
| -omab | Murine (mouse) | Ibritumomab |
| -ximab | Chimeric (mouse + human) | Cetuximab, Rituximab |
| -zumab | Humanized (mostly human) | Bevacizumab, Pembrolizumab |
| -umab | Fully human | Panitumumab, Dupilumab |
- -ci- = cardiovascular
- -li- = immune/inflammatory
- -tu- = tumour
- -ki- = interleukin
Classification by Target / Mechanism
| Class | Mechanism | Examples |
|---|---|---|
| Anti-IgE | Blocks free IgE, prevents mast cell/basophil degranulation | Omalizumab |
| Anti-IL-4/IL-13 | Blocks Type 2 Th2 inflammatory cytokines | Dupilumab |
| Anti-IL-5 / Anti-IL-5Rα | Reduces eosinophil production and survival | Mepolizumab, Benralizumab, Reslizumab |
| Anti-TSLP | Blocks upstream epithelial alarmin | Tezepelumab |
| Anti-EGFR | Blocks epidermal growth factor receptor → inhibits tumour proliferation | Cetuximab, Panitumumab |
| Anti-PD-1 | Checkpoint inhibitor - restores T-cell anti-tumour immunity | Pembrolizumab, Nivolumab |
| Anti-CTLA-4 | Checkpoint inhibitor - prevents T-cell suppression | Ipilimumab |
| Anti-VEGF | Inhibits angiogenesis (tumour/papilloma vascularity) | Bevacizumab |
ENT Application 1: Chronic Rhinosinusitis with Nasal Polyps (CRSwNP)
Background
- CRSwNP is driven by Type 2 (Th2) inflammation with elevated IL-4, IL-5, IL-13, and IgE
- Key cells: eosinophils, mast cells, innate lymphoid cells type 2 (ILC2)
- Biologics target this eosinophilic/Th2 inflammatory cascade
- Indicated for: severe, refractory CRSwNP that fails topical steroids and/or surgery (or recurs post-surgery)
1. Dupilumab (Dupixent®) - FIRST-LINE BIOLOGIC
| Feature | Detail |
|---|---|
| Target | IL-4Rα (shared receptor for IL-4 and IL-13) → blocks both IL-4 and IL-13 simultaneously |
| Route | Subcutaneous injection every 2 weeks (300 mg) |
| FDA approval | CRSwNP (2019); asthma (2018); atopic dermatitis (2017) |
| Key trials | LIBERTY NP SINUS-24 and SINUS-52: significant reduction in nasal polyp score, nasal congestion, loss of smell; reduced need for systemic steroids and revision surgery |
| ENT effects | Reduces polyp burden, improves nasal patency and smell, reduces systemic steroid use |
| Side effects | Injection site reactions, conjunctivitis, transient eosinophilia (hypereosinophilia paradox) |
2. Omalizumab (Xolair®)
| Feature | Detail |
|---|---|
| Target | Free IgE - binds to Fc region of IgE, preventing binding to FcεRI on mast cells/basophils |
| Route | Subcutaneous every 2-4 weeks (dose based on IgE level and body weight) |
| FDA approval | Allergic asthma (2003); chronic idiopathic urticaria; CRSwNP (2020) |
| Mechanism | Reduces free IgE by 90-95%; downregulates FcεRI expression; reduces mast cell/basophil activation |
| ENT effects | Reduces nasal polyp size, improves symptom scores, reduces need for surgery; also benefits allergic rhinitis |
| Selection | High baseline IgE (30-700 IU/mL), elevated blood eosinophils, high FeNO → best predictors of response |
| Side effects | Injection site reactions; rare anaphylaxis (must observe 30 min post-dose) |
3. Mepolizumab (Nucala®)
| Feature | Detail |
|---|---|
| Target | IL-5 (anti-IL-5 antibody) |
| Route | Subcutaneous 100 mg every 4 weeks |
| FDA approval | Severe eosinophilic asthma; eosinophilic granulomatosis with polyangiitis (EGPA) |
| ENT effects | Reduces eosinophilic CRSwNP polyp burden; reduces blood and tissue eosinophils; efficacy in EGPA (a granulomatous vasculitis affecting ENT - sinonasal involvement, subglottic stenosis) |
| Evidence | Phase III trials showing polyp size reduction and symptom improvement in eosinophilic CRSwNP |
4. Benralizumab (Fasenra®)
| Feature | Detail |
|---|---|
| Target | IL-5Rα (receptor for IL-5 on eosinophils and basophils) - produces ADCC-mediated eosinophil depletion |
| Route | Subcutaneous 30 mg every 4 weeks x3, then every 8 weeks |
| Unique mechanism | Direct eosinophil depletion (near-complete) via antibody-dependent cell cytotoxicity (ADCC) - faster and more complete than anti-IL-5 antibodies |
| ENT effects | Reduces eosinophilic CRSwNP; studied in EGPA |
5. Tezepelumab (Tezspire®)
| Feature | Detail |
|---|---|
| Target | TSLP (thymic stromal lymphopoietin) - an upstream epithelial "alarmin" that initiates the entire Type 2 cascade |
| Route | Subcutaneous 210 mg every 4 weeks |
| Significance | Blocks the most upstream trigger of Th2 inflammation; effective in both eosinophilic and non-eosinophilic asthma/CRS; broader mechanism than IL-5/IL-4/IL-13 targeting |
| ENT | Emerging evidence for CRSwNP (PMID 39636450 - 2024 review confirms role in CRSwNP) |
Biologic Selection for CRSwNP
| Biomarker | Preferred Agent |
|---|---|
| Elevated IgE + allergic sensitization | Omalizumab |
| Elevated blood eosinophils (>300/μL) | Mepolizumab or Benralizumab |
| High FeNO + eosinophilia | Dupilumab |
| Comorbid atopic dermatitis/asthma | Dupilumab |
| Non-eosinophilic endotype | Tezepelumab |
| EGPA | Mepolizumab |
ENT Application 2: Head and Neck Squamous Cell Carcinoma (HNSCC)
1. Cetuximab (Erbitux®) - Anti-EGFR
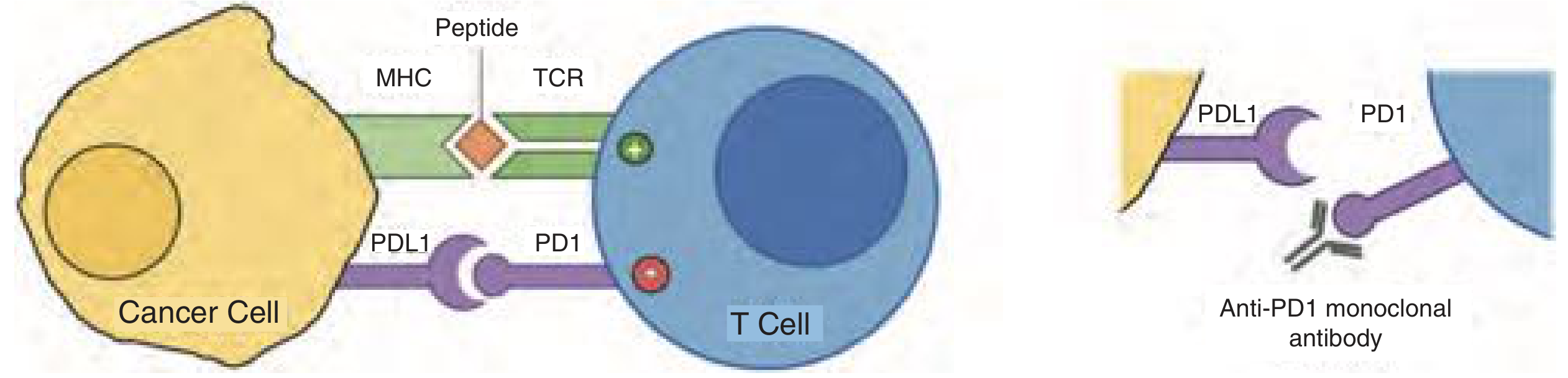
| Feature | Detail |
|---|---|
| Type | Chimeric IgG1 monoclonal antibody |
| Target | EGFR (epidermal growth factor receptor) - overexpressed in >90% of HNSCCs |
| Mechanism | Competitively inhibits EGF and TGF-α binding to EGFR → inhibits downstream RAS/MAPK and PI3K/Akt signalling → reduced proliferation, invasion, angiogenesis + ADCC |
| FDA approval | HNSCC (locoregionally advanced and recurrent/metastatic) |
| Key trial - Bonner (2006) | Radiation vs. radiation + cetuximab in locally advanced HNSCC: cetuximab improved locoregional control (24.4 vs 14.9 months) and OS (49 vs 29.3 months); established cetuximab + RT as standard |
| Key trial - EXTREME | Cetuximab + platinum/5-FU vs. chemotherapy alone in recurrent/metastatic HNSCC: improved OS (10.1 vs 7.4 months); established EXTREME regimen as first-line standard |
| HPV status | HPV-positive HNSCC derives less benefit from cetuximab monotherapy; HPV-negative patients respond better |
| Monotherapy response rate | <10% as single agent |
| Side effects | Acneiform rash (severity correlates with treatment response), hypomagnesaemia, infusion reactions (severe in <3%), fatigue |
2. Pembrolizumab (Keytruda®) - Anti-PD-1 Checkpoint Inhibitor
| Feature | Detail |
|---|---|
| Type | Humanized IgG4 antibody |
| Target | PD-1 (programmed cell death protein 1) on T cells |
| Mechanism | Blocks PD-1 from binding PD-L1 on tumour cells → prevents T-cell exhaustion → restores cytotoxic T-cell tumour killing |
| FDA approval | First-line treatment of recurrent/metastatic HNSCC (2019, as monotherapy for PD-L1 CPS ≥1, and in combination with chemotherapy) |
| Key trials | KEYNOTE-012 (Phase Ib), KEYNOTE-055, KEYNOTE-040, KEYNOTE-048 |
| KEYNOTE-048 | Pembrolizumab + chemotherapy vs. EXTREME regimen: superior OS for PD-L1 CPS ≥1 patients; pembrolizumab monotherapy superior for CPS ≥20 |
| PD-L1 biomarker | CPS (combined positive score) ≥1 required for first-line monotherapy; ≥20 predicts best response |
| HNSCC PD-L1 expression | 45-80% of HNSCCs express PD-L1 |
| Side effects | Immune-related adverse events (irAEs): pneumonitis, colitis, hepatitis, endocrinopathies (hypothyroidism, adrenal insufficiency), skin rash; pseudoprogression can occur |
3. Nivolumab (Opdivo®) - Anti-PD-1 Checkpoint Inhibitor
| Feature | Detail |
|---|---|
| Type | Human IgG4 antibody |
| Target | PD-1 |
| FDA approval | Recurrent/metastatic HNSCC after platinum failure (2016) |
| Key trial - CheckMate 141 | Nivolumab vs. investigator's choice (cetuximab/methotrexate/docetaxel) in platinum-refractory r/m-HNSCC: OS 7.5 vs 5.1 months (p<0.01); grade 3-4 toxicities 13% vs 35% |
| Advantage | Markedly lower toxicity than chemotherapy while achieving superior OS |
4. Panitumumab - Anti-EGFR (Fully Human)
- Fully human IgG2 anti-EGFR antibody (less ADCC than cetuximab due to IgG2 isotype)
- Phase III trial (657 patients): panitumumab + cisplatin/5-FU vs. chemotherapy alone: improved PFS (5.8 vs 4.6 months, p=0.004) but no significant OS improvement
- Less infusion reaction risk than cetuximab (fully human)
- Better OS in HPV-negative (p16-negative) HNSCC (11.6 vs 8.6 months)
5. Ipilimumab (Yervoy®) - Anti-CTLA-4
- Blocks CTLA-4 on regulatory T cells → promotes T-cell activation against tumour
- Used in combination with nivolumab in recurrent/metastatic HNSCC (investigational)
- CTLA-4 inhibition = more systemic, broader immune activation than PD-1 blockade
- Higher irAE rates than PD-1 inhibitors
ENT Application 3: Recurrent Respiratory Papillomatosis (RRP)
Bevacizumab (Avastin®) - Anti-VEGF
| Feature | Detail |
|---|---|
| Target | VEGF (vascular endothelial growth factor) |
| Mechanism | Inhibits VEGF-driven angiogenesis; HPV-driven papillomas depend on neovascularisation for growth; bevacizumab disrupts this |
| Route in RRP | Intralesional injection (25-50 mg per session, subepithelial injection after KTP/angiolytic laser ablation) |
| Half-life | ~1 month |
| Systemic route | IV infusion also used for aggressive/disseminated RRP |
| Evidence | Multiple case series showing reduced frequency of surgery and extent of recurrence; some patients achieve disease remission |
| Technique | After office-based angiolytic laser ablation, bevacizumab injected into superficial lamina propria at papilloma sites (25 mg/mL, 25-50 mg) |
| Benefit | Reduces number of procedures per year; some patients have total disease eradication |
ENT Application 4: Allergic Rhinitis
Omalizumab (Additional Role)
- Anti-IgE mechanism is directly applicable to allergic rhinitis (IgE-mediated)
- Reduces mast cell and basophil response to allergen
- Useful in patients with severe allergic rhinitis comorbid with asthma and/or CRSwNP
- Not first-line for isolated allergic rhinitis (antihistamines + nasal steroids preferred), but relevant in step-up/refractory disease
- The EXTRA study showed greatest benefit in patients with high FeNO, high serum eosinophils, and elevated periostin
ENT Application 5: Eosinophilic Granulomatosis with Polyangiitis (EGPA / Churg-Strauss)
- ENT manifestations: nasal polyps, sinusitis, granulomatous nasal obstruction, subglottic stenosis
- Mepolizumab (anti-IL-5): FDA-approved for EGPA; reduces eosinophilic inflammation; reduces steroid dependence; reduces ENT flares
- IL-5 drives eosinophil survival in EGPA - blocking it is pathophysiologically logical
Application 6: Nasopharyngeal Carcinoma (NPC)
- NPC overexpresses EGFR and PD-L1
- Cetuximab studied in combination with radiotherapy and chemotherapy
- Pembrolizumab and nivolumab evaluated in recurrent/metastatic NPC (PD-L1 highly expressed)
- EBV-associated NPC shows immune evasion through PD-L1 upregulation - rationale for checkpoint inhibitors
Key Concepts: Immune Checkpoints in HNSCC
- PD-1 is expressed on activated T cells; its ligand PD-L1 is on tumour cells and APCs
- Tumour cells upregulate PD-L1 (stimulated by IFN-γ) → binds PD-1 on T cells → T-cell exhaustion → tumour immune escape
- Anti-PD-1 antibodies (pembrolizumab, nivolumab) block this interaction → restore T-cell killing
- CTLA-4 expressed on regulatory T cells; binds B7 on APCs → downregulates T-cell activation
- Ipilimumab blocks CTLA-4 → removes T-cell suppression → more potent but more toxic immune activation
- MDSCs, tolerogenic DCs, TGF-β, IL-6 secretion all contribute to immune evasion
- Immunoediting: elimination → equilibrium → escape (tumour evades immune system)
- Pseudoprogression: tumour appears larger initially due to immune infiltration - must confirm progression 4 weeks later before stopping therapy (irRC criteria)
Adverse Effects - Summary
| Drug | Key Adverse Effects |
|---|---|
| Cetuximab | Acneiform rash, hypomagnesaemia, infusion reactions, paronychia |
| Pembrolizumab/Nivolumab | irAEs: pneumonitis, colitis, hepatitis, thyroiditis, hypophysitis, skin rash; rarely myocarditis |
| Dupilumab | Conjunctivitis, injection site reactions, paradoxical eosinophilia |
| Omalizumab | Injection site reactions; rare anaphylaxis (observe 30 min post-injection) |
| Mepolizumab/Benralizumab | Generally well tolerated; injection site reactions; headache |
| Bevacizumab | Hypertension, proteinuria, wound healing impairment, thromboembolic events, nasal septal perforation (systemic) |
Summary Table: mAbs in ENT
| Drug | Target | ENT Indication | Route | Approval |
|---|---|---|---|---|
| Dupilumab | IL-4Rα (IL-4/IL-13) | CRSwNP | SC q2w | FDA approved (CRSwNP 2019) |
| Omalizumab | IgE (FcεRI binding site) | CRSwNP, allergic rhinitis | SC q2-4w | FDA approved (CRSwNP 2020) |
| Mepolizumab | IL-5 | CRSwNP, EGPA | SC q4w | FDA approved (EGPA 2017) |
| Benralizumab | IL-5Rα | CRSwNP (eosinophilic) | SC q4-8w | Investigational for CRSwNP |
| Tezepelumab | TSLP | CRSwNP (emerging) | SC q4w | Investigational |
| Cetuximab | EGFR | HNSCC (oropharynx, larynx, NPC) | IV | FDA approved |
| Pembrolizumab | PD-1 | Recurrent/metastatic HNSCC | IV q3w | FDA approved (2016/2019) |
| Nivolumab | PD-1 | Recurrent/metastatic HNSCC | IV | FDA approved (2016) |
| Panitumumab | EGFR | HNSCC (r/m) | IV | Investigated |
| Bevacizumab | VEGF | RRP (intralesional) | Intralesional / IV | Off-label in RRP |
Key Points
- mAbs are single-clone antibodies targeting one specific epitope; named by source suffix (-ximab = chimeric, -zumab = humanized, -umab = fully human)
- In CRSwNP: Type 2/eosinophilic inflammation drives disease; dupilumab (anti-IL-4/IL-13) is FDA-approved first-line biologic; omalizumab (anti-IgE) also approved; mepolizumab/benralizumab target IL-5 pathway; tezepelumab targets upstream TSLP
- Biomarker-guided biologic selection: IgE → omalizumab; eosinophilia → mepolizumab/benralizumab; Th2/mixed → dupilumab
- In HNSCC: EGFR overexpressed in >90% - cetuximab (chimeric anti-EGFR) used with RT (Bonner trial) and chemotherapy (EXTREME trial)
- Checkpoint inhibitors: PD-L1 expressed on 45-80% of HNSCCs; pembrolizumab + chemotherapy now first-line for r/m-HNSCC (KEYNOTE-048); nivolumab approved post-platinum failure (CheckMate 141: OS 7.5 vs 5.1 months)
- RRP: bevacizumab (anti-VEGF, 25-50 mg intralesional) reduces papilloma angiogenesis, decreases surgical frequency, can achieve remission
- EGPA: mepolizumab approved; addresses eosinophilic ENT manifestations including nasal polyps and subglottic stenosis
- irAEs from checkpoint inhibitors are distinct from cytotoxic chemotherapy toxicities and require early recognition and steroid treatment
Surgical anatomy of thyroid
"thyroid" "surgical anatomy" "recurrent laryngeal nerve" parathyroid
Surgical Anatomy of the Thyroid Gland
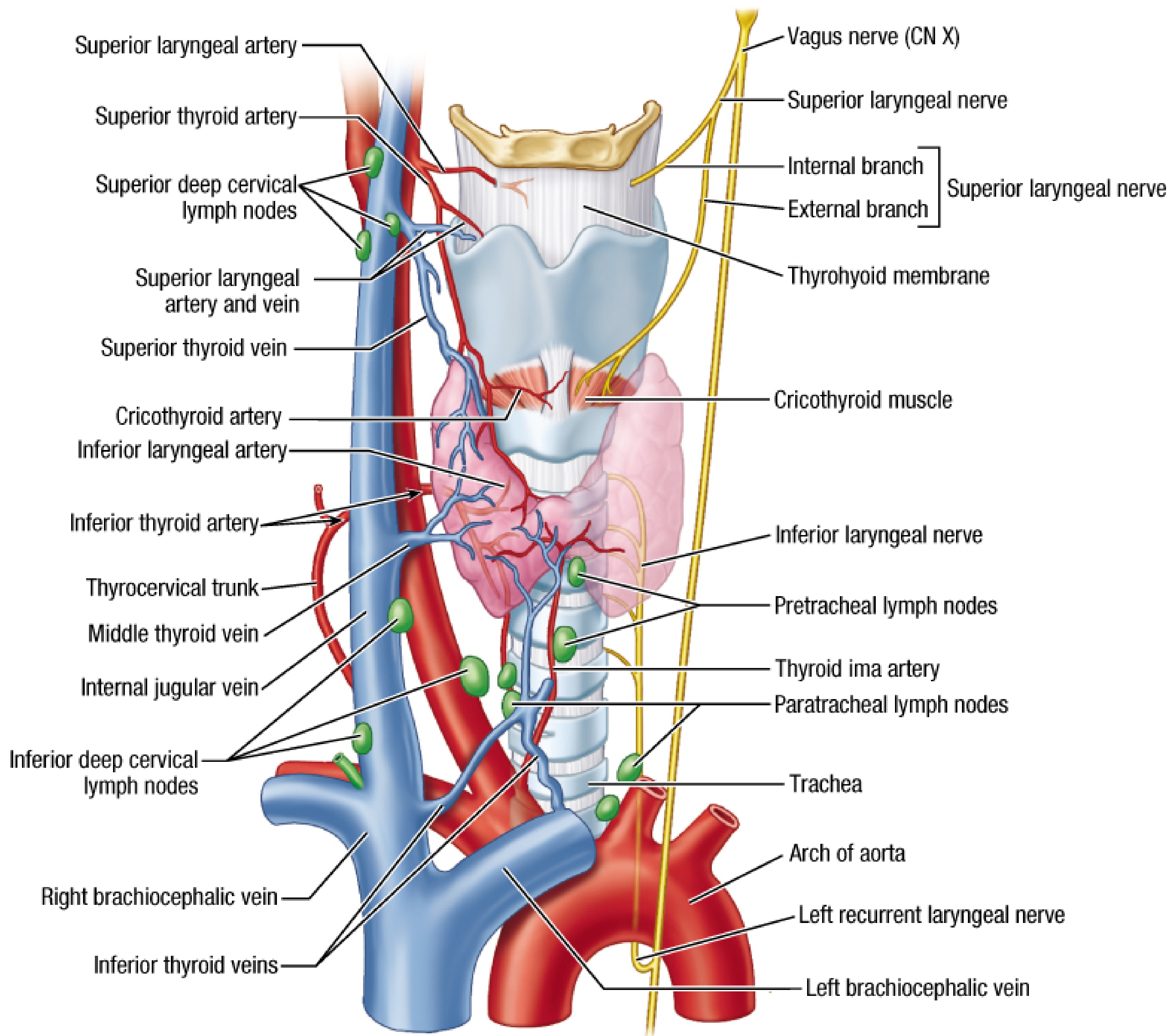
1. Embryology (Surgical Relevance)
Median Thyroid Anlage
- Originates as endodermal thickening at the foramen cecum (base of tongue, junction of anterior 2/3 and posterior 1/3) at ~4 weeks gestation
- Descends caudally, initially connected to tongue by the thyroglossal duct
- By week 5, duct becomes solid; by week 7, duct fragments and disappears
- Thyroid reaches its final position anterior to the trachea by week 7
- Foramen cecum remains at base of tongue; pyramidal lobe may persist as distal remnant
Lateral Thyroid Anlage
- Arises from caudal pharyngeal endoderm and 4th-5th pharyngeal pouches (ultimobranchial bodies)
- Fuses with median anlage during descent
- Source of parafollicular C cells (calcitonin-secreting)
- Forms approximately one-third of total thyroid mass
- Point of fusion = Tubercle of Zuckerkandl
Surgical Implications of Embryology
| Anomaly | Mechanism | Clinical / Surgical Significance |
|---|---|---|
| Thyroglossal duct cyst | Failure of duct to completely resorb | Midline neck mass moving with tongue protrusion; Rx = Sistrunk procedure (excision of cyst + thyroglossal duct + central hyoid) |
| Lingual thyroid | Failure of median anlage to descend | Mass at tongue base; may be only functioning thyroid - must exclude before removal |
| Pyramidal lobe | Persistence of distal thyroglossal tract | Present in ~60%; must be removed in thyroidectomy to prevent residual functioning tissue |
| Ectopic thyroid | Arrest along descent path | Sublingual, substernal, intrathoracic, intrathymic, cardiac |
| Aberrant right subclavian artery | Developmental anomaly of aortic arch | Predicts non-recurrent laryngeal nerve on the right (0.3-1.6%) |
2. Gross Anatomy and Relations
Dimensions
- Weight: 15-30 g (normal)
- Each lobe: ~5 cm craniocaudal × 2-3 cm AP × 3 cm wide
- Isthmus: overlies 2nd-4th tracheal rings
- Lobes extend superiorly over lateral aspects of thyroid cartilage
Position
- Anterior to the trachea, just inferior to the cricoid cartilage, within the central compartment of the neck
Fascial Investment
- Invested by pretracheal fascia - forms an easily mobilised dissection plane (unless thyroiditis or invasive malignancy present)
- Anteriorly: anterior suspensory ligament above isthmus
- Posteromedially: condensation of pretracheal fascia forms the ligament of Berry (lateral ligament / posterior suspensory ligament)
Relations
| Direction | Structures |
|---|---|
| Anterior | Strap muscles: sternothyroid (deep), sternohyoid (superficial), and omohyoid laterally |
| Posterior (medial) | Trachea and oesophagus (oesophagus particularly on the left) |
| Lateral | Carotid sheath (common carotid artery, internal jugular vein, vagus nerve) |
| Posterolateral | Parathyroid glands |
| Posterior deep | Recurrent laryngeal nerves in tracheo-oesophageal groove |
3. Ligament of Berry (Posterior Suspensory Ligament)
- Formed from condensed pretracheal fascia
- Located just caudal to the cricoid cartilage - forms firm lateral attachment of thyroid to trachea
- Traversed by:
- Small branch of inferior thyroid artery
- Small venous branches from thyroid
- Recurrent laryngeal nerve (most vulnerable here)
- The RLN may run anterior, posterior, or within the substance of this ligament
- Most dangerous step in thyroidectomy - RLN most at risk at this fixed point
4. Tubercle of Zuckerkandl
- A lateral/posterior projection of the middle third of the thyroid lobe
- Present in up to 60% of surgical dissections
- Represents the embryologic fusion point between the ultimobranchial body and the median thyroid anlage
Threefold Surgical Importance:
- RLN runs medial to it (most often) - the tubercle points toward the nerve
- Superior parathyroid gland is usually attached to its cranial aspect
- When enlarged (in goitre), significant thyroid tissue may be inadvertently left behind if subtotal thyroidectomy is performed
5. Arterial Supply
Superior Thyroid Artery
- Usually first branch of the external carotid artery
- Runs anteroinferiorly deep to infrahyoid muscles to the superior pole
- Divides into anterior branch (along anterior border) and posterior branch (posterior surface)
- Also gives: superior laryngeal branch (accompanies internal branch of SLN through thyrohyoid membrane) and cricothyroid branch
- The external branch of the SLN runs close to the superior thyroid vessels at the superior pole - at risk during superior pole ligation
Inferior Thyroid Artery
- Branch of the thyrocervical trunk (from subclavian artery)
- Courses superiorly over scalenus anterior, then crosses medially posterior to carotid sheath
- Reaches posterior thyroid gland near the RLN (variable relationship - see below)
- Gives small branches to both superior and inferior parathyroid glands - it is the primary blood supply to both
- Critical: ligating close to the thyroid capsule (not main trunk) preserves parathyroid blood supply
Thyroid Ima Artery
- Present in 8-10% of individuals
- Arises from brachiocephalic artery, aortic arch, right common carotid, internal thoracic, or subclavian artery
- Ascends anterior to the trachea to supply the inferior thyroid isthmus
- Can cause significant unrecognised blood loss during thyroidectomy or tracheostomy
6. Venous Drainage
| Vein | Drainage |
|---|---|
| Superior thyroid vein | Internal jugular vein (ipsilateral) |
| Middle thyroid vein | Internal jugular vein (ipsilateral); may be absent or duplicated; torn if thyroid medialized without first dividing it |
| Inferior thyroid vein | Brachiocephalic vein (right and left); may join to form a thyroidea ima vein draining to left brachiocephalic |
7. The Recurrent Laryngeal Nerve (RLN) - Most Critical Structure
Origin and Course
| Side | Origin | Loop | Course to Larynx |
|---|---|---|---|
| Right RLN | Right vagus at level of right subclavian artery | Loops around right subclavian artery | More oblique course; ascends laterally before entering tracheo-oesophageal groove |
| Left RLN | Left vagus at arch of aorta (posterior to ligamentum arteriosum) | Loops around aortic arch | More vertical; ascends in tracheoesophageal groove throughout neck |
- Both nerves enter the larynx at the caudal aspect of the cricothyroid muscle (cricotracheal junction)
- The inferior laryngeal nerve (terminal branch) is the motor branch supplying all intrinsic laryngeal muscles except cricothyroid
- Other branches are sensory to pharynx and subglottis
Relationship to Inferior Thyroid Artery
- The RLN crosses the inferior thyroid artery at variable points - the artery may pass:
- Anterior to the nerve
- Posterior to the nerve
- Between branches of the nerve (most dangerous - can be mistaken for a vessel)
- Identified most reliably near the cricoid cartilage at the ligament of Berry
Branching Before Laryngeal Entry
- Up to 34% of RLNs branch before insertion
- Motor fibres: anterior branch
- Sensory fibres: posterior branch
- Injury to posterior sensory branch → aspiration (even without hoarseness)
Non-Recurrent Laryngeal Nerve (NRLN)
| Feature | Right | Left |
|---|---|---|
| Incidence | 0.3-1.6% of thyroid operations | Extremely rare (<0.04%) |
| Associated anomaly | Aberrant right subclavian artery (lusoria) arising from aorta | Right-sided aortic arch (situs inversus) |
| Clinical clue | Absent brachiocephalic trunk on preoperative CT/ultrasound | - |
| Risk | Course from vagus directly to larynx without looping = encountered earlier and higher than expected |
Consequences of RLN Injury
- Unilateral: Ipsilateral vocal cord palsy → hoarseness, breathy voice, aspiration risk
- Bilateral: Bilateral vocal cord palsy in adducted position → stridor, respiratory distress, emergency surgical airway required
8. Superior Laryngeal Nerve (SLN) - External Branch (EBSLN)
Origin and Course
- Arises from the vagus near the skull base as the superior laryngeal nerve
- Travels along internal carotid artery, then divides at level of hyoid cornu into:
- Internal branch: sensory to supraglottic mucosa; pierces thyrohyoid membrane; may anastomose with RLN sensory branches (loop of Galen)
- External branch: motor to cricothyroid muscle (and inferior constrictor) → responsible for vocal pitch and projection (high notes, projection)
Cernea Classification (Surgical Risk)
| Type | Position relative to superior thyroid vessels | Risk |
|---|---|---|
| Type 1 | Crosses >1 cm above upper border of superior pole | Low risk |
| Type 2a | Crosses within 1 cm of upper border | Moderate risk |
| Type 2b | Crosses below the upper border of the superior pole | Highest risk |
Consequence of EBSLN Injury
- Loss of cricothyroid function → inability to tense vocal cord → loss of high pitch notes and projection; particularly devastating in singers/professional voice users
9. Parathyroid Glands
Overview
- Usually 4 glands (2 superior + 2 inferior); may be 2-8 in number
- Colour: tan/yellow-brown, slightly darker than thyroid and lighter than fat
- Size: 3-6 mm; weight ~30-40 mg each
- Blood supply: primarily from inferior thyroid artery (both superior and inferior glands); superior may receive accessory branches from superior thyroid artery
- Key: Ligation of inferior thyroid artery close to thyroid capsule (not the main trunk) preserves parathyroid vascularity
Superior Parathyroid Glands
- Derived from 4th pharyngeal pouch (with lateral thyroid anlage)
- More constant in position
- Located on posterior surface of upper thyroid lobe, near the junction of upper and middle thirds
- Often at the level of the cricoid cartilage, just above the inferior thyroid artery
- Typically attached to the cranial aspect of the tubercle of Zuckerkandl
- Covered by thin fascial layer outside the thyroid capsule
Inferior Parathyroid Glands
- Derived from 3rd pharyngeal pouch (with thymus)
- More variable in position (travel further with the thymus)
- Usually located near the lower pole of the thyroid or on its posterior surface
- May be found anywhere from the angle of the jaw to the anterior mediastinum (within the thymus)
Surgical Preservation
- Identify by colour and texture difference from thyroid, fat, and lymph nodes
- Preserve fascial pedicle with inferior thyroid artery branches
- If devascularised: autotransplantation into sternomastoid muscle
10. Lymphatic Drainage (Surgical Staging)
Central Compartment (Level VI and VII)
- Includes: prelaryngeal (Delphian), pretracheal, and paratracheal nodes
- Boundaries: hyoid superiorly, innominate artery inferiorly, carotid sheaths laterally
- Level VI vs. VII: divided at the sternal notch
- Delphian node: prelaryngeal, on anterior suspensory ligament/isthmus; first node encountered; when positive = adverse pathologic characteristics
Lateral Compartment (Levels I-V)
- Level II (upper jugular), III (mid-jugular), IV (lower jugular), V (posterior triangle)
- Thyroid cancer spreads to central compartment first, then lateral
- "Skip" metastases to lateral only reported, particularly from superior pole tumours
Intracapsular Channels
- Rich intracapsular lymph plexus provides communication across isthmus and between lobes - relevant to bilateral lymph node metastasis
11. Fascial Layers and Surgical Planes
| Layer | Surgical Significance |
|---|---|
| Pretracheal fascia | Invests thyroid; easily mobilised plane in normal anatomy |
| Anterior suspensory ligament | Above isthmus; condensed pretracheal fascia |
| Ligament of Berry | Posteromedial; firm tracheal attachment; RLN at risk here |
| Carotid sheath | Lateral border of dissection |
| Strap muscle fascia | Divided in midline raphe for access |
12. Strap Muscles (Covering Structures)
- Platysma (most superficial)
- Investing cervical fascia
- Sternohyoid (superficial strap - divided in midline)
- Omohyoid (lateral strap)
- Sternothyroid (deep strap - directly on thyroid capsule)
13. Key Surgical Landmarks Summary
| Landmark | Significance |
|---|---|
| Ligament of Berry | RLN most vulnerable here; posteromedial tracheal attachment |
| Tubercle of Zuckerkandl | RLN runs medial to it; superior parathyroid attached cranially |
| Inferior thyroid artery | Primary blood supply to parathyroids; variable RLN relationship |
| Superior thyroid artery | EBSLN at risk during superior pole ligation |
| Cricoid cartilage | Level at which RLN enters larynx (cricotracheal junction) |
| Tracheo-oesophageal groove | Course of left RLN; right RLN enters groove more obliquely |
| Delphian node | Prelaryngeal; harbinger of malignancy |
| Thyroid ima artery | Present in 10%; anterior to trachea; must identify to avoid haemorrhage |
| Middle thyroid vein | Divided before medial thyroid mobilisation |
| Foramen cecum | Origin of thyroglossal duct at tongue base |
14. Key Points Summary
- Thyroid = bilobed gland, 15-30g, anterior to trachea at C5-T1; invested by pretracheal fascia
- Embryology: median anlage (foramen cecum) + lateral anlage (4th/5th pouches) fuse at tubercle of Zuckerkandl; C cells from lateral anlage
- Pyramidal lobe present in ~60% - must be removed to avoid residual functioning tissue
- Blood supply: superior thyroid artery (from ECA) + inferior thyroid artery (from thyrocervical trunk); thyroid ima artery in 10%
- Venous drainage: superior + middle (to IJV) + inferior (to brachiocephalic vein)
- RLN: right loops around subclavian (oblique course); left loops around aortic arch (vertical); enters larynx at cricotracheal junction; most vulnerable at ligament of Berry; non-recurrent on right in 0.3-1.6% (associated with aberrant subclavian artery); 34% branch before entry (motor anterior, sensory posterior)
- EBSLN (Cernea classification): Type 2b (below superior pole level) = highest injury risk; injury → loss of high pitch/projection
- Parathyroids: superior from 4th pouch (more constant), inferior from 3rd pouch (more variable); both primarily supplied by inferior thyroid artery; preserve by ligating ITA branches close to capsule
- Tubercle of Zuckerkandl: RLN runs medial; superior parathyroid cranially attached; goitre may hide residual tissue
- Lymphatics: central (VI/VII) → lateral (II-V); Delphian node = prelaryngeal harbinger node
Anatomy of cavernous sinus and its clinical importance in ENT
"cavernous sinus thrombosis" sinusitis otolaryngology
Anatomy of the Cavernous Sinus and Its Clinical Importance in ENT
1. Definition and Overview
- It lies immediately lateral to the sphenoid sinus - directly at risk from sphenoid sinusitis
- Multiple critical cranial nerves and vessels pass through or within its walls
- It drains the face, nose, sinuses, and orbit - allowing spread of infection to the intracranial compartment
2. Location and Boundaries
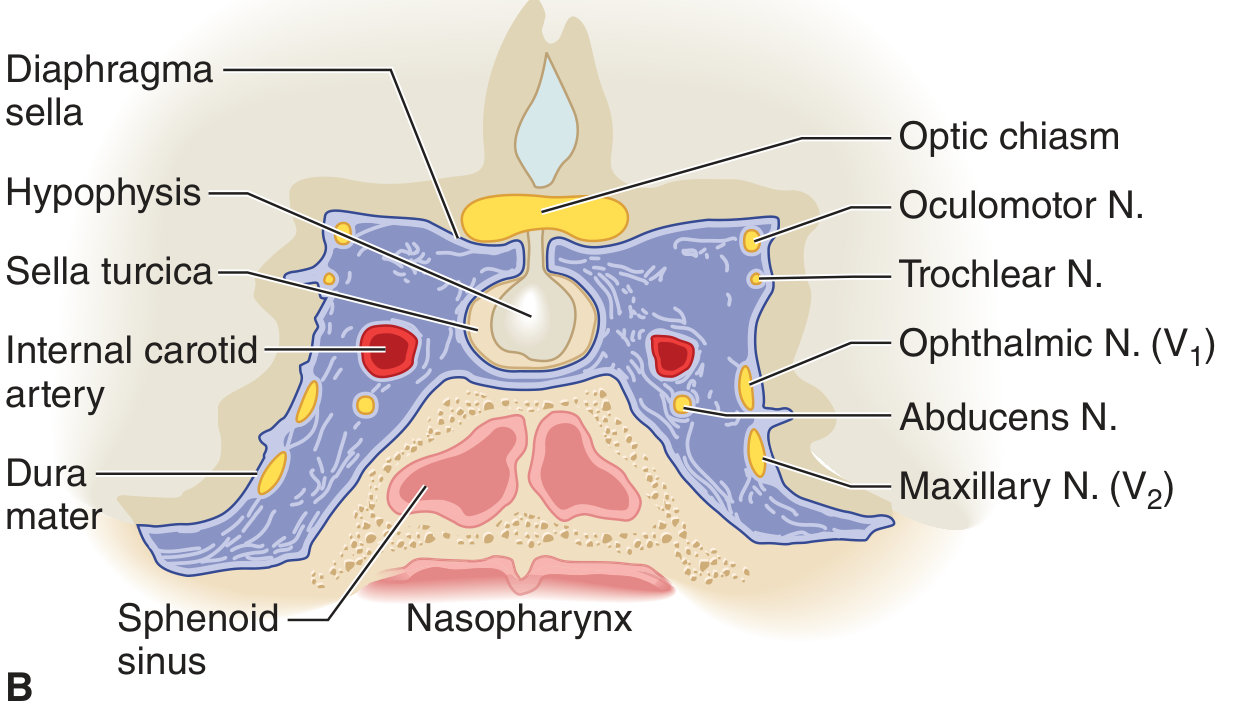
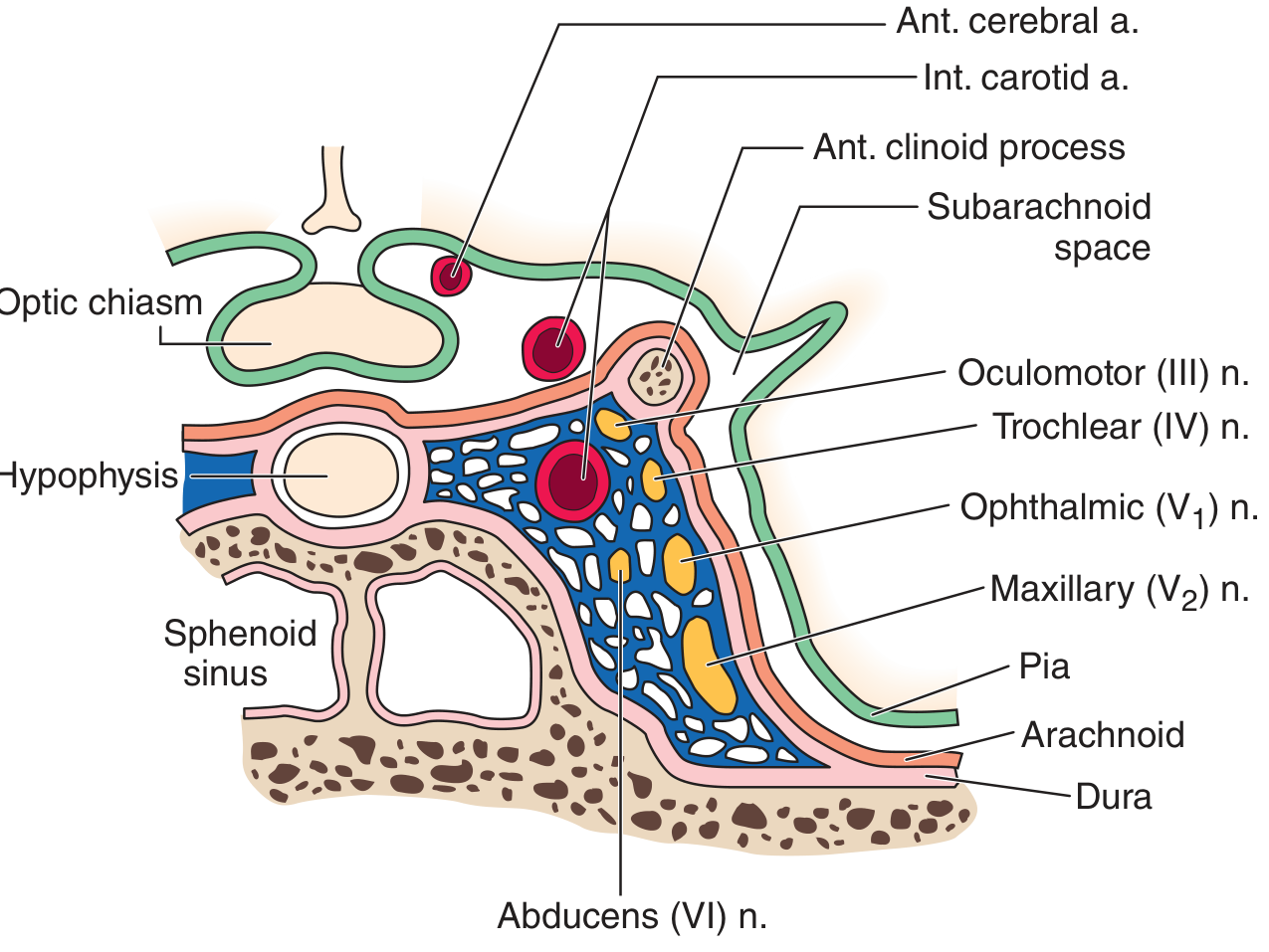
Boundaries
| Wall | Relations |
|---|---|
| Superior | Diaphragma sellae; optic chiasm (above/anterior) |
| Inferior | Floor of middle cranial fossa; apex of petrous bone |
| Medial | Body of sphenoid (lateral wall of sphenoid sinus); pituitary gland / sella turcica |
| Anterior | Superior orbital fissure; medial end of lesser sphenoid wing |
| Posterior | Apex of petrous temporal bone; dorsum sellae |
| Lateral | Two-layered dural lateral wall (contains CN III, IV, V1, V2) |
3. Contents
Structures WITHIN the Sinus (in the trabecular venous space)
| Structure | Position | Note |
|---|---|---|
| Internal carotid artery (ICA) | Central / medial part of sinus | Surrounded by venous blood; accompanied by sympathetic plexus (from SCG) |
| CN VI (Abducens nerve) | Free within the sinus, inferior and medial to ICA | Most vulnerable CN within sinus - damaged first by raised ICA pressure (aneurysm/fistula) |
| Sympathetic plexus | Around ICA | Damage → Horner syndrome |
Structures in the LATERAL WALL of the Sinus (between two dural layers, from superior to inferior)
| Nerve | Position | Function |
|---|---|---|
| CN III (Oculomotor) | Superior in lateral wall | All extraocular movements except SO and LR; pupil constriction |
| CN IV (Trochlear) | Below CN III in lateral wall | Superior oblique muscle |
| CN V1 (Ophthalmic division) | Below CN IV in lateral wall | Sensory: forehead, cornea, upper eyelid, nose tip |
| CN V2 (Maxillary division) | Lowest in lateral wall | Sensory: cheek, upper lip, upper teeth, lower eyelid; exits via foramen rotundum |
- CN III, IV, V1, V2 are in the lateral wall (protected by dural folds)
- CN VI is free within the sinus - most exposed nerve, earliest affected by pressure changes
4. Venous Connections (Drainage Routes - Key for ENT)
Tributaries (Inflow to Cavernous Sinus)
| Vein | Source | ENT Relevance |
|---|---|---|
| Superior ophthalmic vein | Orbit, upper face, angular/supraorbital veins | Main route for facial/orbital infection to cavernous sinus |
| Inferior ophthalmic vein | Orbit, lower eyelid | Secondary route; drains also to pterygoid plexus |
| Sphenoparietal sinus | Along underside of lesser wing of sphenoid | Drains anterior middle fossa |
| Middle cerebral (superficial) veins | Lateral cerebral cortex | - |
| Basilar venous plexus | Crosses clivus | Connects to opposite cavernous sinus and vertebral plexus |
| Pterygoid venous plexus | Via emissary veins through foramen ovale and foramen lacerum | Connects nasopharynx, PTF, deep facial infections to cavernous sinus |
| Angular vein → facial vein → ophthalmic vein | Face/nasal tip/upper lip | "Danger triangle of face" route |
Efferent Drainage from Cavernous Sinus
| Vein | Destination |
|---|---|
| Superior petrosal sinus | Transverse sinus → sigmoid sinus → IJV |
| Inferior petrosal sinus | Directly to jugular bulb/IJV |
| Intercavernous (circular) sinus | Connects to contralateral cavernous sinus (around pituitary) - explains bilateral spread |
| Basilar plexus | Across clivus to contralateral side |
5. Danger Triangle of the Face and Routes of Spread to Cavernous Sinus
Route 1: Via Ophthalmic Vein (Main Route)
Facial infection → Angular vein → Superior ophthalmic vein → Cavernous sinus
- The angular vein (at medial canthus) is the origin of the facial vein
- Has anastomoses with the superior ophthalmic vein (no valves)
- Infection from nasal tip, upper lip, or face travels via this valveless system
Route 2: Via Pterygoid Plexus
Deep facial vein / nasal/nasopharyngeal veins → Pterygoid plexus → Emissary veins through foramen ovale/lacerum → Cavernous sinus
Route 3: Direct Extension from Sphenoid Sinus
- The lateral wall of the sphenoid sinus is directly the medial wall of the cavernous sinus
- Sphenoid sinusitis → bone erosion / direct mucosal spread → cavernous sinus
6. Clinical Syndromes of ENT Importance
A. Cavernous Sinus Thrombosis (CST)
| Source | Organism | Route |
|---|---|---|
| Facial furunculosis/carbuncle (danger triangle) | Staphylococcus aureus | Angular vein → ophthalmic vein |
| Orbital cellulitis/abscess | S. aureus, streptococci | Direct extension, superior ophthalmic vein |
| Sphenoid sinusitis | Mixed, gram-negatives | Direct lateral wall extension |
| Ethmoid sinusitis | Streptococcus, Haemophilus | Via orbital veins |
| Maxillary sinusitis | Mixed | Pterygoid plexus route |
| Dental sepsis | Mixed anaerobes | Pterygoid plexus |
| Mucormycosis (in diabetics) | Rhizopus/Mucor spp. | Angioinvasive - direct extension from nose/sinuses; rapidly fatal |
| Nasopharyngeal infection | Mixed | Pterygoid plexus |
| Feature | Explanation |
|---|---|
| Fever, rigors, toxaemia | Sepsis |
| Severe headache, retro-orbital pain | V1 involvement, venous hypertension |
| Proptosis (exophthalmos) | Obstruction of superior ophthalmic vein → orbital venous hypertension |
| Chemosis (conjunctival oedema) | Impaired orbital venous drainage |
| Periorbital oedema | Venous congestion |
| Ophthalmoplegia | CN III, IV, VI palsy → complete ophthalmoplegia |
| CN VI palsy | First nerve affected - lateral rectus palsy → failure of lateral gaze (convergent squint) |
| CN V1 sensory loss | Forehead/corneal hypoaesthesia |
| V2 involvement | Cheek numbness (maxillary division) |
| Papilloedema / visual loss | Raised intracranial venous pressure; optic nerve compression |
| Retinal venous engorgement | Impaired retinal venous drainage |
| Meningism | Meningeal irritation/meningitis |
| Bilateral signs | Intercavernous sinus allows contralateral spread - hallmark feature |
- MRI with contrast + MR venography (gold standard): filling defect in cavernous sinus, loss of normal signal void
- CT with contrast: shows abnormal enhancement, filling defects
- Blood cultures: positive in 70% of septic cases
- Lumbar puncture (if no contraindication): may show pleocytosis
- FBC: leucocytosis
- Broad-spectrum IV antibiotics (cover S. aureus including MRSA - vancomycin + 3rd/4th generation cephalosporin; add metronidazole for anaerobes)
- Antifungal therapy (amphotericin B) if mucormycosis suspected
- Surgical drainage of primary source (sinus surgery for sphenoid/ethmoid sinusitis, orbital decompression)
- Anticoagulation (heparin): controversial but meta-analysis (PMID 39312001, 2025, Eur Arch Otorhinolaryngol) suggests benefit in reducing mortality and improving neurological outcomes
- Corticosteroids: for associated pituitary insufficiency or severe inflammation
- No role for steroids in infectious CST routinely
B. Cavernous Sinus Syndrome
| Deficit | Nerve | Clinical Feature |
|---|---|---|
| Ophthalmoplegia | CN III, IV, VI | Loss of all ocular movements |
| Ptosis | CN III (levator) | Drooping upper eyelid |
| Fixed dilated pupil | CN III (parasympathetics) | Mydriasis, no light reflex |
| Forehead/corneal sensory loss | CN V1 | Anaesthesia of upper face |
| Cheek sensory loss | CN V2 | If V2 involved |
| Horner syndrome | Sympathetic plexus around ICA | Ptosis + miosis + anhidrosis (may be masked by CN III ptosis) |
| Proptosis | Venous obstruction | Exophthalmos |
| Chemosis | Venous congestion | Conjunctival oedema |
C. Cavernous-Carotid Fistula (CCF)
- Abnormal communication between ICA and cavernous sinus (traumatic or spontaneous)
- Results in high-pressure arterialised blood in the cavernous sinus
- CN VI (free within sinus, adjacent to ICA) affected first
- Features: pulsatile exophthalmos, orbital bruit (audible on auscultation), chemosis, ophthalmoplegia
- ENT relevance: may follow skull base fractures involving the sphenoid
D. Sphenoid Sinusitis and Cavernous Sinus
- The lateral wall of the sphenoid sinus is the medial wall of the cavernous sinus
- Bony impressions of the ICA and optic nerve are commonly visible in well-pneumatised sphenoid sinuses and may be dehiscent (no bone separating from cavernous sinus)
- Isolated sphenoid sinusitis can present with:
- Retro-orbital/vertex headache
- CN VI palsy (abducens palsy - diplopia on lateral gaze)
- CN V1/V2 sensory changes
- Signs of CST if thrombosis supervenes
E. Skull Base Tumour Extension
| Primary | Route of Spread | Clinical Result |
|---|---|---|
| Nasopharyngeal carcinoma | Foramen lacerum → cavernous sinus, or direct perineural along V3 → Gasserian ganglion → cavernous sinus | Multiple CN palsies (Villaret/Collet-Sicard); cavernous sinus syndrome |
| Juvenile nasopharyngeal angiofibroma | Via pterygopalatine fossa → infratemporal fossa → middle cranial fossa | Cavernous sinus invasion |
| Sinonasal malignancy | Direct extension through skull base | Cavernous sinus invasion |
| Pituitary tumour | Lateral extension from sella | Cavernous sinus syndrome |
| Meningioma | Sphenoidal ridge, cavernous sinus | CN III, IV, VI, V1/V2 involvement |
F. Tolosa-Hunt Syndrome
- Idiopathic granulomatous inflammation of the cavernous sinus and/or superior orbital fissure
- Presents with: severe periorbital pain + ophthalmoplegia (CN III, IV, VI) + V1/V2 sensory loss
- Diagnosis of exclusion (must rule out infection, tumour, sarcoid, lymphoma, IgG4 disease)
- Dramatic response to corticosteroids within days (oral prednisone 60 mg/day) is characteristic
- MRI shows enhancing soft tissue in cavernous sinus/superior orbital fissure
- Harrison's 22E, p. 1492
7. Surgical Anatomy (ENT Skull Base Surgery)
- The cavernous sinus is directly at risk during endoscopic skull base surgery (transsphenoidal approach, pituitary surgery, clivus resection)
- The ICA runs in bony canals forming lateral impressions on the sphenoid sinus walls - frequently dehiscent in well-pneumatised sinuses
- The optic nerve (CN II) runs in the superolateral sphenoid wall, just above the ICA
- Cummings: endoscopic view after sphenoid sinus wall removal shows "cavernous sinus and its contents (CN III, IV, V, and VI)" at position 7 around the ICA at position 2
- ICA injury (catastrophic haemorrhage)
- CN VI palsy (diplopia)
- CN III/IV palsy (ophthalmoplegia)
- Pituitary damage (hypopituitarism)
- CSF leak
8. Radiological Assessment
| Modality | Use |
|---|---|
| MRI with Gd (gold standard) | Filling defect, abnormal enhancement, thrombus signal (no flow void) |
| MR venography | Direct visualisation of sinus thrombosis |
| CT + contrast | Bony erosion, sinus opacification, ring-enhancing collections |
| CT angiography | ICA position, CCF, aneurysm |
| Ophthalmology | Fundoscopy (papilloedema, retinal venous engorgement) |
9. Key Points Summary
- Cavernous sinus = paired trabeculated dural venous sinus at base of skull, lateral to sphenoid sinus and sella
- Contents: ICA + CN VI within sinus; CN III, IV, V1, V2 in lateral wall (superior to inferior)
- CN VI is most exposed → first nerve affected by pressure (aneurysm, CCF) and in early CST
- Venous connections (all valveless): superior ophthalmic vein, inferior ophthalmic vein, pterygoid plexus, sphenoparietal sinus, basilar plexus, intercavernous sinus
- Routes of spread to cavernous sinus from ENT sites: (1) Angular vein → ophthalmic vein; (2) Deep facial vein → pterygoid plexus → foramen ovale/lacerum; (3) Direct sphenoid sinus extension
- Danger triangle = nasal tip to corners of mouth; infections here can track to cavernous sinus
- CST: septic (most common - S. aureus, mucormycosis in diabetics) or aseptic; features = bilateral proptosis + chemosis + ophthalmoplegia + fever; treat with IV antibiotics + source control ± anticoagulation
- Cavernous sinus syndrome: complete = total ophthalmoplegia + fixed dilated pupil + V1/V2 sensory loss + Horner syndrome
- Orbital apex syndrome = same as cavernous sinus syndrome + CN II (visual loss) but V2 spared
- Tolosa-Hunt = idiopathic granulomatous cavernous sinus inflammation; dramatic steroid response
- NPC, sinonasal malignancy, JNA can extend via skull base into cavernous sinus
- Direct surgical risk during transsphenoidal/endoscopic skull base procedures
Bills bar