Alveolar macrophage full details for md exams 15marks
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
alveolar macrophage lung function phagocytosis
I now have comprehensive content. Let me compile the full 15-mark MD exam answer on alveolar macrophages.
Alveolar Macrophages — Comprehensive Notes (15 Marks)
1. Introduction & Definition
Alveolar macrophages (AMs) are the principal resident immune effector cells of the lung. They inhabit the alveolar lumen, residing at the interface of the epithelial lining fluid and ambient inhaled air. They are the "sentinels" of the alveolar compartment, constituting the first line of defence against inhaled microbes, particulates, and antigens.
2. Origin & Development
Embryonic Origin
AMs have a unique dual origin unlike most tissue macrophages:
| Source | Marker Profile | Transcription Factor |
|---|---|---|
| Yolk sac (primary, embryonic day E8) | F4/80-high, CX3CR1+, CSF1R+ | PU.1, dependent on IL-34 & CSF1 |
| Fetal liver (E10.5 onward) | F4/80-low, CD11b-high | c-Myb |
| Bone marrow monocytes (postnatal replenishment) | CD11b+, Ly6C+ | — |
- Yolk sac-derived macrophages populate the lung early in embryogenesis and are capable of self-renewal, persisting as long-lived tissue-resident cells.
- The fetal liver and postnatal bone marrow contribute to interstitial macrophages and, to a lesser extent, to alveolar macrophages during steady state and after injury.
Key point: Alveolar macrophages are primarily derived from the yolk sac, while interstitial macrophages are predominantly derived from the fetal liver and circulating monocytes — a distinction in origin that correlates with distinct transcriptional signatures and functions.
— Murray & Nadel's Textbook of Respiratory Medicine, p. 336
3. Morphology & Identification
- Large, mononuclear cells with an abundant, vacuolated cytoplasm
- Contain secondary lysosomes and phagosomes filled with ingested material
- Stain strongly for non-specific esterase (monocyte lineage marker)
- Surface markers: CD68+, CD11c+ (high), SiglecF+ (mouse), CD206+
- Distinct from interstitial macrophages by their transcriptional signature, location, and function
- In smokers and heavily polluted environments, they appear "dust-laden" or "soot-laden" (visible carbon/particle inclusions)
4. Location
- Reside in the alveolar lumen, lying on the alveolar epithelial surface (type I and type II pneumocytes)
- Exist within the mixed environment of epithelial lining fluid (surfactant, immunoglobulins, defensins) and inhaled air
- Also present in terminal bronchioles (as "bronchioloalveolar macrophages")
- The pool is maintained by a combination of local self-renewal and slow recruitment from blood monocytes
5. Primary Functions
A. Phagocytosis of Microbes and Particulates (most important function)
- AMs phagocytose a wide spectrum of inhaled microbes (bacteria, fungi, viruses) and inert particulates (dust, carbon, silica)
- Under basal conditions: particulates are enclosed in phagosomes → fuse with lysosomes → degraded by acid-pH hydrolytic enzymes
- Resistant organisms (e.g., Mycobacterium tuberculosis) and insoluble particles (e.g., crystalline silica) evade degradation and become sequestered in secondary lysosomes for the life span of the macrophage
- Particle-laden macrophages are cleared via the mucociliary escalator (crawl into airways) or undergo apoptosis and are cleared by neighbouring phagocytes
- Some macrophages remain in the lung for extended periods, die, and release their particle burden for re-phagocytosis
B. Clearance of Pulmonary Surfactant
- AMs actively contribute to normal surfactant homeostasis — they engulf and catabolise excess surfactant lipids and proteins
- This function is critically highlighted in Pulmonary Alveolar Proteinosis (PAP):
- Characterised by accumulation of proteinaceous, lipid-rich surfactant in alveoli → impaired gas exchange
- AM numbers are reduced, and those present are inefficient in surfactant clearance
- PAP is associated with anti-GM-CSF autoantibodies, underscoring the importance of GM-CSF for AM function (GM-CSF drives AM differentiation via PU.1)
- Surfactant proteins SP-A and SP-D suppress AM phagocytosis via interaction with SIRP-α, modulating immune tone
C. Tonic Suppression of Inflammation and Adaptive Immunity (critical regulatory role)
- AMs play a critically important role in tonic suppression of alveolar inflammation and adaptive immunity
- The concept: the lung tolerates inhaled microbes/particulates until a threshold burden is reached
- Below threshold → AMs phagocytose and degrade → no inflammatory response
- Above threshold → microbes are taken up by resident dendritic cells (DCs) that "snorkel" through tight junctions of the alveolar epithelium
- DCs then augment adaptive immune responses
- Experimental evidence: depletion of AMs with liposome-encapsulated clodronate → augments antigen presentation by pulmonary DCs → augments adaptive immune responses to intratracheal antigens
- This suppressive function prevents inappropriate inflammation to harmless inhaled antigens
— Murray & Nadel's Textbook of Respiratory Medicine, p. 337
6. Pattern Recognition Receptors (PRRs)
AMs express a broad array of PRRs to recognise both PAMPs (pathogen-associated molecular patterns) and DAMPs:
| Receptor Class | Examples | Ligands |
|---|---|---|
| Toll-like receptors (TLRs) | TLR2, TLR4, TLR9 | Lipoteichoic acid, LPS, CpG DNA |
| Scavenger receptors | MARCO, SR-AI/II | Oxidised lipids, particulates, bacteria |
| Lectin receptors | Mannose receptor (CD206), Dectin-1 | Fungal β-glucan, mannosylated pathogens |
| Complement receptors | CR1 (CD35), CR3 (CD11b/CD18) | Opsonised particles (C3b, iC3b) |
| Fc receptors | FcγRI, FcγRII, FcγRIII | IgG-opsonised particles |
| CD36 | CD36 | Diacylglycerides, Staphylococcus |
MARCO and SR-AI/II protect against inhaled oxidants by scavenging oxidised lipids — Murray & Nadel's, p. 338
7. Cytokine Production & Immunological Role
Pro-inflammatory (M1-like) activation — classical:
Triggered by IFN-γ, LPS, TNF-α
- Secrete: IL-1β, IL-6, IL-12, IL-18, TNF-α
- Enhanced ROS, NO production via iNOS
- Upregulate MHC class II → antigen presentation
- Anti-tumour, anti-microbial activity
Anti-inflammatory (M2-like) activation — alternative:
Triggered by IL-4, IL-10, IL-13, TGF-β, glucocorticoids, GM-CSF
- Secrete: IL-10, TGF-β, arginase-1
- Promote tissue repair, fibrosis, immune regulation
- Maintain alveolar homeostasis under steady-state conditions
Under basal/steady-state conditions, AMs are predominantly in an anti-inflammatory, immunosuppressive phenotype — this is physiologically important to prevent autoimmunity and inappropriate responses to harmless inhaled antigens.
Key cytokines secreted:
- TGF-β, IL-10, PGE₂: Suppress T-cell activation and DC maturation
- MCP-1 (CCL2): Recruit monocytes during infection
- IL-8 (CXCL8): Recruit neutrophils
- IL-12, IL-23: Link innate to adaptive immunity
8. Role of GM-CSF in AM Function
- GM-CSF (granulocyte-macrophage colony-stimulating factor) is essential for AM development and function
- Acts via PU.1 transcription factor to regulate:
- AM differentiation
- FcγR-mediated phagocytosis
- IL-18/IFN-γ axis (innate → adaptive immunity linkage)
- GM-CSF deficiency (or anti-GM-CSF antibodies) → failure of AM maturation → Pulmonary Alveolar Proteinosis
- Inhaled GM-CSF is used therapeutically in PAP
9. Transcriptional Signatures & Tissue Identity
- AMs have a unique transcriptional signature adapted to the lung environment
- All tissue-resident macrophages share core macrophage signature genes, but each displays organ-specific signatures
- Key AM-specific transcription factors: PU.1, C/EBPα, PPARγ (PPARγ is essential for AM identity — knockout mice develop PAP-like syndrome)
- Interstitial macrophages, by contrast, share a conserved transcriptional profile across multiple organs (lung, skin, heart, intestine), suggesting a common function in different tissues
10. AM vs. Interstitial Macrophage — Key Differences
| Feature | Alveolar Macrophage | Interstitial Macrophage |
|---|---|---|
| Location | Alveolar lumen | Lung interstitium |
| Origin | Yolk sac (primarily) | Fetal liver + circulating monocytes |
| Transcriptional profile | Tissue-specific, unique | Conserved across organs |
| Surface markers | F4/80-hi, CD11c-hi, SiglecF+ | F4/80-lo, CD11b-hi |
| Key function | Phagocytosis, surfactant clearance, immune suppression | Antigen presentation, inflammatory signalling |
11. Clinical Correlations (Exam High-Yield)
| Condition | AM Role |
|---|---|
| Pulmonary Alveolar Proteinosis (PAP) | AM deficiency/dysfunction → surfactant accumulation; anti-GM-CSF antibodies |
| Tuberculosis | M. tuberculosis survives in AM lysosomes; key pathogenesis step |
| Silicosis | Crystalline silica sequestered in lysosomes → NLRP3 inflammasome → fibrosis |
| COPD | Defective efferocytosis, M1 polarisation → chronic inflammation, emphysema |
| Sarcoidosis | AM-derived cytokines (IL-12, TNF-α) drive granuloma formation |
| Asthma | M2-polarised AMs → IL-10, TGF-β → modulate airway inflammation |
| Lung cancer | Tumour-associated macrophages (TAMs, M2-like AM) → pro-tumour, angiogenesis, immune suppression |
| Post-influenza bacterial pneumonia | IFN-γ from influenza suppresses AM antibacterial defences → secondary bacterial infection |
12. Summary Diagram of Functions
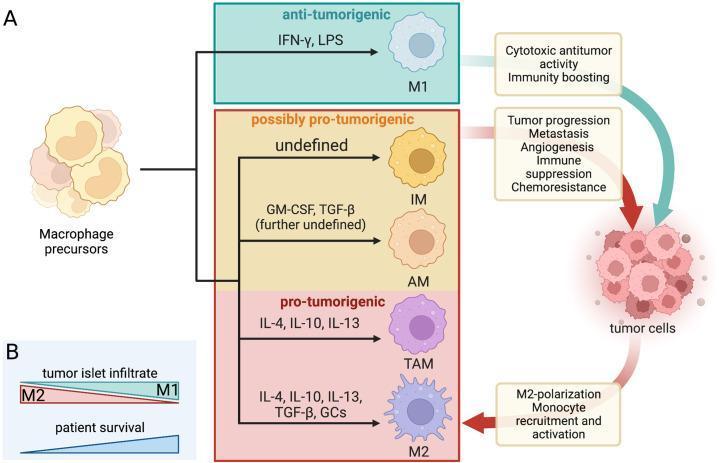
Macrophage polarization spectrum: M1 (IFN-γ/LPS-driven, anti-tumorigenic) vs. alveolar/M2 (IL-4/IL-10/GM-CSF-driven, homeostatic/pro-tumorigenic). Note the central role of alveolar macrophages.
13. Quick Recall Points for Exam
- Three primary functions: phagocytosis, surfactant clearance, immune suppression
- Origin: yolk sac (embryonic), self-renewing pool
- PAP = prototype disease of AM dysfunction (anti-GM-CSF Abs → PU.1 failure)
- GM-CSF → PU.1 is the master axis for AM development
- PPARγ is essential for AM identity
- M. tuberculosis exploits the AM — evades lysosomal fusion
- Silica → cannot be degraded → NLRP3 → IL-1β → fibrosis
- Depletion of AMs → enhances DC-mediated adaptive immunity (loss of tonic suppression)
- Surfactant proteins (SP-A, SP-D) modulate AM activity via SIRP-α
- Interstitial macrophages ≠ alveolar macrophages (different origin, transcriptome, function)
Sources: Murray & Nadel's Textbook of Respiratory Medicine (2-Volume); Fishman's Pulmonary Diseases and Disorders; Roitt's Essential Immunology; Janeway's Immunobiology 10e
This is a shared conversation. Sign in to Orris to start your own chat.