Tetanus wound treatment
Reading File
Finding Sources
Searching PubMed
tetanus wound management prophylaxis
Searching the Web
tetanus wound treatment prophylaxis guidelines 2024 2025
Reading File
Reading File
Reading Web Page
https://www.cdc.gov/tetanus/hcp/clinical-guidance/index.html
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough response.
Tetanus Wound Treatment
Overview
Tetanus is caused by Clostridium tetani, a Gram-positive spore-forming anaerobe found in soil and human intestines. It enters through wounds and produces tetanospasmin, a toxin that blocks inhibitory neurotransmitter release at CNS synapses, causing uncontrolled muscle spasms. The median incubation period is 7 days (range 4-14 days).
Part 1: Wound Management & Prophylaxis
This is the most critical step after any at-risk injury.
Step 1 - Wound Assessment & Care
Classify the wound first:
Clean/Minor wounds - Low tetanus risk
- Small cuts, superficial abrasions with no contamination
Dirty/Major wounds - High tetanus risk
- Penetrating or puncture wounds
- Wounds contaminated with dirt, soil, feces, or saliva (animal/human bites)
- Burns, crush injuries, compound fractures, frostbite
- Necrotic or gangrenous tissue
- Devitalized tissue (provides the anaerobic environment C. tetani needs)
Wound care steps:
- Clean the wound thoroughly
- Remove all dirt and foreign material
- Debride necrotic/devitalized tissue - this is essential, as devitalized tissue creates the anaerobic conditions that allow C. tetani to replicate
- Antibiotics are NOT recommended for tetanus prophylaxis (topical or systemic) - per CDC guidance (updated June 2025); treat infection if present, but not prophylactically for tetanus
Step 2 - Tetanus Vaccination (Active Immunization)
Use Tdap, DTaP, or Td depending on age and history.
| Vaccination History | Clean/Minor Wound | Dirty/Major Wound |
|---|---|---|
| Unknown or < 3 doses | Give vaccine | Give vaccine |
| ≥ 3 doses, last dose < 5 years ago | Not needed | Not needed |
| ≥ 3 doses, last dose 5-10 years ago | Not needed | Give vaccine booster |
| ≥ 3 doses, last dose > 10 years ago | Give vaccine booster | Give vaccine booster |
Key rule: A person who has completed a primary series AND received a booster within the past 5 years (dirty wound) or 10 years (clean wound) does NOT need vaccine or TIG.
Dose: 0.5 mL tetanus toxoid intramuscularly (Bailey & Love's Surgery, p. 476)
Note: Tetanus disease itself does NOT confer immunity - patients recovering from tetanus must still be actively immunized.
Step 3 - Tetanus Immune Globulin (TIG) - Passive Immunization
TIG provides immediate, temporary protection by neutralizing circulating toxin (it cannot neutralize toxin already bound to nerve endings).
TIG is NEVER indicated for clean/minor wounds.
TIG indications for dirty/major wounds:
| Condition | Give TIG? |
|---|---|
| Unknown vaccination history | Yes |
| Never received tetanus vaccines | Yes |
| Incomplete primary series (< 3 doses) | Yes |
| HIV infection | Yes |
| Severe immunodeficiency | Yes |
| Fully vaccinated, up to date | No |
Dose: 250 international units IM (some sources recommend 250-500 U; up to 3,000-6,000 U for treatment of established tetanus)
- Give TIG and vaccine at separate anatomical sites when both are needed
- Part of the TIG dose may be infiltrated around the wound if the wound site can be identified
- TIG is commercially available - the CDC does not stockpile it
Part 2: Treatment of Established Tetanus
Once tetanus develops, four strategies must be pursued simultaneously (Rosen's Emergency Medicine, p. 2592):
1. Supportive Care - Muscle Spasm Control
- Minimize all sensory stimulation (noise, light, touch trigger spasms)
- Benzodiazepines are the mainstay - they are GABA agonists that indirectly antagonize tetanospasmin effects:
- Diazepam - most studied; can be given orally, rectally, or IV; rapid onset
- Lorazepam / Midazolam - equally effective alternatives
- Note: IV diazepam and lorazepam contain propylene glycol - at high doses this can cause lactic acidosis
- Magnesium sulfate infusion - effective as adjuvant or first-line for mild-to-moderate tetanus to control spasms and rigidity
- Dantrolene - direct muscle relaxant, adjunctive use
- If spasms cannot be controlled: neuromuscular blockade + mechanical ventilation
- Avoid succinylcholine (risk of severe hyperkalemia in neuromuscular disease after ~day 4)
- Prefer non-depolarizing agents: vecuronium, rocuronium (fewer cardiovascular effects)
2. Eliminate Unbound Toxin - TIG (Treatment Dose)
- TIG 3,000-6,000 units IM as a single dose for generalized tetanus
- Some evidence supports intrathecal TIG for faster neutralization of CNS-bound toxin
- Equine antitoxin (available in some countries) is an alternative if human TIG is unavailable
3. Prevent Further Toxin Production - Wound Debridement + Antibiotics
- Surgical wound debridement - remove all necrotic and devitalized tissue; eliminate the anaerobic environment
- Antibiotics:
- Metronidazole (preferred) - 500 mg IV/oral every 6-8 hours
- Penicillin G - alternative (note: some sources suggest it may potentiate tetanospasmin by antagonizing GABA, making metronidazole preferable)
- Duration: 7-10 days
4. Active Immunization
- Give tetanus toxoid vaccine during hospitalization (disease does not confer immunity)
- Complete the 3-dose primary series if not previously vaccinated:
- 2nd dose: 1-2 months after 1st
- 3rd dose: 6-12 months after 1st
Part 3: ICU Care
Patients with established tetanus require ICU admission for:
- Airway management (laryngospasm risk)
- Autonomic dysfunction management (hypertension, tachycardia, hypotension - use labetalol, magnesium, or morphine)
- Nutritional support (prolonged course)
- Prevention of complications (DVT, pressure ulcers, aspiration pneumonia)
Overall case fatality rate: ~18%; approaches 50% in patients over 70 years old. (Rosen's Emergency Medicine)
Quick Reference: Prophylaxis Decision Table
| Clean/Minor Wound | Dirty/Major Wound | |
|---|---|---|
| Vaccine | If > 10 yrs since last dose, or unknown | If > 5 yrs since last dose, or unknown |
| TIG | Never | If unvaccinated, incomplete series, HIV, or severe immunodeficiency |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed, p. 476; Rosen's Emergency Medicine, p. 2589-2592; CDC Clinical Guidance for Wound Management to Prevent Tetanus (updated June 2025)
Pictures of tetanus wound look
Finding Sources
Searching the Web
tetanus wound clinical appearance types puncture laceration contaminated
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a full visual guide to tetanus-related wounds and their clinical appearance.
Tetanus Wound - Visual Guide
What Makes a Wound "Tetanus-Prone"?
C. tetani spores thrive in devitalized, anaerobic tissue. The wound itself doesn't look unusual - the danger is invisible (contamination + lack of oxygen in tissue). However, certain wound characteristics flag high risk:
Tetanus-prone wounds:
- Puncture/penetrating injuries in a contaminated environment
- Animal or human bites
- Compound fractures
- Foreign bodies embedded in tissue
- Wounds with systemic sepsis
High-risk tetanus-prone wounds (greatest danger):
- Heavy soil/manure contamination
- Extensive devitalized tissue
- Burns, crush injuries, frostbite
- Surgery delayed >6 hours
(Bailey and Love's Surgery, Table 3.3)
Image 1 - Grossly Contaminated Facial Wound (pre-debridement)
This is the type of heavily contaminated wound that poses the highest tetanus risk - extensive devitalized tissue, gross contamination, delayed presentation:

Fig. 33.14(a) - Late-presenting facial injury with gross contamination, prior to debridement. This is a classic "high-risk tetanus-prone" wound: delayed, devitalized, heavily soiled. (Bailey & Love's Short Practice of Surgery, 28th Ed.)
Image 2 - After Surgical Debridement and Delayed Primary Closure
The same wound post-debridement - the standard surgical response. All necrotic tissue has been removed to eliminate the anaerobic environment where C. tetani replicates, followed by delayed primary closure:

Fig. 33.14(c) - After thorough debridement + delayed primary closure. Good outcome. (Bailey & Love's Surgery, 28th Ed.)
Image 3 - Risus Sardonicus ("Lockjaw" Smile)
This is the clinical sign of established tetanus - not the wound itself, but the result. The involuntary sustained contraction of facial muscles produces this characteristic grimacing expression:

Fig. 33.15 - Risus sardonicus ("lockjaw" grin) in a tetanus patient. This is the first clinical sign - painful spasm of the masseter and facial muscles. (Bailey & Love's Surgery, 28th Ed., courtesy Dr. Samira Ajmal)
Image 4 - Extensive Soft Tissue Injury Post-Debridement (Intraoperative)
A severely degloved/lacerated wound after surgical debridement - showing what the wound bed looks like when all devitalized tissue is removed, ready for reconstruction:

Fig. 33.14(b) - Intraoperative view after debridement of devitalized tissue. The surgical goal is to convert a contaminated anaerobic wound environment into clean vascularized tissue. (Bailey & Love's Surgery, 28th Ed.)
Key Visual Points
| Feature | Tetanus Risk |
|---|---|
| Small puncture wound, clean skin | Can STILL be high risk if object was contaminated |
| Deep wound with dirt/soil | High risk |
| Wound with black/grey necrotic edges | Very high risk - devitalized tissue |
| Animal bite | High risk (saliva contamination) |
| Burn with charred tissue | High risk |
| Compound fracture with exposed bone | High risk |
Important: A wound does not need to look dramatic to carry tetanus risk. A small nail puncture from a rusty, soil-exposed nail is often MORE dangerous than a clean surgical incision, because the deep, narrow track creates the anaerobic pocket where C. tetani thrives.
Neonatal jaundice
Reading File
Finding Sources
Searching PubMed
neonatal jaundice hyperbilirubinemia management
Searching the Web
neonatal jaundice phototherapy guidelines 2024 2025 AAP
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive information and the key clinical decision charts. Here is the full structured answer.
Neonatal Jaundice (Neonatal Hyperbilirubinemia)
Pathophysiology
Bilirubin is formed from the breakdown of heme-containing proteins, primarily hemoglobin. Unconjugated (indirect) bilirubin binds to albumin and is carried to the liver, where glucuronyl transferase conjugates it for biliary excretion. Three physiologic factors combine to cause neonatal jaundice:
- Increased bilirubin production - neonates have a higher red cell mass, shorter RBC lifespan (~70-90 days vs. 120 days in adults), and more rapid breakdown
- Decreased clearance/excretion - immature hepatic glucuronyl transferase activity
- Increased enterohepatic resorption - intestinal bacteria that convert bilirubin to urobilinogen are absent in neonates; beta-glucuronidase in the gut deconjugates bilirubin back for reabsorption
Nearly every newborn develops a serum bilirubin >1 mg/dL (adult upper limit) in the first week. Jaundice becomes clinically visible at ~5 mg/dL, progressing cephalocaudally (face first, feet last - Kramer's zones).
Classification
Unconjugated (Indirect) Hyperbilirubinemia - Most Common
| Category | Causes |
|---|---|
| Physiologic (benign) | Physiologic jaundice of the newborn, breast milk jaundice |
| Hemolysis | ABO incompatibility, Rh incompatibility (HDFN), G6PD deficiency, hereditary spherocytosis, sickle cell, thalassemia, birth-trauma hematoma (cephalohematoma), intracranial hemorrhage |
| Infectious | Sepsis, TORCHS infections, UTI |
| Obstructive (GI) | Hirschsprung disease, meconium ileus, pyloric stenosis, duodenal atresia |
| Metabolic/genetic | Galactosemia, congenital hypothyroidism, Crigler-Najjar syndrome, Gilbert syndrome |
Conjugated (Direct) Hyperbilirubinemia - Always Pathologic
| Category | Causes |
|---|---|
| Biliary | Biliary atresia (most important), choledochal cyst, inspissated bile, Alagille syndrome |
| Infectious | Gram-negative sepsis, TORCHS, hepatitis B, HIV, listeriosis |
| Metabolic | Galactosemia, tyrosinemia, alpha-1-antitrypsin deficiency, cystic fibrosis, glycogen storage disease IV |
| Other | Parenteral nutrition, Dubin-Johnson syndrome, Rotor syndrome |
(Rosen's Emergency Medicine; Quick Compendium of Clinical Pathology)
Key rule: Conjugated hyperbilirubinemia in a neonate is always pathologic and requires urgent investigation.
Physiologic vs. Pathologic Jaundice
| Feature | Physiologic | Pathologic |
|---|---|---|
| Onset | Day 2-3 of life | Within 24 hours of birth |
| Rise rate | < 5 mg/dL/day | > 5 mg/dL/day |
| Peak | Day 4-5 (term), up to day 7 (preterm) | Any time |
| Level | Rarely > 12-15 mg/dL | Can exceed 20+ mg/dL |
| Resolution | By 2 weeks (term), 3 weeks (preterm) | Persists > 3 weeks |
| Type | Unconjugated | Conjugated or high unconjugated |
Breast milk jaundice: A distinct, benign form - prolonged unconjugated jaundice beyond 2 weeks in a breastfed infant due to a factor in breast milk that increases intestinal bilirubin reabsorption. Breastfeeding should be encouraged, not stopped.
Risk Factors for Severe Hyperbilirubinemia
- Prematurity (gestational age 35-37 weeks)
- Isoimmune hemolytic disease (ABO or Rh incompatibility)
- G6PD deficiency
- Sepsis / asphyxia / acidosis
- Significant lethargy
- Temperature instability
- Albumin < 3.0 g/dL
- Cephalohematoma
- East Asian ethnicity
Complications - Kernicterus
At bilirubin levels > 20-25 mg/dL, unconjugated bilirubin crosses the blood-brain barrier causing bilirubin-induced neurologic dysfunction (BIND). Kernicterus is the chronic, irreversible form.
Areas most affected: Basal ganglia (globus pallidus, subthalamic nucleus), cerebellar vermis, dentate nuclei, hippocampus, cranial nerve nuclei (especially oculomotor and VIII)
Acute signs (Bilirubin Encephalopathy):
- Poor feeding, lethargy
- High-pitched cry
- Rigidity, opisthotonus (backward arching)
- Fever, seizures
Chronic sequelae (Kernicterus):
- Choreoathetoid cerebral palsy
- High-frequency sensorineural deafness
- Cognitive impairment / learning deficits
- ~50% mortality in untreated severe cases; 70% of affected infants die in first week
(Tietz Textbook of Laboratory Medicine; Bradley & Daroff's Neurology)
Diagnosis
When to Evaluate (Red Flags - Box 166.1)
- Jaundice within 24 hours of birth
- Any elevated direct (conjugated) bilirubin
- Rapidly rising TSB unexplained by history
- TSB approaching exchange transfusion threshold or not responding to phototherapy
- Jaundice persisting beyond 3 weeks
- Sick-appearing infant
Tests
- Transcutaneous bilirubin (TcB) - rapid bedside screen (valid after 24 hrs of life, within 7 days; not for infants who have had phototherapy)
- If TcB ≥ 15 mg/dL or within 3 mg/dL of phototherapy threshold → confirm with serum
- Total serum bilirubin (TSB) + direct fraction - fractionation identifies conjugated vs. unconjugated
- CBC + peripheral smear - for hemolysis (spherocytes, elliptocytes)
- Direct Coombs test (DAT) - for immune-mediated hemolysis
- Blood group typing of mother and infant
- In sick infants: blood glucose, electrolytes, urine reducing substances, ammonia, lactate, blood culture
Management
1. Encourage Feeding
Oral intake stimulates intestinal motility, reduces enterohepatic reabsorption, and lowers bilirubin. Breastfeeding should be continued, not stopped.
2. Phototherapy
Phototherapy is the first-line treatment for unconjugated hyperbilirubinemia. Light at ~450 nm disrupts intramolecular hydrogen bonds in bilirubin, converting it to water-soluble photoisomers that can be excreted without hepatic conjugation.
Initiate when TSB exceeds the age- and risk-adjusted phototherapy threshold (AAP guidelines):
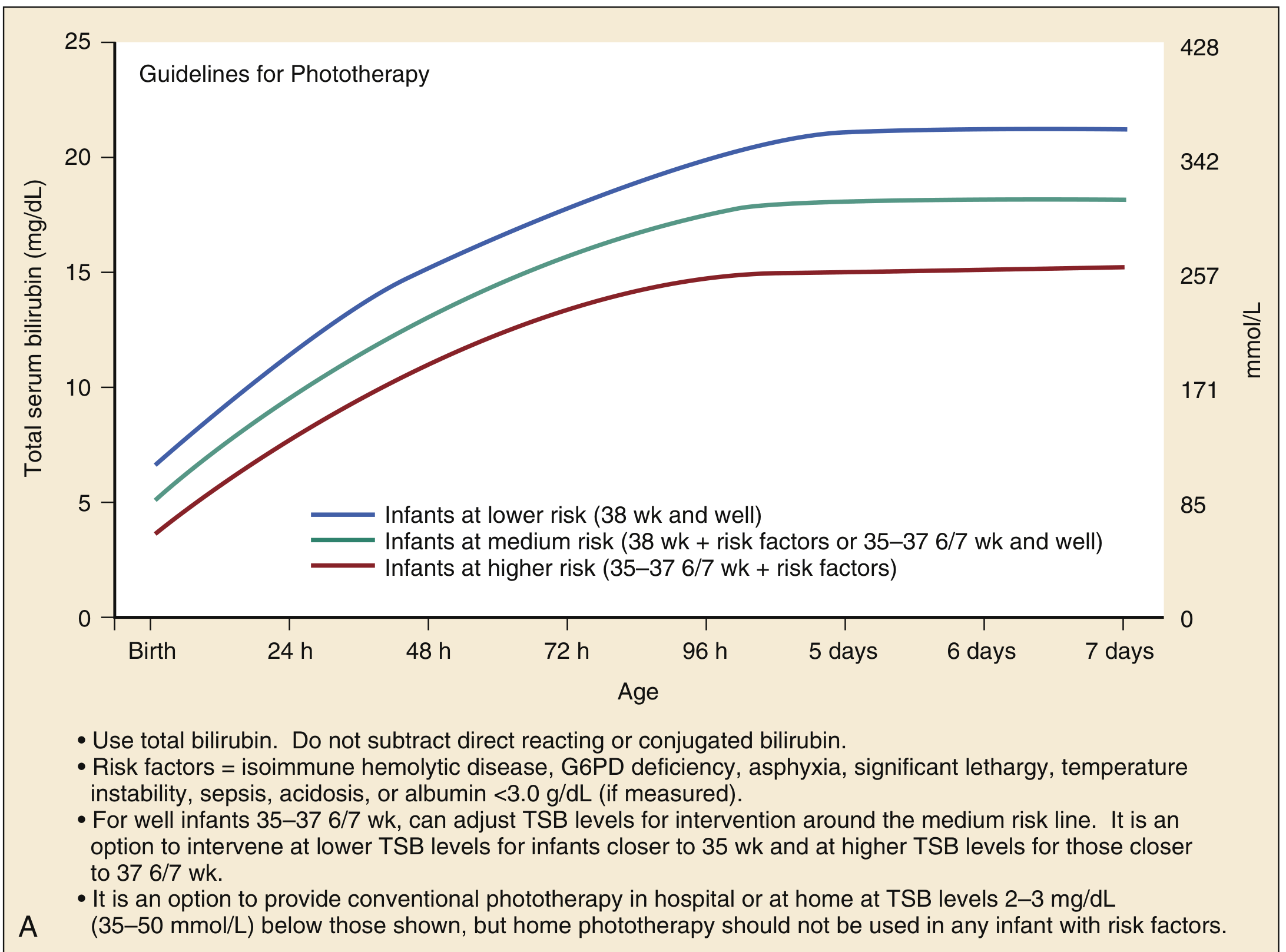
Fig. 166.1A - AAP Guidelines for Phototherapy (infants ≥35 weeks gestation). Use total bilirubin. Risk factors = isoimmune hemolytic disease, G6PD deficiency, asphyxia, lethargy, temperature instability, sepsis, acidosis, albumin <3.0 g/dL. (Rosen's Emergency Medicine)
- Lower risk (≥38 wk, well): phototherapy threshold ~15-21 mg/dL depending on age
- Medium risk (38 wk + risk factors, or 35-37 wk well): lower threshold
- Higher risk (35-37 wk + risk factors): lowest threshold
The 2022 AAP updated guidelines raised phototherapy thresholds slightly (risk-stratified), which reduced phototherapy use by ~50% without increasing readmissions.
3. Exchange Transfusion
Reserved for severe or refractory hyperbilirubinemia. Most effective and rapid method to remove bilirubin.
Indications:
- TSB above age-specific exchange transfusion threshold (see chart)
- Failure of phototherapy (TSB continues rising despite intensive phototherapy)
- Signs/symptoms of acute bilirubin encephalopathy (hypertonia, arching, opisthotonus, high-pitched cry, fever)
- TSB ≥ 5 mg/dL above exchange threshold lines
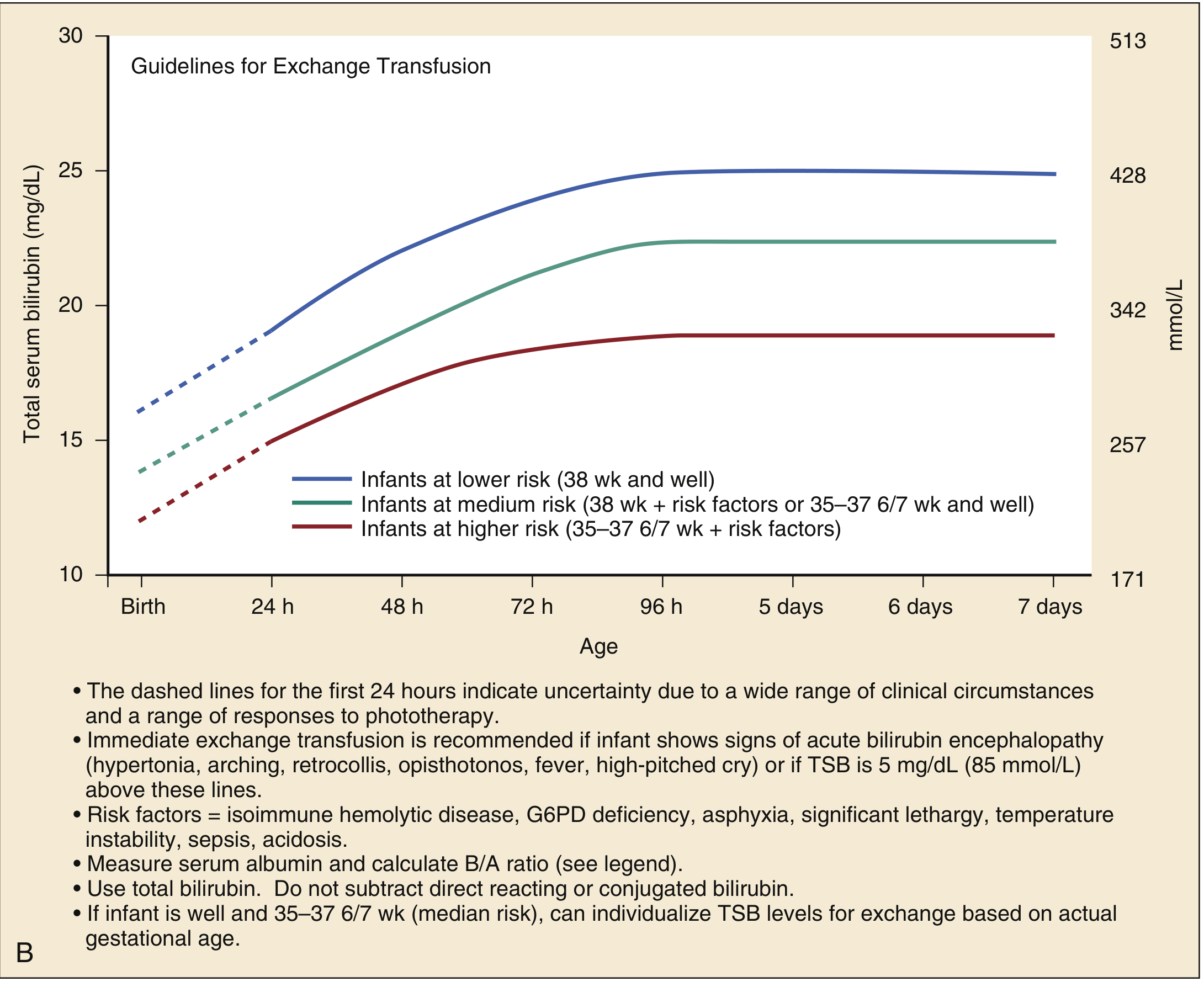
Fig. 166.1B - AAP Guidelines for Exchange Transfusion. Immediate exchange transfusion if signs of acute bilirubin encephalopathy OR TSB is 5 mg/dL above these lines. (Rosen's Emergency Medicine)
Procedure: Double-volume transfusion (180-190 mL/kg packed RBCs) serially removes 5-10 mL/kg aliquots and replaces with donor blood, replacing ~85% of infant's blood volume and reducing bilirubin by ≥50%. Must be done in NICU.
4. Treatment of Conjugated Hyperbilirubinemia
- Treat the underlying cause (antibiotics for sepsis, surgery consult for biliary atresia)
- Biliary atresia requires Kasai portoenterostomy before 8 weeks of age for best outcomes
- All infants with direct hyperbilirubinemia require hospital admission
Disposition Summary
| Situation | Action |
|---|---|
| TSB above phototherapy threshold, well infant | Phototherapy (inpatient or home if reliable caregiver + 24h follow-up) |
| Ill-appearing, poor feeding, dehydrated | Admit - phototherapy + IV hydration |
| TSB at/near exchange transfusion threshold | NICU admission, exchange transfusion |
| Any direct (conjugated) hyperbilirubinemia | Admit, investigate, subspecialty consult |
| Jaundice > 3 weeks | Evaluate for biliary atresia, hypothyroidism, metabolic cause |
Online tool: BiliTool (bilitool.org) uses AAP guidelines to calculate phototherapy/exchange thresholds based on exact age in hours and gestational age.
Sources: Rosen's Emergency Medicine (p. 3225-3228); Tietz Textbook of Laboratory Medicine, 7th Ed.; Bradley & Daroff's Neurology in Clinical Practice; Quick Compendium of Clinical Pathology 5th Ed.; AAP 2022 revised hyperbilirubinemia guidelines
Recent evidence: A 2026 Cochrane review (PMID 41784088) on high- vs. low-dose phototherapy and a 2024 Cochrane review (PMID 38804265) on transcutaneous bilirubinometry are the most recent systematic reviews in this area - no major changes to the above management framework are indicated.
Detailed treatment
Finding Sources
Finding Sources
Searching PubMed
neonatal hyperbilirubinemia phototherapy exchange transfusion treatment
Searching the Web
neonatal jaundice treatment phototherapy exchange transfusion AAP 2022 detailed management
Finding Sources
Finding Sources
Reading Web Page
https://emedicine.medscape.com/article/974786-treatment
Reading File
Finding Sources
Reading File
Reading File
Excellent - I now have comprehensive, authoritative content from the Harriet Lane Handbook (the premier neonatal reference), Rosen's EM, and Tintinalli's EM, plus current AAP 2022 guideline details. Let me compile the full detailed treatment answer.
Neonatal Jaundice - Detailed Treatment
STEP 1: General Supportive Measures
Adequate Feeding
Feeding is the single most important preventive and therapeutic intervention:
- Stimulates intestinal motility and bile flow, reducing enterohepatic recirculation of bilirubin
- Prevents dehydration (which concentrates bilirubin)
- Breastfeeding must be encouraged and continued - do not stop it
- If breastfeeding is inadequate, supplement with formula; supplementing with water or dextrose water is not effective and not recommended (AAP 2022: strong recommendation against)
- Target: 8-12 feeds per 24 hours in the first days of life
Avoid Exacerbating Factors
- Avoid drugs that displace bilirubin from albumin (e.g., sulphonamides, ceftriaxone in neonates)
- Treat any underlying sepsis, dehydration, or metabolic disturbance promptly
STEP 2: Phototherapy
Phototherapy is the primary treatment for unconjugated hyperbilirubinemia.
Mechanism
Light at approximately 450-460 nm (blue-green spectrum) converts unconjugated bilirubin in the skin via two photochemical reactions:
- Photo-isomerization - converts toxic Z,Z-bilirubin to water-soluble E,Z or Z,E isomers (reversible; major pathway, fast)
- Lumirubin formation - irreversible structural isomer, rapidly excreted in bile and urine without hepatic conjugation
- Photo-oxidation - minor pathway, slow
(Tietz Textbook of Laboratory Medicine)
Types of Phototherapy
| Type | Light Source | Notes |
|---|---|---|
| Conventional | Fluorescent blue-white lamps / LED | Standard inpatient setup |
| Intensive/high-dose | High-irradiance blue LED arrays | Used for severe/escalating cases |
| Fiberoptic ("Bili-blanket") | Fiberoptic pad on infant's back | Can be used at home; useful adjunct |
| Combined | Overhead + fiberoptic | Maximum surface area exposure |
Key Technical Points for Effective Phototherapy
- Maximize skin surface exposure - remove clothing except nappy; cover eyes with opaque shields (prevents retinal damage)
- Optimal irradiance: Standard phototherapy ≥ 8-10 μW/cm²/nm; intensive phototherapy ≥ 30 μW/cm²/nm in the 460-490 nm range
- Distance: Position light source as close as safely possible to infant (typically 20-30 cm for LED units - follow manufacturer guidance)
- Turning the infant is not necessary with overhead lights if back is exposed
- Goal: Intensive phototherapy should produce a TSB decline of 1-2 mg/dL within 4-6 hours
- Cover phototherapy lights when drawing bilirubin (light degrades bilirubin in samples)
Monitoring During Phototherapy (AAP 2022)
- Measure TSB within 12 hours of starting phototherapy
- Repeat TSB every 6-12 hours initially based on age, risk factors, and TSB trajectory
- Once TSB is falling and clearly below the exchange threshold, can extend to every 12-24 hours
- Do not subtract direct (conjugated) fraction from TSB when making treatment decisions
Discontinuing Phototherapy
- Stop when TSB falls 2-3 mg/dL below the phototherapy threshold
- Check rebound TSB 6-12 hours after stopping, then again the day after
- Risk of rebound is higher in: hemolytic disease, prematurity, early discharge
Home Phototherapy
- An option for well-appearing infants, reliable caregivers, access to emergency care
- Follow-up within 24 hours mandatory
- Never use for infants with neurotoxicity risk factors
STEP 3: Intravenous Immunoglobulin (IVIG)
Used specifically for immune-mediated hemolytic disease (ABO incompatibility, Rh disease) to reduce the need for exchange transfusion.
Mechanism
IVIG blocks Fc receptors on macrophages in the reticuloendothelial system, reducing antibody-mediated destruction of sensitized red blood cells, thereby slowing the rate of bilirubin production.
Indications (Harriet Lane Handbook)
- Isoimmune hemolytic disease (positive DAT)
- TSB rising despite intensive phototherapy, AND
- TSB within 2-3 mg/dL of exchange transfusion threshold
Dose
- 0.5-1 g/kg IV over 2 hours (Harriet Lane: 0.5-1 g/kg; Medscape: 500 mg/kg)
- May repeat dose in 12 hours if needed
- Start immediately - continue during transfer if transport is required
- Evidence: Reduces need for exchange transfusion in Rh and ABO isoimmunization; 2022 AAP includes it as a specific recommendation
STEP 4: Escalation of Care (NEW in AAP 2022)
This is a critical concept added to the 2022 AAP guideline:
Escalation-of-care threshold = TSB within 2 mg/dL of the exchange transfusion threshold
When TSB reaches this zone, it is a medical emergency.
Escalation Protocol
- Transfer to NICU urgently - must be capable of performing exchange transfusion
- Intensive phototherapy immediately - do not wait for lab results
- IV hydration - supports albumin levels and bilirubin excretion
- STAT labs: TSB + direct fraction, CBC, serum albumin, electrolytes, blood culture, type and crossmatch
- Measure TSB every 2 hours until out of escalation zone
- Consult neonatologist immediately
- Start IVIG if hemolytic disease is present
STEP 5: Exchange Transfusion
The most definitive and rapid method of bilirubin removal. Replaces antibody-coated RBCs (in hemolytic disease) and removes bilirubin directly.
Indications
- TSB at or above the exchange transfusion threshold (AAP Fig. 166.1B) despite intensive phototherapy
- TSB 5 mg/dL above exchange threshold lines
- Any signs of acute bilirubin encephalopathy regardless of TSB level: hypertonia, arching, retrocollis, opisthotonus, fever, high-pitched cry
- Failure of intensive phototherapy with rising TSB
Procedure Details (Harriet Lane Handbook)
| Parameter | Term Infant | Preterm Infant |
|---|---|---|
| Exchange volume | 160 mL/kg (double volume) | 200 mL/kg |
| Aliquot size | 15 mL per exchange | 2-3 mL/kg |
| Speed | Standard | 2-3 mL/kg/min (slower to avoid hemolysis) |
| Effect | Replaces ~85% of blood volume; reduces TSB by ≥50% |
Route:
- Blood removed via umbilical arterial catheter (UAC)
- Equal volume infused via umbilical venous catheter (UVC)
- If UAC unavailable: peripheral arterial line or single venous catheter
Blood product: Cross-matched, CMV-negative, irradiated packed red blood cells; reconstituted to a hematocrit of 40-50%
Pre-Procedure Checklist
- CBC, reticulocyte count, peripheral smear, bilirubin, Ca²⁺, glucose, total protein, blood type and Coombs test must be drawn on pre-exchange sample (these are diagnostically useless after exchange)
- Save sample for newborn screening, serologic or genetic studies
- Intensive phototherapy should be continued throughout the exchange transfusion procedure
Complications of Exchange Transfusion
| Complication | Details |
|---|---|
| Cardiovascular | Arrhythmia, air emboli, thromboembolism, hemodynamic instability |
| Metabolic | Hypocalcemia (citrate in blood product chelates Ca²⁺), hypoglycemia, hyperkalemia, acidosis |
| Hematologic | Coagulopathy, thrombocytopenia, graft-versus-host disease |
| Infectious | Sepsis, transmission of infection |
| Death | ~0.3-0.5% procedure mortality; higher in sick neonates |
Post-exchange: Continue phototherapy; monitor TSB every 2 hours; expect rebound (bilirubin redistributes from tissues back into blood); second exchange may rarely be needed.
STEP 6: Management of Conjugated Hyperbilirubinemia
Always pathologic. Treatment is cause-specific:
| Cause | Treatment |
|---|---|
| Biliary atresia | Kasai hepatoportoenterostomy - must be done before 8 weeks of age for best outcome; liver transplant if Kasai fails |
| Neonatal hepatitis / cholestasis | Ursodeoxycholic acid, fat-soluble vitamin supplementation (A, D, E, K) |
| Sepsis | IV antibiotics, supportive care |
| Galactosemia | Lactose-free formula immediately |
| Congenital hypothyroidism | Thyroid hormone replacement (L-thyroxine) |
| TPN-associated cholestasis | Reduce/cycle parenteral nutrition; introduce enteral feeds |
Summary Treatment Algorithm
Measure TSB (TcB screen → confirm with serum if ≥15 mg/dL or within 3 mg/dL of threshold)
│
▼
Is jaundice < 24 h, or conjugated? → ALWAYS PATHOLOGIC → Investigate + admit
│
▼
Plot TSB on AAP nomogram (age in hours + gestational age + risk factors)
│
┌─────┴──────────────────┐
▼ ▼
Below phototherapy At phototherapy At escalation zone At exchange level
threshold threshold (within 2 mg/dL of or above
│ │ exchange threshold) │
▼ ▼ │ ▼
Encourage feeding, Phototherapy MEDICAL EMERGENCY: Exchange transfusion
close follow-up (home or inpatient) NICU transfer + + intensive
IVIG if hemolytic + intensive phototherapy phototherapy throughout
TSB within 2-3 mg/dL + IV fluids + IVIG
of exchange level + STAT labs
Phototherapy Thresholds for Preterm Infants (Harriet Lane, Table 18.9)
| Gestational Age | Start Phototherapy | Consider Exchange Transfusion |
|---|---|---|
| < 28 weeks | 5-6 mg/dL | 11-14 mg/dL |
| 28-29 6/7 weeks | 6-8 mg/dL | 12-14 mg/dL |
| 30-31 6/7 weeks | 8-10 mg/dL | 13-16 mg/dL |
| 32-33 6/7 weeks | 10-12 mg/dL | 15-18 mg/dL |
| ≥ 35 weeks | Use AAP nomogram (hour-specific) | Use AAP nomogram |
Pharmacological Adjuncts (Limited Role)
| Agent | Mechanism | Evidence |
|---|---|---|
| Phenobarbitone | Induces hepatic glucuronyl transferase, increases bilirubin excretion | A 2025 systematic review (PMID 40604638) confirms it reduces TSB but its clinical use is limited by sedation and delayed onset; not standard first-line |
| Clofibrate | Enhances hepatic bilirubin conjugation | Limited evidence; not in routine use |
| Tin-mesoporphyrin | Inhibits heme oxygenase → reduces bilirubin production | Promising; not yet widely available |
| Oral zinc sulfate | Reduces enterohepatic circulation | Adjunct; early evidence only |
| IV albumin | Increases bilirubin binding capacity before exchange transfusion | May be given (1 g/kg) 1-2 hours before exchange to mobilize tissue bilirubin |
Sources: Harriet Lane Handbook 23rd Ed. (Johns Hopkins); Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; AAP 2022 Hyperbilirubinemia Guidelines; Medscape Neonatal Jaundice Treatment
This is a shared conversation. Sign in to Orris to start your own chat.