congenital heart defects in adults and differential diagnosis also
Reading File
Finding Sources
Finding Sources
Searching PubMed
"congenital heart disease" AND adults
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have comprehensive material to write a thorough, well-organized response. Let me compile it.
Congenital Heart Defects in Adults (ACHD) - Differential Diagnosis
Sources: Goldman-Cecil Medicine (Ch. 55), Robbins Basic Pathology, Tintinalli's Emergency Medicine
Overview
An estimated 2.4 million people in the United States currently live with congenital heart disease (CHD), and two thirds of them are adults. Congenital heart defects occur in ~1% of births; an overall adult prevalence of 3-4 per 1000 has been documented. Thanks to advances in pediatric surgery and cardiology, patients with even complex lesions now routinely survive into adulthood, making recognition and management of adult congenital heart disease (ACHD) a core competency.
Classification Framework
CHD in adults is best organized into three hemodynamic categories:
| Category | Mechanism | Examples |
|---|---|---|
| Left-to-right shunts (acyanotic initially) | Increased pulmonary blood flow; may progress to Eisenmenger syndrome | ASD, VSD, PDA, AVSD |
| Right-to-left shunts (cyanotic) | Bypassed pulmonary circulation; systemic desaturation | Tetralogy of Fallot, Ebstein anomaly, tricuspid atresia, truncus arteriosus, transposition |
| Obstruction | Reduced flow through a chamber, valve, or vessel | Pulmonary stenosis, aortic stenosis (bicuspid AV), coarctation of the aorta |
A useful mnemonic for cyanotic lesions is the "5 Ts": Tetralogy of Fallot, Tricuspid anomalies (atresia/Ebstein), Truncus arteriosus, Total anomalous pulmonary venous return, and Transposition of the great arteries.
Specific Defects in Adults
1. Bicuspid Aortic Valve (BAV)
- Most common congenital cardiac anomaly in adult populations, present in ~2% of the general population
- Accounts for up to half of surgical aortic stenosis cases in adults
- Clinical: Systolic ejection click + murmur; progressive AS or AR; aortic root dilation/dissection risk
- Complications: Infective endocarditis, aortic coarctation association, aortopathy
- Differential: Acquired/calcific tricuspid AS (older patients), rheumatic AS, hypertrophic obstructive cardiomyopathy (HOCM)
2. Atrial Septal Defect (ASD)
- Constitutes 30-40% of CHD in adults; ostium secundum ASD accounts for 7% of all congenital lesions
- Types: Ostium secundum (most common), ostium primum, sinus venosus, coronary sinus
- Clinical: Often silent for decades. Presents in 3rd-5th decade with exertional dyspnea, atrial fibrillation, RV volume overload. Fixed splitting of S2 is the hallmark auscultatory finding. Pulmonary hypertension develops after the 4th decade; Eisenmenger syndrome occurs in 5-10%.
- ECG: Right bundle branch block (rSR' pattern in V1), right axis deviation in secundum ASD; left axis deviation in primum ASD
- Echocardiographic finding: Left-to-right flow across the atrial septum on color Doppler (see figure below)
- Differential: Pulmonary hypertension (primary or secondary), right heart failure from any cause, mitral stenosis, anomalous pulmonary venous drainage
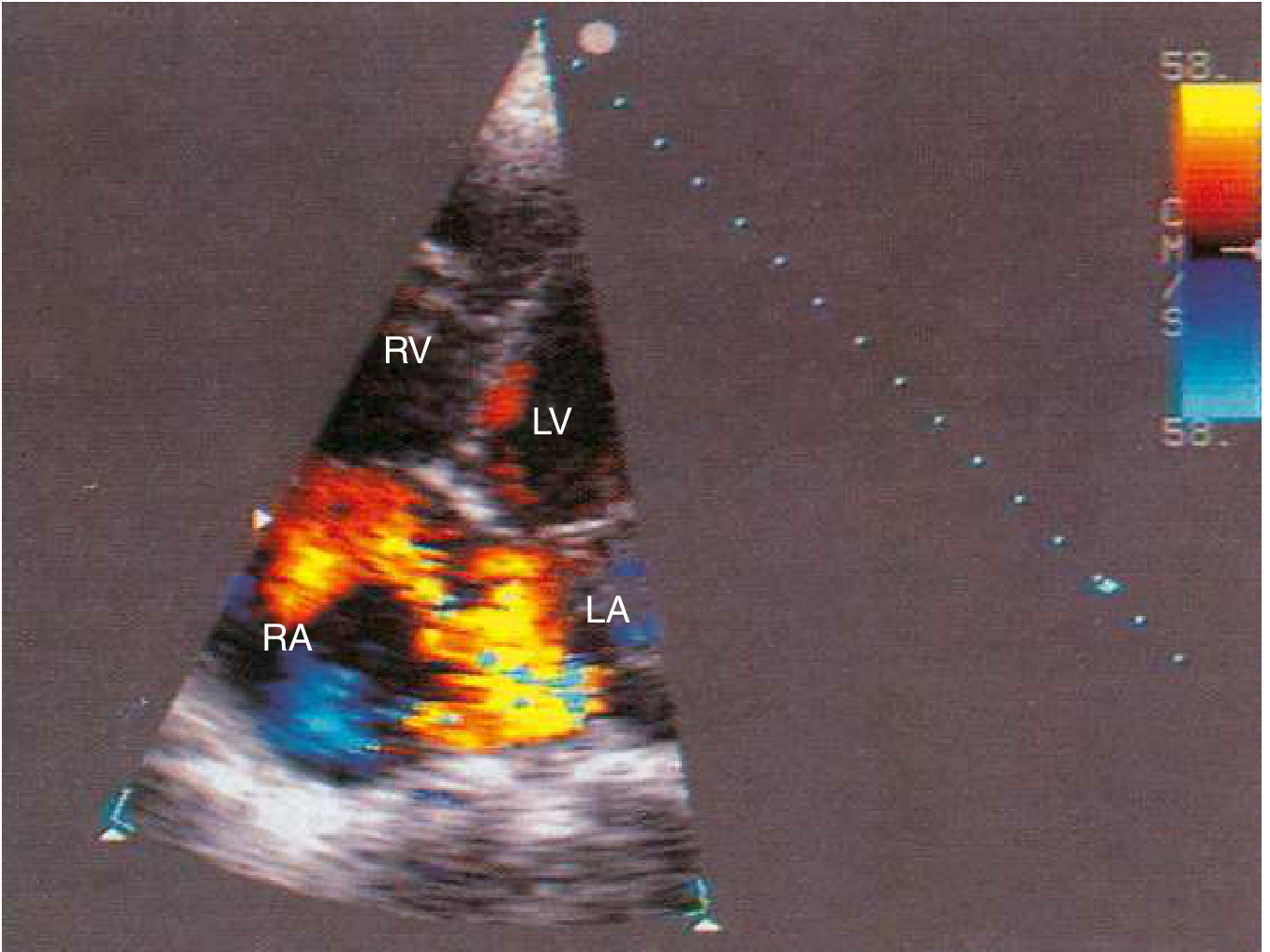
Color flow Doppler apical four-chamber view - blood flow from LA to RA through a moderately sized ASD. (Goldman-Cecil Medicine)
3. Ventricular Septal Defect (VSD)
- Most common congenital lesion in children (15-20% of all CHD); less prevalent in adults due to high spontaneous closure rates
- Types: Perimembranous (up to 80%), infundibular/supracristal, inlet, muscular/trabecular
- Clinical: Small (restrictive) VSDs - asymptomatic with a harsh holosystolic murmur at the left sternal border. Moderate/large VSDs - LV volume overload, pulmonary hypertension, dyspnea. Eisenmenger complex develops in ~10% of unrestricted VSDs.
- Differential: Mitral regurgitation (murmur radiates to axilla), tricuspid regurgitation, HOCM (murmur increases with Valsalva), aortic stenosis
4. Patent Ductus Arteriosus (PDA)
- Accounts for 5-10% of all CHD in infants with normal birthweight
- Clinical: Small PDAs - asymptomatic. Moderate/large PDAs - continuous "machinery" murmur at left infraclavicular area, wide pulse pressure, LV volume overload. Eisenmenger reversal causes lower-limb cyanosis and clubbing (differential cyanosis).
- Differential: Aortic regurgitation + stenosis, coronary arteriovenous fistula, sinus of Valsalva aneurysm rupture, aortopulmonary window
Left-to-right shunt diagram (ASD, VSD, PDA):
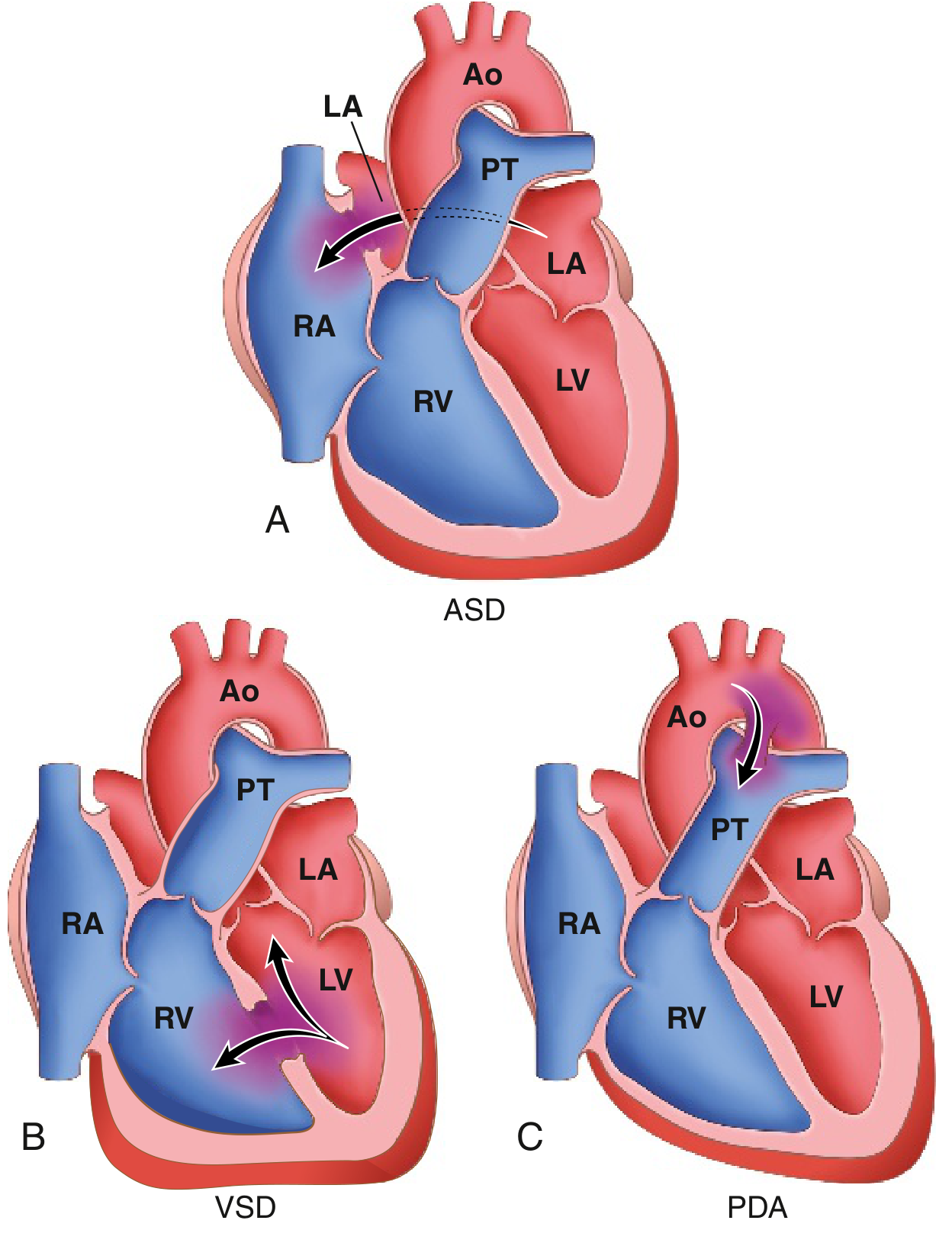
FIG. Common congenital causes of left-to-right shunts. (A) ASD - flow across atrial septum. (B) VSD - bidirectional turbulence across interventricular septum. (C) PDA - aorta-to-pulmonary trunk shunt. (Robbins Basic Pathology)
5. Pulmonary Stenosis
- Accounts for 3-10% of all congenital lesions
- Clinical: Mild-moderate PS is usually well-tolerated into adulthood. Severe PS causes exertional dyspnea, RV hypertrophy, right heart failure. Ejection click that decreases with inspiration + crescendo-decrescendo systolic murmur at LUSB with radiation to the back.
- Differential: Atrial septal defect, dynamic RVOT obstruction in HOCM, pulmonary artery stenosis, tetralogy of Fallot
6. Coarctation of the Aorta
- 3-10% of CHD; associated with bicuspid aortic valve in up to 50% of cases; Turner syndrome association
- Clinical hallmarks:
- Hypertension in upper extremities, reduced pressure and weak/delayed pulses in lower extremities
- Blood pressure differential: arm systolic > popliteal systolic; >30 mmHg difference between right and left arms if left subclavian artery is involved
- Systolic murmur heard posteriorly in the mid-thoracic region
- Systolic ejection click from associated BAV
- Collateral flow murmurs in infraclavicular areas
- CXR: Classic "3 sign" (dilated left subclavian artery + descending aorta indentation) and posterior rib notching of 3rd-8th ribs
- Differential: Essential hypertension, renal artery stenosis, Takayasu arteritis (in young women), mid-aortic syndrome
7. Tetralogy of Fallot (TOF)
Most common cyanotic congenital anomaly in adults. Comprises 4 features:
- Pulmonary stenosis (infundibular, most common)
- Ventricular septal defect (large, perimembranous)
- Overriding aorta
- Right ventricular hypertrophy
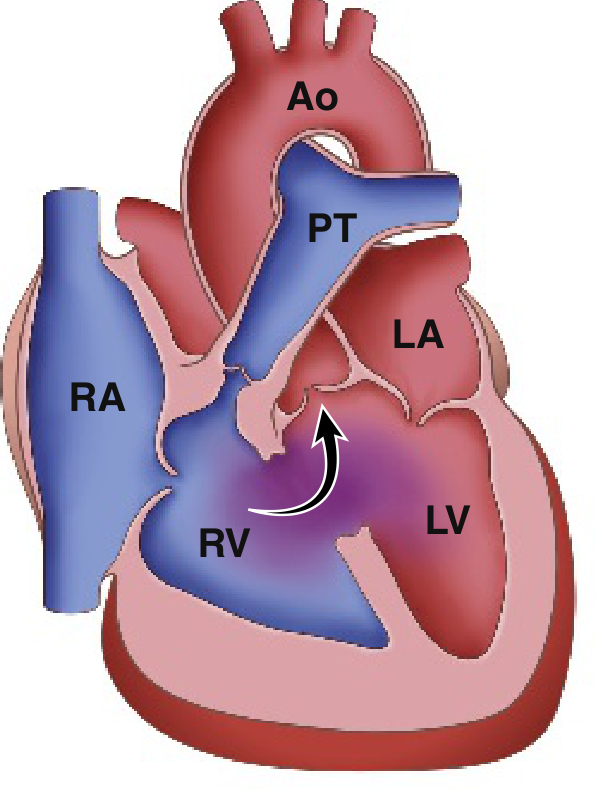
Classic Tetralogy of Fallot: right-to-left shunting through large VSD with overriding aorta. PT = pulmonary trunk, Ao = aorta. (Robbins Basic Pathology)
- Clinical: Cyanosis (degree depends on severity of RV outflow obstruction), clubbing, polycythemia, hypertrophic osteoarthropathy. "Boot-shaped" heart on CXR (coeur en sabot). Most adults have had prior surgical repair; residual complications include pulmonary regurgitation, RV dilation/failure, arrhythmias, and sudden cardiac death.
- Genetic: 15% have 22q11 deletion (DiGeorge/CATCH-22 syndrome)
- CXR post-repair: Right aortic arch, upturned RV apex, sternal wires
- Differential: Large VSD with Eisenmenger, primary pulmonary hypertension, double-outlet right ventricle, pulmonary atresia with VSD
8. Ebstein Anomaly
- Apical displacement of the tricuspid valve leaflets (particularly the septal and posterior leaflets) into the RV, causing "atrialization" of a portion of the RV
- Clinical: Wide spectrum from severe neonatal presentation to incidental adult diagnosis. Symptoms include cyanosis (via ASD/PFO with R-to-L shunting), exercise intolerance, palpitations (accessory pathways, WPW syndrome in up to 25%). Characteristic auscultatory finding: "sail sound" (loud widely split S1 from tricuspid closure), triple or quadruple rhythm.
- ECG: Right bundle branch block, tall peaked P waves, delta waves if WPW
- Differential: Tricuspid regurgitation (any cause), dilated cardiomyopathy with TR, ASD, RV cardiomyopathy (ARVC)
9. Transposition of the Great Arteries (TGA) - Congenitally Corrected TGA (ccTGA)
- Simple TGA (D-TGA): Rarely reaches adulthood unrepaired; adults are almost always post-Mustard/Senning repair or arterial switch operation, each with specific late complications (baffle obstruction, systemic RV failure, arrhythmias)
- Congenitally corrected TGA (ccTGA/L-TGA): AV and ventriculo-arterial discordance that is "physiologically corrected." The systemic ventricle is the morphologic RV, which tends to fail over decades. Adults may present with TR, complete heart block, or heart failure.
- Differential: Dilated cardiomyopathy, complex RV failure, ARVC
10. Sinus of Valsalva Aneurysm
- A previously asymptomatic young man typically presents with acute chest pain and rapidly progressive dyspnoea (sometimes after physical exertion) due to rupture into the right heart
- Rupture creates a large left-to-right shunt; continuous "to-and-fro" murmur
- Differential: PDA, aortic regurgitation, coronary AV fistula
11. Anomalous Coronary Arteries
- Present in 0.6-1.5% of patients undergoing coronary angiography
- Most dangerous: left main or LAD arising from the right sinus and coursing between the aorta and pulmonary artery (risk of ischemia, MI, sudden death with exertion)
- Clinical: Exertional chest pain, syncope, sudden cardiac death in young athletes
- Differential: Premature CAD, HOCM, exercise-induced spasm, myocarditis
Eisenmenger Syndrome
When any large left-to-right shunt (ASD, VSD, PDA, AVSD) remains uncorrected, chronic exposure of the pulmonary vasculature to elevated pressure and flow causes irreversible pulmonary vascular remodeling. This raises pulmonary vascular resistance until it exceeds systemic resistance, reversing the shunt (right-to-left), causing cyanosis, clubbing, and polycythemia. Key features:
- Late cyanosis (central, differential in PDA)
- Clubbing and polycythemia
- Symptoms of right heart failure
- Once established, structural repair is contraindicated (defect acts as a "pop-off valve")
- Treatment: pulmonary vasodilators (bosentan, sildenafil, prostacyclins), transplant
Differential Diagnosis Summary Table
| Presentation | Primary ACHD Diagnoses | Non-CHD Differentials |
|---|---|---|
| Exertional dyspnea + fixed split S2 | ASD (ostium secundum) | Primary pulmonary hypertension, right heart failure |
| Harsh holosystolic murmur, LLSB | VSD | Mitral regurgitation, tricuspid regurgitation, HOCM |
| Continuous "machinery" murmur | PDA | Sinus of Valsalva aneurysm rupture, coronary AV fistula, aortopulmonary window |
| Upper limb hypertension + weak femoral pulses | Coarctation of the aorta | Essential HTN, Takayasu arteritis, renal artery stenosis |
| Cyanosis + clubbing + polycythemia | Eisenmenger syndrome, TOF, Ebstein anomaly | Pulmonary AV malformation, severe COPD/IPF, hepatopulmonary syndrome |
| Systolic ejection murmur + click + aortopathy | Bicuspid aortic valve | Degenerative/calcific AS, rheumatic AS, HOCM |
| Young athlete + exertional syncope/SCD | Anomalous coronary artery, TOF, Ebstein | HOCM, WPW, long QT, myocarditis, ARVC |
| RV failure + AV block + palpitations | ccTGA, Ebstein anomaly | Dilated cardiomyopathy, ARVC, amyloidosis |
| Acute chest pain + new continuous murmur (young adult) | Sinus of Valsalva aneurysm rupture | Aortic dissection, acute MI, pericarditis |
General Diagnostic Approach in Adults
- History: Prior surgeries, cardiac catheterizations, known diagnosis in childhood, family history of CHD or genetic syndromes
- Physical exam: Cyanosis, clubbing, differential cyanosis (PDA), blood pressure in all 4 limbs, character and location of murmurs, S2 splitting, precordial heave
- ECG: RV hypertrophy/strain, bundle branch blocks, axis deviation, pre-excitation (WPW in Ebstein), arrhythmias
- CXR: Cardiomegaly, pulmonary vascular markings (plethora vs. oligemia), rib notching (coarctation), "3 sign," boot-shaped heart (TOF), situs
- Echocardiography: First-line modality; assesses anatomy, shunt direction/quantification (Qp:Qs), ventricular function, pressures
- Cardiac MRI: Gold standard for RV volumes, TOF residua, complex anatomy, coarctation
- Cardiac CT angiography: Coronary anomalies, aortic anatomy, vascular structures
- Cardiac catheterization: Hemodynamic assessment (pulmonary vascular resistance), vasoreactivity testing before repair decisions in pulmonary hypertension
Genetic Associations to Keep in Mind
| Syndrome | Associated Defects |
|---|---|
| Down syndrome (trisomy 21) | Endocardial cushion defects (AVSD), VSD |
| Turner syndrome (45,X) | Coarctation, BAV, ASD |
| DiGeorge/22q11 deletion | TOF, interrupted aortic arch, truncus arteriosus, VSD |
| Marfan syndrome | Aortic root dilation, MVP |
| Holt-Oram syndrome | ASD, VSD, heart block |
| Noonan syndrome | Pulmonary stenosis, HCM |
Key Clinical Pearls:
- Any adult with an unexplained stroke, TIA, or systemic embolism should be screened for PFO or ASD (paradoxical embolism)
- Differential cyanosis (lower limbs only) + clubbing in a young adult = PDA with Eisenmenger reversal
- New continuous murmur + acute dyspnea in a previously well young adult = suspect sinus of Valsalva aneurysm rupture
- Exertional syncope in a young athlete = coronary anomaly until proven otherwise (also consider HOCM, long QT, ARVC)
- All patients with repaired or unrepaired CHD need prophylaxis consideration; high-risk lesions (unrepaired cyanotic CHD, prosthetic valves, post-repair residua) require endocarditis prophylaxis for dental procedures
Sources: Goldman-Cecil Medicine International Edition (Ch. 55 - Congenital Heart Disease in Adults); Robbins & Kumar Basic Pathology (Ch. 9); Tintinalli's Emergency Medicine (Ch. 129)
This is a shared conversation. Sign in to Orris to start your own chat.