Essay on macrovascular complications of diabetes mellitus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive essay on the macrovascular complications of diabetes mellitus, synthesized from multiple authoritative sources.
Macrovascular Complications of Diabetes Mellitus
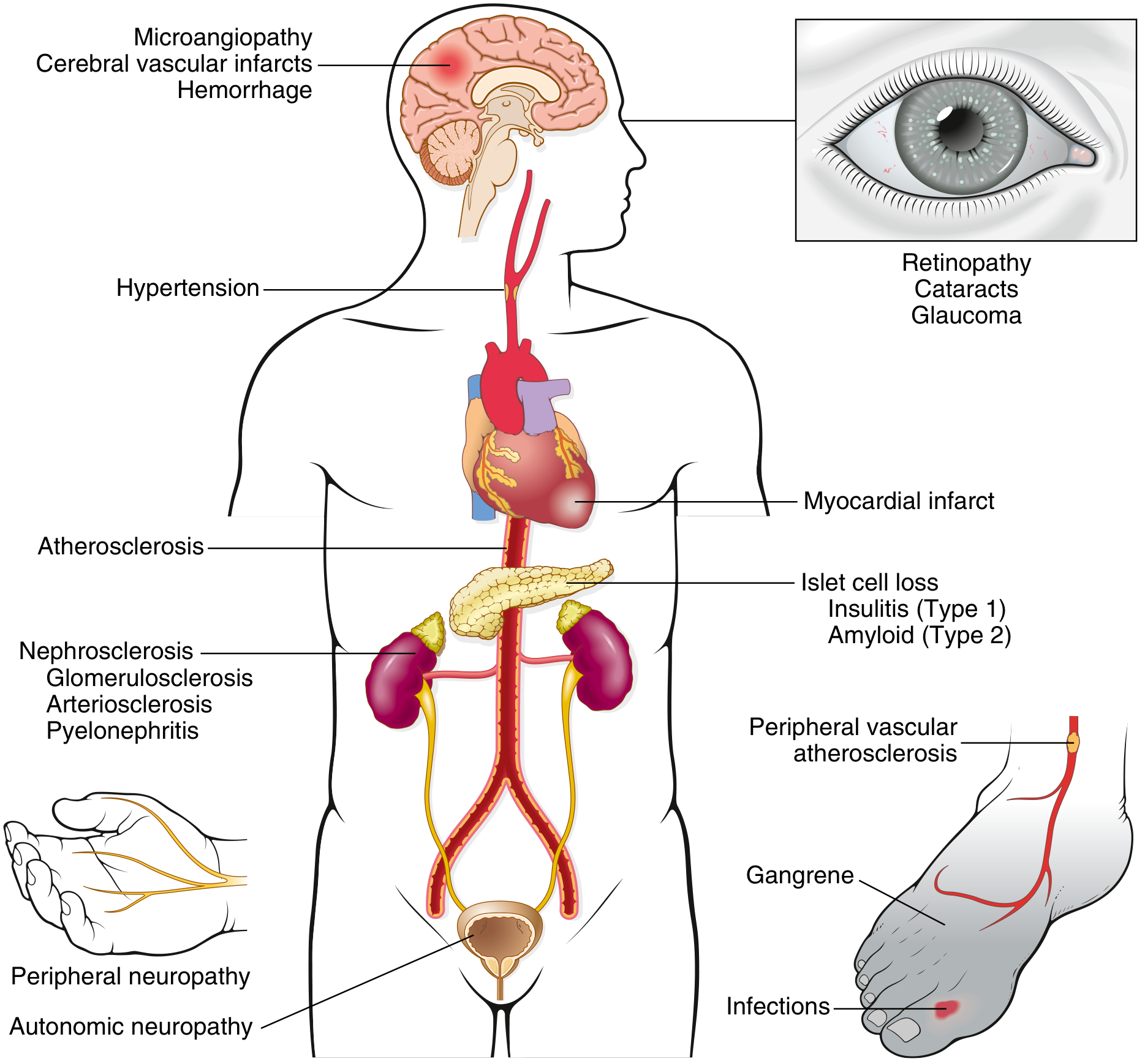
FIG. 18.22 Long-term complications of diabetes mellitus — Robbins & Kumar Basic Pathology
1. Overview and Classification
The chronic complications of diabetes mellitus arise from damage to both large vessels (macrovascular disease) and small vessels (microvascular disease). Macrovascular complications — encompassing atherosclerotic cardiovascular disease (ASCVD), peripheral arterial disease (PAD), cerebrovascular disease, and heart failure — are the dominant cause of morbidity and mortality in people with diabetes. Coronary heart disease (CHD), stroke, and peripheral vascular disease together account for approximately 80% of deaths in persons with diabetes.
An important distinction exists between the two complication classes: microvascular complications (retinopathy, nephropathy, neuropathy) are largely specific to diabetes and driven primarily by hyperglycemia, whereas macrovascular complications share pathophysiologic mechanisms with the general population, with hyperglycemia as one of several contributing factors alongside dyslipidemia, hypertension, and insulin resistance. — Harrison's Principles of Internal Medicine, 22E
2. Pathogenesis
2.1 Accelerated Atherosclerosis
The hallmark of diabetic macrovascular disease is accelerated atherosclerosis affecting the aorta and large- and medium-sized arteries. Except for its greater severity and earlier onset, atherosclerosis in patients with and without diabetes is morphologically indistinguishable. — Robbins & Kumar Basic Pathology
Several interacting mechanisms drive this acceleration:
Advanced Glycation End Products (AGEs)
Persistent hyperglycemia promotes the non-enzymatic glycation of proteins and lipids, forming AGEs. These bind to RAGE (receptor for AGE) on macrophages, T cells, endothelium, and vascular smooth muscle. The consequences include:
- Release of pro-inflammatory cytokines, TGF-β (promoting basement membrane deposition), and VEGF
- Generation of reactive oxygen species (ROS) in endothelial cells
- Increased procoagulant activity
- Enhanced vascular smooth muscle proliferation and extracellular matrix synthesis
- Direct cross-linking of LDL within large-vessel walls, accelerating plaque formation
Protein Kinase C (PKC) Activation
Intracellular hyperglycemia stimulates de novo synthesis of diacylglycerol (DAG) from glycolytic intermediates, activating PKC. This promotes VEGF-driven neovascularization and TGF-β–driven fibrosis, and broadly impairs endothelial function. — Robbins & Kumar Basic Pathology
Dyslipidemia and Oxidative Stress
Increases in oxidation and glyoxidation of lipoproteins enhance their atherogenicity and promote foam cell formation. Insulin resistance and dyslipidemia — elevated triglycerides, low HDL, and small dense LDL particles — are co-conspirators in plaque formation. — Goldman-Cecil Medicine
Endothelial Dysfunction and Prothrombotic State
Hyperglycemia, free fatty acids, and insulin resistance collectively cause endothelial dysfunction. This manifests as impaired nitric oxide bioavailability, increased adhesion molecule expression, platelet aggregation, and a shift toward a prothrombotic milieu.
Hyaline Arteriolosclerosis
The vascular lesion associated with hypertension is both more prevalent and more severe in diabetic patients and is characterized by amorphous hyaline thickening of arteriolar walls, narrowing the lumen. Its severity correlates with disease duration and the presence of hypertension. — Robbins & Kumar Basic Pathology
3. Coronary Heart Disease (CHD)
Epidemiology and Risk
Myocardial infarction (MI) is the most common cause of death in patients with diabetes. Notably, it is almost as common in diabetic women as in diabetic men — a stark contrast to the general population, where premenopausal women are largely protected. ASCVD events and mortality are two to four times higher in patients with type 2 DM, correlating with both fasting/postprandial glucose and HbA1c levels. — Harrison's Principles of Internal Medicine, 22E
Coronary artery disease (CAD) in diabetes has several distinguishing features:
- Onset at a younger age than in the non-diabetic population
- More atypical clinical presentations (including silent ischemia, due to autonomic neuropathy blunting pain perception)
- Worse prognosis after MI
- Less satisfactory results from percutaneous coronary intervention (PCI)
- More diffuse, multivessel disease
Glycemic Control and CHD
Every 1% rise in HbA1c is associated with a 40% increase in cardiovascular mortality. In type 1 DM, the Diabetes Control and Complications Trial (DCCT) and its long-term follow-up (EDIC) demonstrated that intensive glycemic control during the early years after diagnosis confers lasting cardiovascular protection — the concept of "metabolic memory" or legacy effect. In type 2 DM, large trials (ACCORD, ADVANCE, VADT) failed to show that aggressive glycemic lowering alone reduces ASCVD events, underlining the importance of multifactorial risk reduction. — Harrison's Principles of Internal Medicine, 22E
Treatment of CHD in Diabetes
- Glycemic control: Target HbA1c <7% (≤53 mmol/mol), particularly in the early years after diagnosis
- Lipid management: High-intensity statin therapy (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) with an LDL goal <55 mg/dL in those with established ASCVD; add ezetimibe or a PCSK9 inhibitor if goals are not met
- Blood pressure: Target <130/80 mmHg; ACE inhibitors or ARBs are preferred first-line agents
- Antiplatelet therapy: Aspirin 81–325 mg/day for secondary prevention; also considered for primary prevention in those over 40 years with diabetes and CV risk factors
- Revascularization: In multivessel coronary disease, coronary artery bypass grafting (CABG) gives better outcomes than PCI with drug-eluting stents in terms of reduced all-cause mortality and non-fatal MI. — Goldman-Cecil Medicine
Novel Cardioprotective Agents
Certain glucose-lowering drugs provide CV benefit independent of their glycemic effect:
- SGLT2 inhibitors (empagliflozin, canagliflozin, dapagliflozin): Reduce MACE, cardiovascular death, HF hospitalization, and progression of CKD
- GLP-1 receptor agonists (liraglutide, semaglutide, dulaglutide): Reduce MACE and cardiovascular mortality in high-risk patients
The ADA/EASD consensus recommends preferential use of these agents in individuals with established atherosclerotic CVD, heart failure, or CKD. — Washington Manual of Medical Therapeutics
4. Heart Failure
Epidemiology
Heart failure (HF) is more common and carries a worse prognosis in persons with diabetes. The hazard ratio for developing HF in those with prediabetes is 1.2–1.7; in those with established diabetes, the HR rises to approximately 2.5. Survival after HF diagnosis is substantially worse in those with diabetes. — Washington Manual of Medical Therapeutics
Diabetic Cardiomyopathy
Distinct from ischemic cardiomyopathy, diabetes can cause a primary cardiomyopathy from direct metabolic injury to the myocardium. Features include:
- Left ventricular concentric remodeling and hypertrophy
- Diastolic dysfunction (often preceding systolic dysfunction)
- Impaired myocardial energetics and altered substrate utilization
- These changes are not directly attributable to coronary artery disease or hypertension
Management
- SGLT2 inhibitors are the agents of choice — they consistently reduce HF hospitalization in both HFrEF and HFpEF. If both CKD and HF are prominent, SGLT2 inhibitors are the preferred agents.
- Thiazolidinediones cause fluid retention and are contraindicated in HF
- Saxagliptin and alogliptin (DPP-4 inhibitors) showed increased HF risk in CVOTs; other DPP-4 inhibitors are neutral
- GLP-1 receptor agonists are neutral in established HF but beneficial for ASCVD prevention
5. Cerebrovascular Disease
Stroke and transient ischaemic attacks are significant macrovascular manifestations. Diabetes roughly doubles the risk of ischaemic stroke. Mechanisms include accelerated large-vessel atherosclerosis (particularly of the carotids and intracranial vessels), small-vessel lacunar disease, and a prothrombotic state.
Aggressive control of hypertension, lipids, and glucose — along with antiplatelet therapy — forms the basis of both primary and secondary prevention of cerebrovascular events. Clopidogrel has additional benefits over aspirin in the setting of peripheral and cerebrovascular disease in diabetic patients. — Washington Manual of Medical Therapeutics
6. Peripheral Arterial Disease (PAD)
Risk and Epidemiology
Diabetes and smoking are the two strongest risk factors for PAD. Gangrene of the lower extremities is approximately 100 times more common in individuals with diabetes than in the general population, making diabetes the leading cause of non-traumatic lower extremity amputation in the United States. PAD risk in diabetes is increased by advancing age, longer disease duration, and coexistent peripheral neuropathy. — Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine, 22E
PAD is a systemic vascular disease marker: patients with diabetes and PAD have increased risk for subsequent MI and stroke regardless of PAD symptoms.
Clinical Features
Symptoms include:
- Intermittent claudication
- Rest pain
- Tissue loss and non-healing ulcers
- Gangrene
However, diabetic patients with concomitant peripheral neuropathy may present with fewer symptoms, making the disease more insidious and advanced at detection. Physical signs include diminished peripheral pulses, dependent rubor, pallor on elevation, loss of hair, dystrophic nails, and cool dry fissured skin.
Diagnosis
The ankle-brachial index (ABI) — the ratio of systolic blood pressure at the ankle to that at the brachial artery — is the best initial diagnostic test. An ABI <0.9 (measured by a 5–10 MHz Doppler probe) has 95% sensitivity for detecting angiogram-positive PVD. The ADA recommends screening for asymptomatic PAD in patients over 50 years with diabetes and additional risk factors. — Washington Manual of Medical Therapeutics
Treatment
- Aggressive control of all cardiovascular risk factors (BP, lipids, glucose, smoking cessation)
- Antiplatelet therapy: Clopidogrel 75 mg/day has additional benefit over aspirin in diabetic patients with PAD
- Exercise rehabilitation and cilostazol (100 mg bid) benefit patients with intermittent claudication (cilostazol is contraindicated in CHF)
- Revascularization (endovascular or surgical) for critical limb ischaemia
Lower Extremity Complications and the Diabetic Foot
The "diabetic foot" arises from the convergence of PAD, peripheral sensory neuropathy, motor neuropathy, and autonomic neuropathy:
- Sensory neuropathy abolishes protective pain sensation, enabling unnoticed trauma
- Disordered proprioception causes abnormal weight-bearing and callus/ulcer formation
- Motor neuropathy leads to structural deformities (hammer toe, claw toe, Charcot joint)
- Autonomic neuropathy causes anhidrosis, altered superficial blood flow, skin dryness, and fissure formation
- PAD impairs wound healing
Risk factors for foot ulcers and amputation: male sex, diabetes >10 years, peripheral neuropathy, foot deformity, smoking, history of prior ulcer/amputation, poor glycemic control, and diabetic nephropathy/dialysis. — Harrison's Principles of Internal Medicine, 22E
Prevention through regular foot examination and patient education is paramount. All patients with DM should have an annual foot examination; those with sensory loss, deformity, or non-healing ulcers should be referred to a specialist.
7. Risk Factor Management — The Multifactorial Approach
Given the multifactorial nature of macrovascular disease, risk factors must be treated comprehensively:
| Risk Factor | Target / Intervention |
|---|---|
| HbA1c | <7% (individualized); avoid hypoglycemia |
| Blood pressure | <130/80 mmHg; ACE inhibitor or ARB first-line |
| LDL cholesterol | <55 mg/dL (with ASCVD); high-intensity statin ± ezetimibe/PCSK9i |
| Triglycerides/HDL | Lifestyle, fibrates if severely elevated |
| Smoking | Cessation — mandatory |
| Obesity | Weight loss; GLP-1 RA preferred |
| Antiplatelet | Aspirin (secondary prevention); consider in primary prevention >40 years |
| Preferred antidiabetics | SGLT2i (HF/CKD prominent); GLP-1 RA (ASCVD prominent) |
Every 1% rise in HbA1c increases cardiovascular mortality by 40%. Aggressive glycemic control reduces cardiovascular events by about 60% in type 1 DM. In type 2 DM, the overall CV benefit depends more on the specific drug class chosen than on the degree of glycemic lowering per se. — Goldman-Cecil Medicine
8. Key Landmark Trials
| Trial | Population | Key Finding |
|---|---|---|
| DCCT/EDIC | Type 1 DM | Intensive glycemic control reduces macrovascular events (legacy effect) |
| UKPDS | Type 2 DM (newly diagnosed) | Intensive control reduces microvascular risk; modest macrovascular benefit |
| EMPA-REG OUTCOME | Type 2 DM + CVD | Empagliflozin: ↓CV death, ↓HF hospitalization |
| LEADER | Type 2 DM + CVD | Liraglutide: ↓MACE, ↓CV mortality |
| SUSTAIN-6 | Type 2 DM + CVD | Semaglutide: ↓MACE |
| ACCORD | Type 2 DM | Intensive glycemia alone did not reduce MACE; increased mortality in those <7% HbA1c arm |
9. Conclusion
Macrovascular complications of diabetes mellitus encompass coronary heart disease, heart failure, cerebrovascular disease, and peripheral arterial disease. They arise from accelerated atherosclerosis driven by hyperglycemia, insulin resistance, dyslipidemia, endothelial dysfunction, and a prothrombotic state — all amplified by co-morbid hypertension. These complications are responsible for the majority of diabetes-related mortality. Effective prevention and management require a multifactorial approach: optimizing glycemia (particularly with SGLT2 inhibitors and GLP-1 receptor agonists in high-risk patients), aggressive lipid and blood pressure control, antiplatelet therapy, smoking cessation, and regular surveillance for peripheral vascular disease and foot complications.
Sources:
- Robbins & Kumar Basic Pathology — Chronic Complications of Diabetes
- Harrison's Principles of Internal Medicine, 22E — Diabetes Mellitus Complications
- Goldman-Cecil Medicine, International Edition — Diabetic Cardiovascular Disease
- Washington Manual of Medical Therapeutics — Macrovascular Complications of Diabetes Mellitus
This is a shared conversation. Sign in to Orris to start your own chat.