Excellent — I now have comprehensive source material. Here is the complete, structured answer to all 20 questions.
Questions 181–200: Jaundice, Hepatitis, Cirrhosis & Liver Cancer
181. Classification of Jaundice
Jaundice (icterus) is organized according to the phase of bilirubin metabolism at which dysfunction occurs:
I. Prehepatic (Hemolytic / Suprahepatic) Jaundice
- Excess bilirubin production overwhelms hepatic conjugation
- Predominantly unconjugated (indirect) hyperbilirubinemia
- Examples: hereditary spherocytosis, sickle cell disease, thalassemia, G6PD deficiency, autoimmune hemolytic anemia, malaria
II. Hepatic (Parenchymal) Jaundice
- Defect in hepatocyte uptake, conjugation, or excretion
- May present with mixed (both conjugated and unconjugated) hyperbilirubinemia
- Examples: viral hepatitis, alcoholic hepatitis, drug-induced liver injury, cirrhosis, autoimmune hepatitis, inherited disorders (Gilbert's, Crigler-Najjar, Dubin-Johnson, Rotor syndrome)
III. Posthepatic (Mechanical / Obstructive / Subhepatic) Jaundice
- Obstruction of bile flow after bilirubin is conjugated
- Predominantly conjugated (direct) hyperbilirubinemia
- Examples: choledocholithiasis, carcinoma of the pancreatic head, cholangiocarcinoma, biliary strictures, primary sclerosing cholangitis
— Harrison's Principles of Internal Medicine 22E; Schwartz's Principles of Surgery 11th Ed.
182. Main Causes of Jaundice Syndrome
Prehepatic causes
- Hemolytic anemias (inherited and acquired)
- Ineffective erythropoiesis (B₁₂, folate, iron deficiency)
- Resorption of large hematomas
- Massive blood transfusion
Hepatic causes
- Viral hepatitis (A, B, C, D, E)
- Alcoholic liver disease
- Drug/toxin-induced hepatocellular injury
- Autoimmune hepatitis
- Ischemic hepatitis
- Inherited disorders: Gilbert's syndrome (reduced UGT1A1 activity), Crigler-Najjar syndrome, Dubin-Johnson syndrome, Rotor syndrome
- Infiltrative diseases (lymphoma, sarcoidosis, amyloidosis)
Posthepatic causes
- Choledocholithiasis (common bile duct stones)
- Carcinoma of the pancreatic head
- Cholangiocarcinoma (Klatskin tumor)
- Ampullary carcinoma
- Biliary strictures (post-surgical, inflammatory)
- Primary sclerosing cholangitis
- Chronic pancreatitis causing biliary compression
- Parasitic biliary obstruction
Bilirubin metabolism dysfunction can arise from: (1) overproduction; (2) impaired uptake, conjugation, or excretion; (3) regurgitation from damaged hepatocytes or bile ducts. — Harrison's 22E
183. Diagnostic Criteria for Prehepatic (Hemolytic) Jaundice
| Feature | Finding |
|---|
| Skin color | Lemon-yellow (mild icterus) |
| Serum bilirubin | ↑ Total; predominantly indirect (unconjugated) |
| Urine bilirubin | Absent (unconjugated bilirubin is not water-soluble) |
| Urine urobilinogen | ↑↑ Increased |
| Stool color | Normal to dark (↑ stercobilin) |
| Liver enzymes (ALT, AST) | Normal |
| Alkaline phosphatase (ALP) | Normal |
| CBC | Anemia; reticulocytosis; fragmented RBCs on smear |
| LDH | Elevated |
| Haptoglobin | Low (consumed by free hemoglobin) |
| Direct Coombs | Positive in immune hemolysis |
| Spleen | Often enlarged (splenomegaly) |
| Liver | Normal size |
In hemolysis, serum bilirubin rarely exceeds 5 mg/dL unless there is coexistent renal/hepatocellular dysfunction or acute crisis. — Harrison's 22E, p. 366
184. Diagnostic Criteria for Hepatic (Parenchymal) Jaundice
| Feature | Finding |
|---|
| Skin color | Saffron-yellow to bright yellow |
| Serum bilirubin | ↑ Both conjugated and unconjugated (mixed) |
| Urine bilirubin | Present (conjugated bilirubin is water-soluble) |
| Urine urobilinogen | Variable (↑ in hepatitis, ↓ in severe hepatocellular failure) |
| Stool color | Pale/acholic in severe cases |
| ALT, AST | Markedly elevated (hepatocellular pattern: ALT/AST >> ALP) |
| ALP, GGT | Mildly–moderately elevated |
| Albumin | Decreased (in chronic disease) |
| Prothrombin time | Prolonged (impaired synthesis of clotting factors) |
| Liver | Tender hepatomegaly in acute hepatitis |
| Viral markers | Anti-HAV IgM, HBsAg, anti-HCV, etc. |
| Autoantibodies | ANA, SMA, LKM (if autoimmune hepatitis suspected) |
The hallmark pattern is disproportionate elevation of ALT/AST relative to ALP. — Harrison's 22E
185. Diagnostic Criteria for Subhepatic (Mechanical/Obstructive) Jaundice
| Feature | Finding |
|---|
| Skin color | Greenish-yellow (verdinous jaundice); may progress to bronze |
| Pruritus | Prominent (bile salts deposited in skin) |
| Serum bilirubin | ↑ Predominantly conjugated (direct) |
| Urine bilirubin | Present, dark (tea-colored) |
| Urine urobilinogen | Absent or very low |
| Stool color | Pale, acholic (clay-colored) (no bile in gut) |
| ALP | Markedly elevated (cholestatic pattern: ALP >> ALT/AST) |
| GGT | Markedly elevated |
| ALT, AST | Mildly elevated or normal |
| Bile acids | Elevated |
| Cholesterol | Elevated (fat malabsorption) |
| Fat-soluble vitamins | Deficient (A, D, E, K) — prolonged PT |
| Ultrasound / CT | Dilated intrahepatic and/or extrahepatic bile ducts |
| Clinical signs | Courvoisier sign (palpable, non-tender gallbladder) if pancreatic head mass |
Biliary obstruction causes elevated ALP from increased synthesis and release from bile duct epithelium; GGT elevation confirms hepatic origin. ALP has a half-life of ~7 days, so levels normalize slowly even after obstruction is relieved. — Schwartz's Surgery 11E, p. 1381
186. Clinical and Laboratory Signs of Jaundice
Clinical Signs
- Icterus — yellowish discoloration of sclera (first visible at bilirubin >2.5–3 mg/dL), skin, mucous membranes
- Pruritus — especially in cholestatic jaundice
- Dark urine (bilirubinuria) — conjugated jaundice
- Pale/acholic stools — obstructive jaundice
- Xanthomas / xanthelasmas — chronic cholestasis
- Hepatomegaly — hepatic or obstructive causes
- Splenomegaly — hemolytic or portal hypertension
- Steatorrhea — chronic bile duct obstruction (fat malabsorption)
- Spider nevi, palmar erythema, leukonychia, caput medusae — chronic liver disease
Laboratory Signs
- Total bilirubin (fractionated into direct/indirect)
- ALT, AST — hepatocellular injury markers
- ALP, GGT — cholestasis markers
- Albumin, prothrombin time — hepatic synthetic function
- CBC — anemia, reticulocytosis in hemolysis
- LDH, haptoglobin — hemolysis markers
- Urinalysis — bilirubinuria, urobilinogen
187. Differential Diagnostic Signs of Different Forms of Jaundice
| Feature | Hemolytic (Prehepatic) | Parenchymal (Hepatic) | Obstructive (Subhepatic) |
|---|
| Skin color | Lemon-yellow | Saffron/bright yellow | Greenish-yellow to bronze |
| Pruritus | Absent | Mild/absent | Marked |
| Urine color | Normal | Dark | Dark (tea) |
| Stool color | Dark | Pale/normal | Acholic (clay) |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | ↑↑ | ↑ or variable | Absent |
| Total bilirubin | ↑ (mainly indirect) | ↑ (mixed) | ↑ (mainly direct) |
| ALT/AST | Normal | ↑↑ Markedly elevated | Mildly elevated |
| ALP/GGT | Normal | Mildly elevated | ↑↑ Markedly elevated |
| Albumin | Normal | ↓ (chronic) | Normal (acute) |
| PT | Normal | Prolonged | Prolonged (corrects with Vit K) |
| Anemia | Hemolytic anemia | Absent | Absent |
| Reticulocytes | ↑↑ | Normal | Normal |
| Haptoglobin | ↓ | Normal | Normal |
| Bile duct dilation | No | No | Yes (on imaging) |
Key distinguishing rule:
- Prehepatic → indirect bilirubin dominant, no bilirubinuria, ↑ urobilinogen
- Hepatic → mixed bilirubin, markedly elevated transaminases
- Posthepatic → direct bilirubin dominant, absent urobilinogen, ↑ ALP/GGT, dilated bile ducts
188. Role of ALT, AST, ALP, and GGT in Differential Diagnosis of Jaundice
ALT (Alanine Aminotransferase)
- Liver-specific enzyme; found in hepatocyte cytoplasm
- Markedly elevated in hepatocellular damage (viral hepatitis, drug injury, ischemic hepatitis)
- ALT > AST suggests viral hepatitis
- AST:ALT ratio >2:1 suggests alcoholic liver disease
AST (Aspartate Aminotransferase)
- Found in liver, heart, muscle, kidney — less specific
- Elevated with ALT in hepatocellular injury
- Isolated AST elevation may indicate myocardial or skeletal muscle damage
ALP (Alkaline Phosphatase)
- Expressed by bile duct epithelium in the liver; also found in bone, intestine, placenta
- Elevated in biliary obstruction (intra- or extrahepatic) — synthesized in excess and released into serum
- Half-life ≈ 7 days; slow normalization after obstruction resolves
- To confirm hepatic origin, check GGT or liver isoenzyme (both elevated = liver source)
- Isolated ALP elevation without GGT suggests bone disease
GGT (Gamma-Glutamyl Transferase)
- Located in hepatocytes and bile duct epithelium
- Most sensitive marker of hepatobiliary disease (but non-specific)
- Induced by: alcohol, certain drugs (phenytoin, barbiturates), pancreatic disease, MI, renal failure
- Elevated GGT + elevated ALP = confirms hepatic source of ALP
- GGT elevated alone (normal ALP) → suspect alcohol use or drug induction
Diagnostic pattern summary:
- Hepatocellular injury: ALT/AST >> ALP
- Cholestatic injury: ALP/GGT >> ALT/AST
— Schwartz's Surgery 11E, p. 1380
189. Main Biochemical Markers of Cholestasis and Cytolysis
Markers of Cytolysis (Hepatocellular Injury)
| Marker | Significance |
|---|
| ALT | Most specific for hepatocyte necrosis; >10× ULN = severe cytolysis |
| AST | Less specific; parallels ALT in viral hepatitis |
| LDH | Nonspecific; ↑ in ischemic hepatitis ("shock liver") |
| Serum iron | Elevated in hepatocyte necrosis (release from damaged cells) |
Markers of Cholestasis (Impaired Bile Flow)
| Marker | Significance |
|---|
| ALP | Elevated in biliary obstruction (intra- or extrahepatic) |
| GGT | Sensitive early marker; confirms hepatic origin of ALP ↑ |
| Conjugated (direct) bilirubin | Elevated; spills into urine |
| Total bile acids | Elevated (accumulate when bile flow impaired) |
| Cholesterol | Elevated (impaired biliary excretion) |
| 5'-nucleotidase | Liver-specific; rises in cholestasis; useful when ALP elevated in pregnancy/bone disease |
Markers of Hepatic Synthetic Function
| Marker | Significance |
|---|
| Albumin | Decreased in chronic liver failure (half-life ~20 days) |
| Prothrombin time (PT/INR) | Prolonged — reflects failure to synthesize clotting factors I, II, V, VII, X |
| Fibrinogen | Decreased in severe hepatic failure |
190. Instrumental Methods for Diagnosing Jaundice
1. Abdominal Ultrasound (First-line)
- Non-invasive, radiation-free
- Detects: dilated bile ducts (obstructive jaundice), gallstones, hepatomegaly, liver texture changes, masses
- Limitation: poor visualization of distal common bile duct (bowel gas)
2. CT Scan (Computed Tomography)
- Better visualization of biliary tree, pancreas, portal vein
- Identifies: pancreatic head masses, cholangiocarcinoma, hepatic metastases, lymphadenopathy
- With contrast: defines vascular anatomy
3. MRCP (Magnetic Resonance Cholangiopancreatography)
- Non-invasive "roadmap" of the biliary tree
- Gold standard for diagnosing bile duct strictures, choledocholithiasis, primary sclerosing cholangitis
- No radiation, no contrast required
4. ERCP (Endoscopic Retrograde Cholangiopancreatography)
- Diagnostic and therapeutic — allows sphincterotomy, stone extraction, stent placement
- Used when MRCP confirms obstruction requiring intervention
- Risk of pancreatitis, cholangitis, perforation
5. PTC (Percutaneous Transhepatic Cholangiography)
- Alternative when ERCP not feasible
- Can place external/internal biliary drains
6. Liver Biopsy
- Definitive for hepatocellular jaundice when etiology unclear after serologic testing
- Transjugular approach preferred in coagulopathy
- Guides diagnosis of autoimmune hepatitis, PBC, PSC, storage diseases, malignancy
7. Endoscopic Ultrasound (EUS)
- High-resolution imaging of distal bile duct and pancreatic head
- Allows fine-needle aspiration of masses
191. Classification of Chronic Hepatitis
Chronic hepatitis is defined as hepatic inflammation lasting >6 months.
By Etiology
- Chronic viral hepatitis — HBV (±HDV), HCV
- Autoimmune hepatitis — Types 1, 2, 3
- Drug-induced chronic hepatitis — isoniazid, methyldopa, nitrofurantoin
- Metabolic/genetic — Wilson's disease, alpha-1 antitrypsin deficiency, NAFLD/NASH
- Cryptogenic — no identifiable cause
By Histological Grade & Stage (Knodell/METAVIR scoring)
- Grade (activity): degree of necroinflammation (0–4 or A0–A3)
- Stage (fibrosis): F0 (none) → F1 (portal fibrosis) → F2 (periportal) → F3 (bridging) → F4 (cirrhosis)
Traditional Histological Classification (older terminology, still used clinically)
- Chronic Persistent Hepatitis (CPH) — mild, portal inflammation, preserved lobular architecture, no necrosis; generally benign prognosis
- Chronic Active (Aggressive) Hepatitis (CAH) — periportal inflammation, piecemeal necrosis (interface hepatitis), progressive fibrosis; risk of cirrhosis
- Chronic Lobular Hepatitis — predominantly lobular necroinflammation
192. Diagnostic Criteria for Chronic Persistent Hepatitis (CPH)
CPH is a mild, non-progressive form of chronic hepatitis:
Clinical Features
- Often asymptomatic or mild fatigue, right upper quadrant discomfort
- No signs of hepatic decompensation (no jaundice, ascites, encephalopathy)
- Mild or no hepatomegaly
Laboratory Features
- Mild elevation of transaminases (ALT 1.5–3× ULN)
- Normal or near-normal albumin and PT
- Normal or mildly elevated bilirubin
- Specific serological markers depending on etiology (anti-HCV, HBsAg, ANA, etc.)
Histological Criteria (definitive)
- Portal inflammation confined to portal tracts
- Intact limiting plate (no interface hepatitis / piecemeal necrosis)
- Normal lobular architecture preserved
- Minimal or no fibrosis (F0–F1)
- Absence of bridging necrosis
Prognosis
- Generally benign; does not commonly progress to cirrhosis
- Regression possible with treatment of underlying cause (antiviral therapy, cessation of offending drug)
193. Principles of Treatment of Chronic Hepatitis
General Measures
- Remove/treat underlying cause (antiviral therapy, alcohol cessation, stop offending drugs)
- Avoid hepatotoxins (alcohol, certain medications)
- Vaccination against HAV and HBV if not immune
- Nutritional support
Viral Hepatitis B
- Tenofovir (TDF or TAF) or Entecavir — first-line oral antivirals
- Pegylated interferon-alfa — finite course, achieves HBsAg seroconversion in some patients
- Goal: suppress HBV DNA, normalize ALT, prevent fibrosis progression
Viral Hepatitis C
- Direct-acting antivirals (DAAs) — pangenotypic regimens: sofosbuvir/velpatasvir or glecaprevir/pibrentasvir
- Sustained virologic response (SVR = "cure") in >95% of patients
- 8–12 week courses
Autoimmune Hepatitis
- Prednisolone ± Azathioprine — standard induction and maintenance
- Budesonide as alternative in non-cirrhotic patients
- Mycophenolate mofetil for azathioprine-intolerant patients
NAFLD/NASH
- Weight loss (>7–10% body weight), exercise, metabolic optimization
- Control of diabetes, hyperlipidemia, hypertension
- Emerging pharmacotherapy: resmetirom, semaglutide (under evaluation)
Monitoring
- Regular LFTs, viral loads, AFP surveillance in HBV/HCV
- Fibrosis reassessment (elastography, APRI, FIB-4)
- Screen for hepatocellular carcinoma in advanced fibrosis/cirrhosis
194. Differential Diagnosis of Cirrhosis and Liver Cancer
| Feature | Cirrhosis | Primary Liver Cancer (HCC) |
|---|
| Onset | Insidious, years | May arise on cirrhotic background |
| Symptoms | Fatigue, jaundice, ascites, edema | Weight loss, RUQ pain, rapid deterioration |
| AFP | Mildly elevated or normal | Markedly elevated (>400 ng/mL highly suggestive) |
| Imaging (US/CT/MRI) | Nodular liver, splenomegaly, varices | Focal mass; arterial enhancement + venous washout (LI-RADS 5) |
| Biopsy | Cirrhotic nodules, fibrosis | Malignant hepatocytes, vascular invasion |
| CA 19-9 | Normal | Elevated in cholangiocarcinoma |
| Portal hypertension signs | Present (varices, caput medusae) | May be absent early |
| Prognosis | Variable; Child-Pugh/MELD scoring | Poor if advanced; Barcelona staging (BCLC) |
| Hepatic veins/IVC | Budd-Chiari if thrombosed | Tumor thrombus in portal/hepatic veins |
Secondary liver cancer (metastases): multiple lesions, known primary (colon, lung, breast), CEA/CA 19-9 elevated, ring-enhancing on CT.
195. Complications of Liver Cirrhosis
- Portal Hypertension → variceal bleeding (esophageal, gastric), portal hypertensive gastropathy
- Ascites — most common decompensation event; cirrhosis accounts for ~84% of cases
- Spontaneous Bacterial Peritonitis (SBP) — infection of ascitic fluid (PMN >250/mm³)
- Hepatic Encephalopathy — neuropsychiatric dysfunction from ammonia and other toxins; 20–40% 1-year survival after onset
- Hepatorenal Syndrome (HRS) — functional renal failure; HRS-1 (acute, severe) and HRS-2 (chronic)
- Hepatocellular Carcinoma (HCC) — annual incidence 1–8% in cirrhotic patients
- Coagulopathy — decreased synthesis of clotting factors, thrombocytopenia (hypersplenism)
- Hepatopulmonary Syndrome — intrapulmonary vascular dilatations → hypoxemia
- Portopulmonary Hypertension — elevated pulmonary artery pressure
- Malnutrition and Sarcopenia
- Hyponatremia — dilutional, due to ADH dysregulation
196. Basic Laboratory Parameters in Liver Cirrhosis
| Parameter | Finding | Significance |
|---|
| ALT / AST | Mildly–moderately elevated | Ongoing hepatocyte injury |
| ALP / GGT | Elevated | Cholestasis, biliary involvement |
| Bilirubin | Elevated (direct + indirect) | Impaired excretion and conjugation |
| Albumin | ↓ Decreased | Impaired synthetic function |
| PT / INR | Prolonged | Reduced clotting factor synthesis |
| Platelet count | ↓ Thrombocytopenia | Hypersplenism, reduced TPO synthesis |
| WBC | Leukopenia | Hypersplenism |
| Hemoglobin | Anemia (multifactorial) | Bleeding, hemolysis, nutrition |
| Serum Na⁺ | Hyponatremia | ADH excess, water retention |
| Creatinine / BUN | ↑ in HRS | Functional renal failure |
| Ammonia | Elevated | Hepatic encephalopathy risk |
| AFP | Mildly elevated | Regeneration; if very high → HCC |
| MELD score | 6–40+ | Calculated from bilirubin, INR, creatinine — predicts 3-month mortality |
| Child-Pugh score | A/B/C | Based on bilirubin, albumin, PT, ascites, encephalopathy |
197. Instrumental Diagnostics of Liver Cirrhosis
1. Abdominal Ultrasound
- First-line: nodular liver surface, increased echogenicity, caudate lobe hypertrophy
- Portal vein diameter >13 mm (portal hypertension)
- Splenomegaly, ascites, collateral vessels
2. Doppler Ultrasound
- Assesses portal blood flow direction (hepatofugal flow = severe portal hypertension)
- Detects portal vein thrombosis
3. CT / MRI
- Detailed liver morphology, HCC surveillance, vascular anatomy
- Dynamic contrast MRI — arterial enhancement of HCC nodules
4. Transient Elastography (FibroScan)
- Non-invasive fibrosis staging by measuring liver stiffness (kPa)
- Cirrhosis: >12.5 kPa (varies by etiology)
- Alternative non-invasive indices: APRI, FIB-4
5. Upper GI Endoscopy (Esophagogastroduodenoscopy)
- Identifies esophageal and gastric varices
- Grades variceal size; guides prophylactic banding or beta-blocker therapy
6. Liver Biopsy (Gold Standard for Histology)
- Confirms diagnosis, grades activity, stages fibrosis
- Transjugular approach preferred in coagulopathy (also measures hepatic venous pressure gradient — HVPG)
7. HVPG (Hepatic Venous Pressure Gradient)
-
5 mmHg = portal hypertension; >10 mmHg = clinically significant; >12 mmHg = variceal bleeding risk
198. Modern Principles of Liver Cirrhosis Therapy and Prognosis Criteria
Treatment Principles
Treat underlying cause:
- HBV/HCV: antiviral therapy (can lead to fibrosis regression)
- Alcohol: complete abstinence
- NASH: weight loss, metabolic management
- Autoimmune hepatitis: immunosuppression
- Wilson's disease: copper chelation (D-penicillamine, trientine)
Manage complications:
- Ascites: salt restriction (<2 g/day), diuretics (spironolactone ± furosemide), therapeutic paracentesis, TIPS
- Variceal prophylaxis: non-selective beta-blockers (propranolol, carvedilol) or endoscopic band ligation
- SBP: IV ceftriaxone/cefotaxime; prophylaxis with norfloxacin in high-risk patients
- Hepatic encephalopathy: lactulose (target 2–3 soft stools/day), rifaximin, identify and treat precipitants
- HRS: vasoconstrictors (terlipressin + albumin); renal replacement therapy
Liver transplantation:
- Indicated in decompensated cirrhosis (MELD ≥15), HCC within Milan criteria
- Milan criteria for HCC: single lesion ≤5 cm OR up to 3 lesions each ≤3 cm, no vascular invasion
Prognosis Criteria
Child-Pugh Score (A/B/C):
- Parameters: serum bilirubin, albumin, PT, degree of ascites, grade of encephalopathy
- Class A: 5–6 pts (1-year survival ~100%); Class B: 7–9 pts; Class C: 10–15 pts (1-year survival ~45%)
MELD Score (Model for End-Stage Liver Disease):
- Formula: 3.78×ln[bilirubin mg/dL] + 11.2×ln[INR] + 9.57×ln[creatinine mg/dL] + 6.43
- Range 6–40; higher = greater 3-month mortality
- Used for transplant waiting list prioritization
199. Modern Methods of Laboratory and Instrumental Diagnostics of Liver Cancer
Laboratory Methods
| Test | Significance |
|---|
| AFP (Alpha-fetoprotein) | Primary HCC marker; >400 ng/mL highly suggestive; >20 ng/mL with risk factors warrants imaging |
| AFP-L3 fraction | Lens culinaris agglutinin-reactive AFP; more specific for HCC |
| DCP / PIVKA-II (Des-gamma-carboxyprothrombin) | Complements AFP; elevated in HCC |
| CA 19-9 | Elevated in cholangiocarcinoma and metastatic pancreatic cancer |
| CEA | Elevated in colorectal liver metastases |
| LDH, ALP, bilirubin | Elevated with large tumor burden |
| Liver function panel | Baseline hepatic reserve assessment |
Instrumental Methods
| Method | Role |
|---|
| Ultrasound | Surveillance every 6 months in cirrhotic patients (±AFP) |
| CT (triphasic/dynamic) | Arterial enhancement + portal venous washout = HCC hallmark (LI-RADS classification) |
| MRI with hepatobiliary contrast (Eovist/Primovist) | Highly sensitive for small HCC; characterization of biliary tumors |
| PET-CT | Detects extrahepatic metastases and cholangiocarcinoma; limited sensitivity for well-differentiated HCC |
| ERCP / MRCP | Cholangiocarcinoma — biliary stricture characterization, brush cytology |
| EUS + FNA | Hilar cholangiocarcinoma, periportal lymph nodes |
| Liver biopsy | Histological confirmation if imaging non-diagnostic; not required if classic imaging + elevated AFP in cirrhosis |
| Angiography (DSA) | Pre-TACE/ablation planning; assesses tumor vascularity |
BCLC Staging System (Barcelona Clinic Liver Cancer) guides treatment allocation: Very early (0) → Early (A) → Intermediate (B) → Advanced (C) → Terminal (D).
200. Principles of Treatment for Primary and Secondary Liver Cancer
Primary Liver Cancer (Hepatocellular Carcinoma — HCC)
Curative options (early stage):
- Surgical resection — single tumor, adequate hepatic reserve (Child-Pugh A), no portal hypertension
- Liver transplantation — within Milan criteria; removes tumor and underlying cirrhosis
- Radiofrequency ablation (RFA) / Microwave ablation (MWA) — tumors ≤3 cm, not surgically resectable; curative intent
Locoregional therapy (intermediate stage):
- TACE (Trans-Arterial Chemo-Embolization) — standard for BCLC-B (multinodular, preserved liver function, no vascular invasion)
- TARE (Trans-Arterial Radio-Embolization with Y-90 microspheres) — alternative to TACE
Systemic therapy (advanced stage):
- Sorafenib (multikinase inhibitor) — first approved systemic therapy
- Lenvatinib — non-inferior to sorafenib, first-line alternative
- Atezolizumab + Bevacizumab — current preferred first-line regimen (immunotherapy + VEGF inhibition; superior OS vs sorafenib)
- Tremelimumab + Durvalumab — alternative first-line option
- Second-line: regorafenib, cabozantinib, ramucirumab (AFP >400)
Secondary Liver Cancer (Metastases)
Colorectal liver metastases (most common resectable type):
- Surgical resection — gold standard when technically feasible, adequate liver remnant
- Perioperative chemotherapy — FOLFOX/FOLFIRI ± bevacizumab/cetuximab
- Ablative techniques (RFA, MWA) — for small, unresectable lesions
- TACE / TARE — for chemorefractory, unresectable disease
Non-colorectal liver metastases:
- Primary systemic chemotherapy based on tumor origin
- Surgery rarely curative except neuroendocrine tumors (NET) metastases — resection and PRRT (peptide receptor radionuclide therapy)
- Liver-directed therapy as palliative adjunct
Cholangiocarcinoma:
- Resection when possible (R0 margin critical)
- Gemcitabine + cisplatin — standard first-line systemic chemotherapy
- Pemigatinib / Infigratinib — for FGFR2 fusion-positive intrahepatic cholangiocarcinoma (targeted therapy)
- Pembrolizumab — for MSI-H/dMMR tumors
- ERCP/PTC biliary drainage for obstructive jaundice
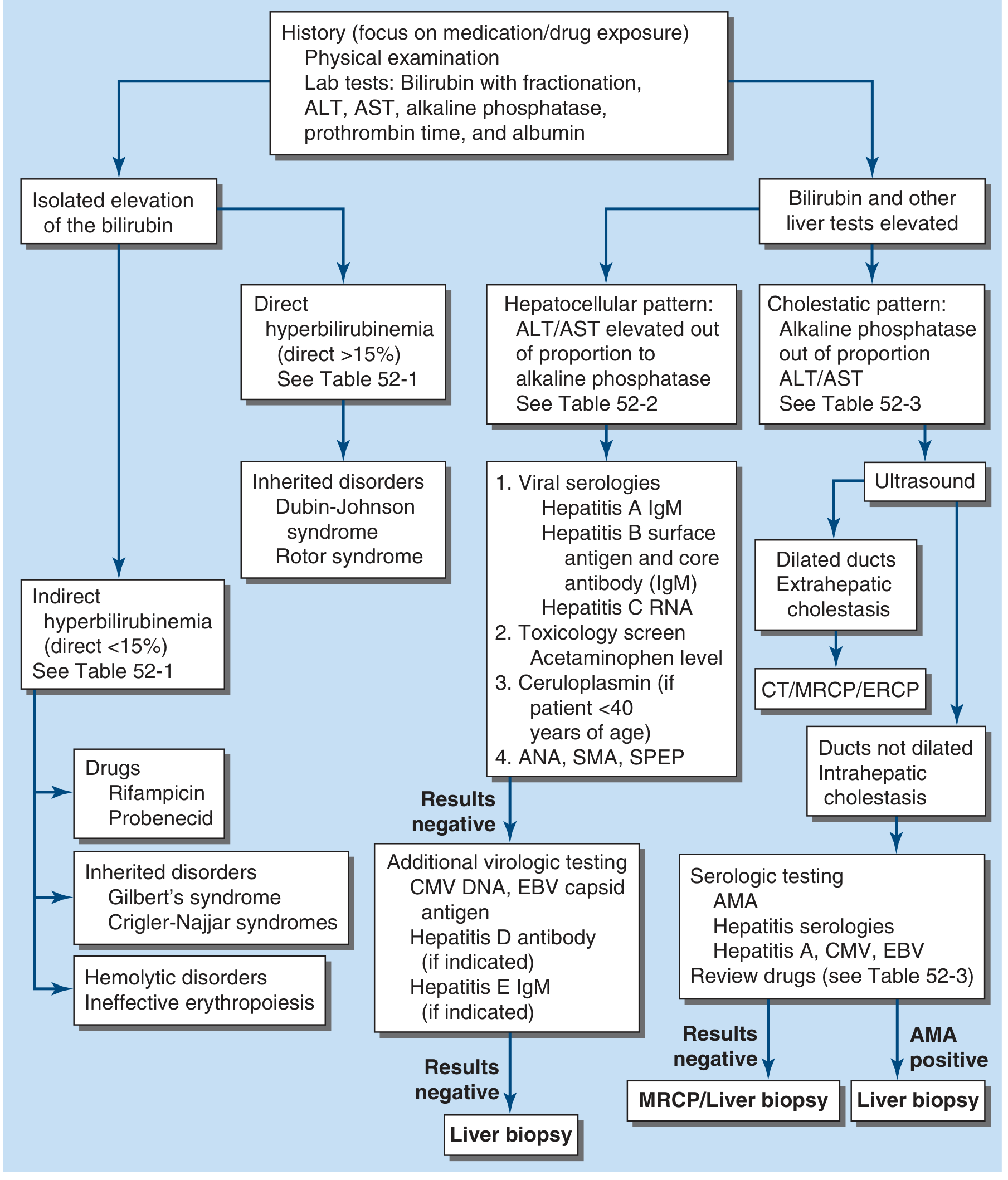
Diagnostic algorithm for jaundice (Harrison's 22E, Fig. 52-1):
Sources: Harrison's Principles of Internal Medicine 22E (2025); Schwartz's Principles of Surgery 11E; Sleisenger and Fordtran's GI and Liver Disease; Goldman-Cecil Medicine