Short notes on Hdf modalities of HD and advantages disadvantages, also illustrates the hdf process is helpful over normal hemodialysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive textbook content. Let me compile the full answer.
Hemodiafiltration (HDF): Modalities, Advantages, Disadvantages & Comparison with HD
What is HDF?
Hemodiafiltration (HDF) combines the two fundamental mechanisms of solute removal:
| Mechanism | Used in | How it works |
|---|---|---|
| Diffusion | Hemodialysis (HD) | Concentration gradient drives small solutes across membrane |
| Convection | Hemofiltration (HF) | Hydrostatic pressure drives fluid + solutes (solvent drag) |
HDF = Diffusion (HD) + Convection (HF) using a high-flux membrane.
A large volume of fluid is removed by ultrafiltration (convective volume), and the excess volume beyond target weight loss is replaced by ultrapure infusion solution (substitution fluid).
Online HDF: The dialysis machine itself produces ultrapure, nonpyrogenic dialysate which is also used as the infusion solution — eliminating the need for pre-bottled substitution bags. High-volume HDF: Effective convection volume >23 L per dialysis session.
— Comprehensive Clinical Nephrology, 7th Ed.
HDF Circuit (How It Works)
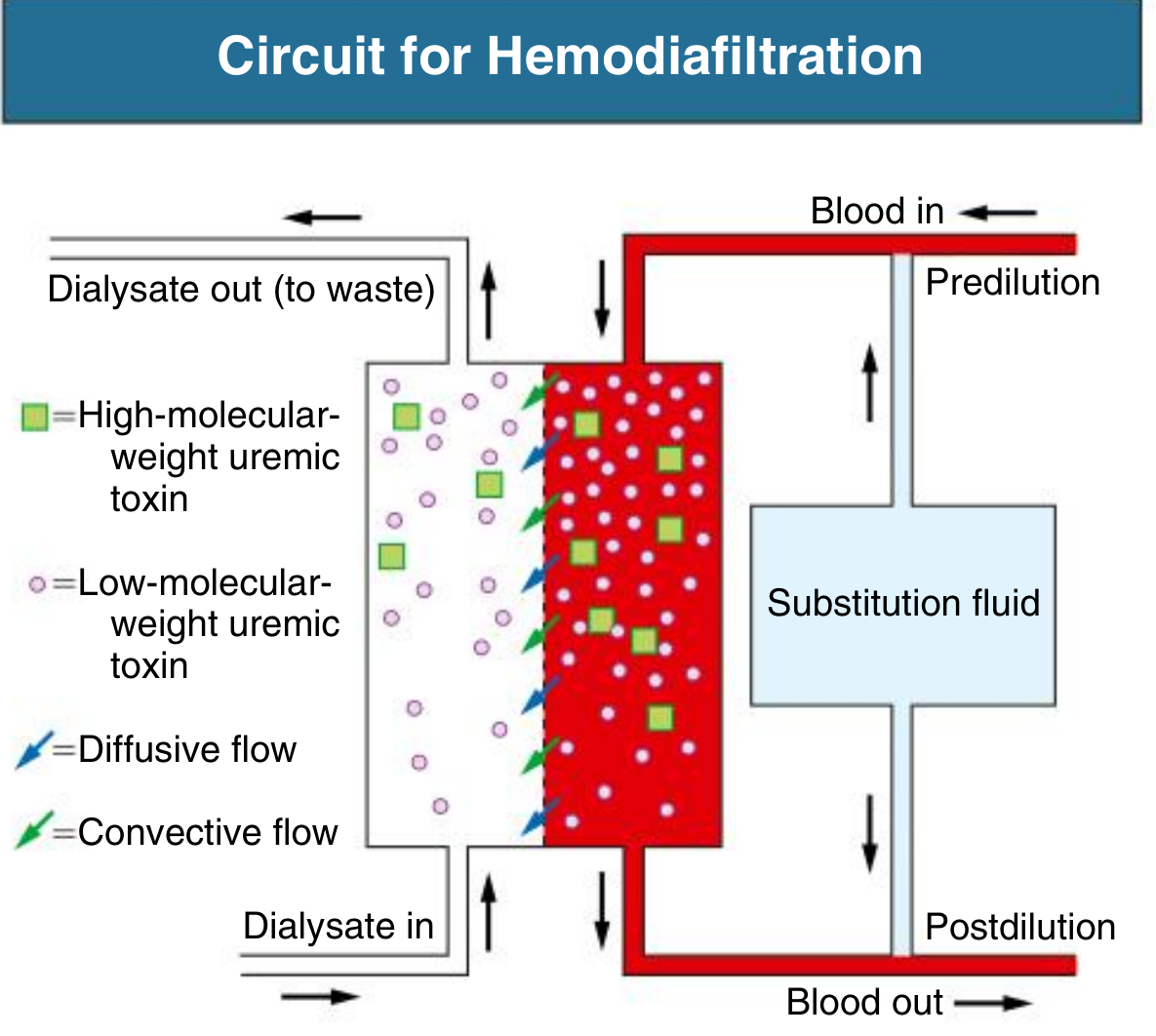
Circuit for Hemodiafiltration — substitution fluid can be administered predilution (upstream) or postdilution (downstream) of the dialyzer. Blue arrows = diffusive flow; green arrows = convective flow.
The key difference from standard HD:
- In HD: only dialysate on the other side of the membrane creates a concentration gradient (diffusion only). Small molecules removed well; large/middle molecules poorly.
- In HDF: dialysate flows AND a large ultrafiltrate volume is simultaneously driven across the membrane by pressure. Both small and large/middle molecules are cleared efficiently.
Modalities of HDF
HDF modalities are classified by the site of infusion of substitution fluid:
1. Postdilution HDF
- Substitution fluid infused downstream (after) the dialyzer
- Blood passes through the dialyzer undiluted → maximum solute removal efficiency
- Most efficient modality for increasing solute removal
- Limitation: hemoconcentration within the dialyzer limits achievable ultrafiltration rate (filtration fraction must be kept ≤25–30% to prevent membrane clogging)
2. Predilution HDF
- Substitution fluid infused upstream (before) the dialyzer
- Blood is diluted before entering the dialyzer → reduces transmembrane concentration gradient
- For an identical substitution volume, efficiency is lower than postdilution HDF
- Advantage: less hemoconcentration, allows higher ultrafiltration volumes safely; less protein deposition on membrane
3. Mixed Dilution HDF
- Substitution fluid infused both upstream and downstream of the dialyzer
- The ratio of upstream:downstream infusion can be varied
- Achieves an optimal compromise between maximizing clearance and avoiding the consequences of high transmembrane pressure and hemoconcentration
4. Mid-Dilution HDF
- Substitution fluid infused mid-way along specifically designed dialyzers
- The first portion of the dialyzer operates in postdilution mode (high efficiency)
- The second portion operates in predilution mode (less hemoconcentration)
- Designed to leverage the benefits of both modes within a single pass
5. Internal Filtration / Backfiltration (Passive HDF)
- In high-flux dialyzers, ultrafiltration dominates proximally and backfiltration of dialysate occurs distally — passively delivering convective clearance without added substitution fluid
- Concern: if dialysate is not ultrapure, backfiltration can introduce endotoxin fragments into blood, potentially worsening inflammation
- Medium cut-off membranes designed for high internal filtration/backfiltration to enhance clearance of middle molecules (e.g., complement factor D, free κ light chains, TNF-α, β₂-microglobulin)
— Comprehensive Clinical Nephrology, 7th Ed.
HDF Dose Prescription
| Parameter | Requirement |
|---|---|
| Membrane | High-flux; ultrafiltration coefficient >20 mL/h/mmHg/m²; sieving coefficient for β₂-microglobulin ≥0.6 |
| Blood flow (Qb) | High (typically 350–500 mL/min) |
| Dialysate flow | 500 mL/min |
| Convective volume target | >23 L/session (high-volume HDF); minimum 20% of total processed blood volume |
| Filtration fraction (FF) | FF = UFR/Qb; must not exceed 25% (up to 30% with modern machines) |
| Water quality | Ultrapure, virtually sterile and nonpyrogenic (stricter than standard HD requirements) |
— Comprehensive Clinical Nephrology, 7th Ed.
HDF vs. Standard Hemodialysis — Advantages & Disadvantages
Advantages of HDF over HD
| Advantage | Detail |
|---|---|
| Superior middle molecule clearance | β₂-microglobulin, complement factor D, free light chains, cytokines removed far more efficiently via convection |
| Reduced β₂-microglobulin levels | Lower predialysis levels compared to HD; associated with lower mortality in some studies |
| Less intradialytic hypotension | Meta-analyses and some RCTs show reduced hemodynamic instability during HDF sessions |
| Better cardiovascular outcomes (high-volume) | ESHOL study (~23 L/session): lower cardiovascular mortality, all-cause mortality, and hospitalization |
| Mimics glomerular filtration more closely | Combined diffusion + convection better replicates native kidney clearance, especially for patients with no residual kidney function |
| Potential reduction in all-cause mortality | High-volume HDF (>22 L convective volume/session) associated with mortality benefit in subgroup analyses of CONTRAST and OL-HDF trials |
| Better removal of protein-bound uremic toxins | Convective clearance augments removal of some protein-bound solutes (e.g., indoxyl sulfate, p-cresyl sulfate) |
Disadvantages / Limitations of HDF
| Disadvantage | Detail |
|---|---|
| High water quality demands | Requires ultrapure water (virtually sterile, pyrogen-free) — more stringent than standard HD |
| Complex, expensive equipment | Requires specialized machines capable of generating online infusate; not widely available (e.g., only one FDA-approved HDF device exists in the USA) |
| Regulatory restrictions | Online HDF not available in the United States for routine clinical use |
| Risk of amino acid and albumin loss | Convective flux can remove albumin, amino acids, vitamins (e.g., vitamin D-binding protein with medium cut-off membranes), and drugs like vancomycin |
| Higher cost | Large volumes of substitution fluid, specialized membranes, and advanced equipment increase cost |
| No proven benefit at low convection volumes | Benefits only demonstrated at high convective volumes (>22–23 L/session); low-volume HDF is no better than standard HD |
| Conflicting RCT evidence | CONTRAST and OL-HDF trials showed no overall difference in all-cause or cardiovascular mortality; benefit emerged only in post-hoc high-volume subgroup analyses |
| Endotoxin risk | Backfiltration with non-ultrapure dialysate can introduce endotoxin/bacterial fragments into blood |
| Hemoconcentration risk (postdilution) | Requires careful monitoring of filtration fraction to prevent protein deposition and dialyzer clogging |
Head-to-Head: HDF vs. HD — Clinical Trial Evidence
| Parameter | HD | HDF | Evidence |
|---|---|---|---|
| Small solute (urea) removal | Excellent | Equivalent | Trials show no difference |
| Middle molecule (β₂-microglobulin) removal | Moderate (high-flux HD) | Superior | Consistent across studies |
| Intradialytic hypotension | More common | Less common | Meta-analyses favor HDF |
| All-cause mortality (overall) | — | No significant difference | CONTRAST, OL-HDF |
| All-cause mortality (high-volume HDF >22 L) | — | Reduced | CONTRAST & OL-HDF subgroup; ESHOL overall |
| Cardiovascular mortality | — | Reduced (high-volume) | ESHOL study |
| ESA (erythropoietin) requirement | — | No difference | RCTs |
| Serum phosphate | — | No difference | RCTs |
| Quality of life | — | No consistent difference | RCTs |
| Left ventricular mass / pulse wave velocity | — | No significant difference | RCTs |
Key take-home: High-volume online HDF (>23 L convective volume/session) likely reduces cardiovascular and all-cause mortality and intradialytic hypotension, but standard or low-volume HDF offers no proven benefit over conventional HD.
— Brenner & Rector's The Kidney; Comprehensive Clinical Nephrology, 7th Ed.; NKF Primer on Kidney Diseases, 8th Ed.
Summary
HD = Diffusion only (concentration gradient)
HF = Convection only (solvent drag, no dialysate)
HDF = Diffusion + Convection (best of both)
HDF Modalities:
1. Postdilution → most efficient, hemoconcentration risk
2. Predilution → safer, less efficient
3. Mixed dilution → compromise of both
4. Mid-dilution → within-dialyzer hybrid
5. Internal filtration/backfiltration → passive, water quality critical
High-volume HDF (>23 L/session) = clinical benefit threshold
This is a shared conversation. Sign in to Orris to start your own chat.