Changes of respiratory system in pregnancy full details for md exams 15marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive MD-exam answer. Here is the full detailed response:
Changes of the Respiratory System in Pregnancy
Overview
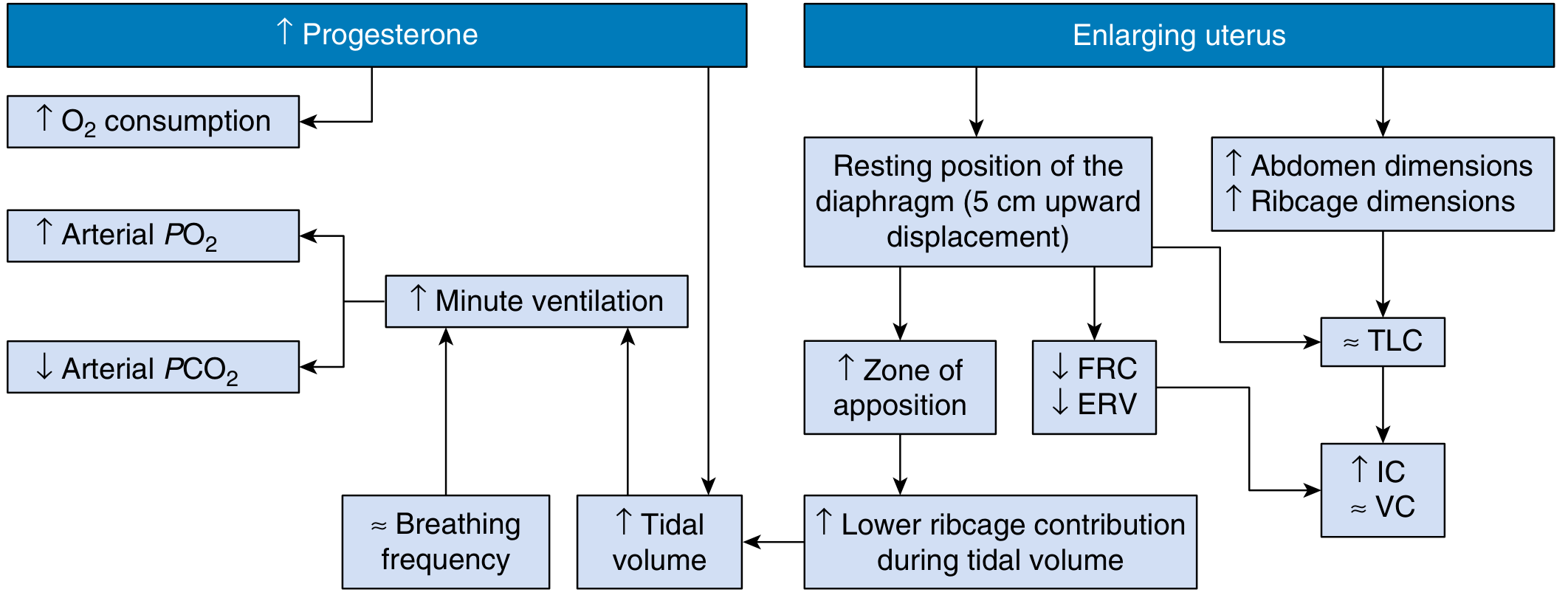
Pregnancy induces profound adaptive changes in the respiratory system driven by two key forces: hormonal (primarily progesterone) and mechanical (enlarging uterus). These changes begin as early as 6 weeks after fertilization and serve to optimize oxygen delivery to the fetus while eliminating fetal CO₂.
1. Anatomical / Structural Changes
| Structure | Change |
|---|---|
| Diaphragm | Displaced cranially by 4–5 cm |
| Subcostal angle | Widens from 68° → 103° (before mechanical pressure of uterus) |
| Transverse chest diameter | Increases by 2 cm |
| Chest circumference | Increases by ~5–7 cm |
| Nasal mucosa | Edema, hyperemia, glandular hypersecretion (gestational rhinitis) — driven by estrogen |
The diaphragm elevation occurs early, even before the uterus is large enough to cause direct mechanical pressure, indicating a hormonal (progesterone-mediated relaxing) component. Despite the higher resting position, diaphragm excursion actually increases by ~1.5 cm — so respiratory function is not impaired.
— Creasy & Resnik's Maternal-Fetal Medicine
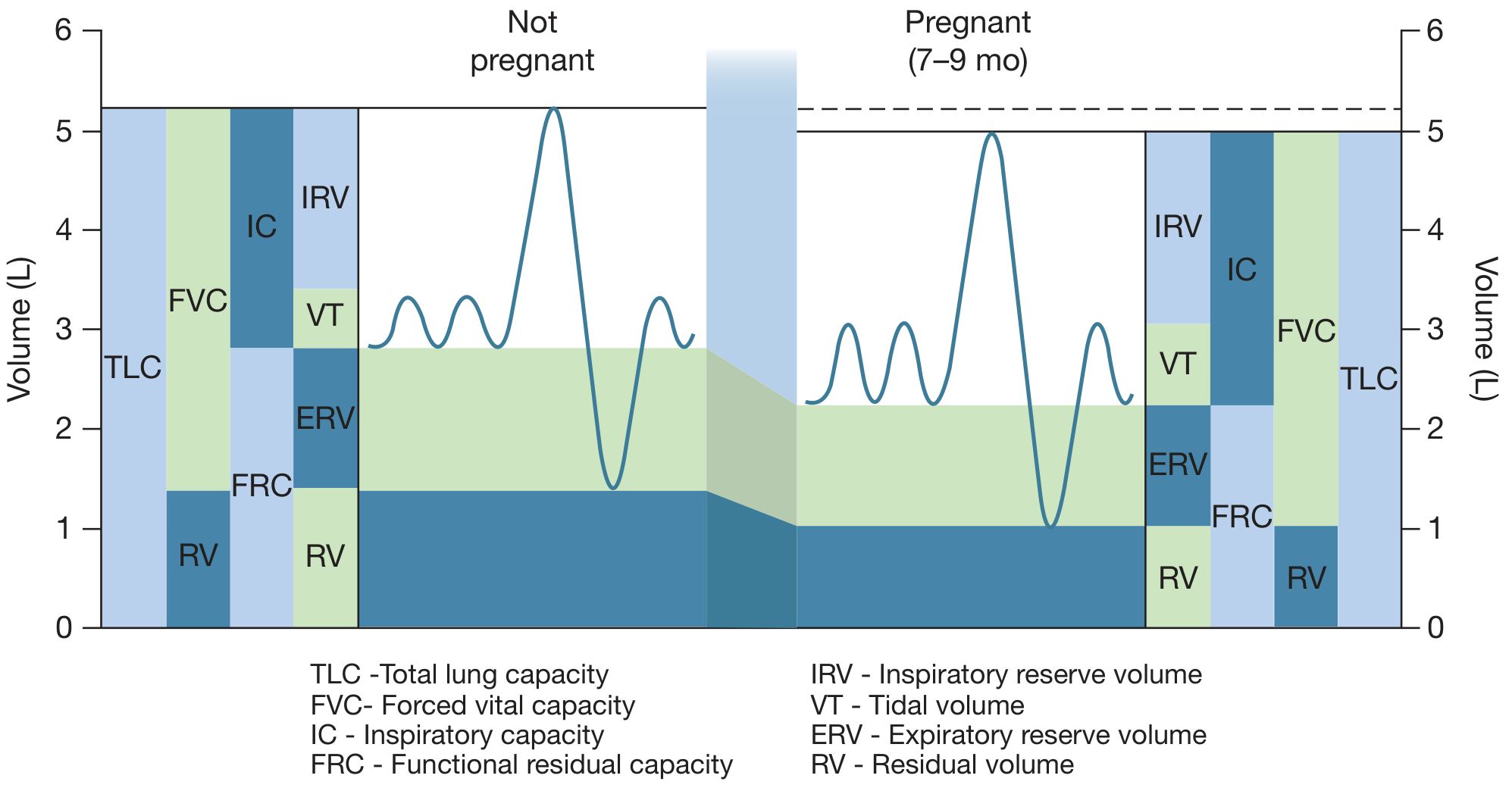
2. Lung Volume Changes
| Parameter | Direction | Magnitude |
|---|---|---|
| Tidal Volume (TV) | ↑ | ~40–50% (500 → 700 mL) |
| Inspiratory Reserve Volume (IRV) | ↑ | Slight increase |
| Expiratory Reserve Volume (ERV) | ↓ | ~20% decrease |
| Residual Volume (RV) | ↓ | ~20% (1200 → 1000 mL) |
| Functional Residual Capacity (FRC) | ↓ | 20–30% by late gestation |
| Inspiratory Capacity (IC) | ↑ | Increases |
| Vital Capacity (VC) | ↔ | No significant change |
| Total Lung Capacity (TLC) | ↔/↓ | 4–5% decrease (minimal) |
Key exam point: FRC = ERV + RV — both decrease → FRC decreases significantly. IC increases, which compensates, keeping TLC near normal. Vital capacity is preserved. FRC decreases further in the supine position.
The physiologic dead space increases by ~60 mL due to dilation of small airways, but the VD/VT ratio is unchanged (dead space increases proportionally with tidal volume).
— Creasy & Resnik's Maternal-Fetal Medicine; Fishman's Pulmonary Diseases and Disorders
3. Ventilation Changes
| Parameter | Direction | Magnitude |
|---|---|---|
| Respiratory Rate (RR) | ↔ | No change early; rises ~10% only late in pregnancy |
| Tidal Volume (TV) | ↑ | 40–50% |
| Minute Ventilation (MV) | ↑ | ~50% (7.5 → 10.5 L/min) |
| Alveolar Ventilation | ↑ | Significantly increased |
| Airway Resistance | ↓ | Decreases (bronchial smooth muscle relaxation) |
| Total Pulmonary Resistance | ↓ | Falls |
The 50% increase in minute ventilation is almost entirely due to the increase in tidal volume, not respiratory rate. This increase begins in the first trimester (as early as 6 weeks) and is maintained throughout.
Mechanism: Progesterone acts as a direct respiratory center stimulant. The CO₂ threshold of the respiratory center is lowered. In pregnancy, a 1 mmHg rise in PaCO₂ increases ventilation by 6 L/min (vs. 1.5 L/min in non-pregnant state) — a 4-fold increase in respiratory center sensitivity.
Progesterone also increases carbonic anhydrase B levels in RBCs, facilitating CO₂ transfer and independently lowering PaCO₂.
— Creasy & Resnik's Maternal-Fetal Medicine; Medical Physiology (Boron & Boulpaep)
4. Arterial Blood Gas Changes
| Parameter | Non-Pregnant | Pregnant | Change |
|---|---|---|---|
| PaO₂ | ~95 mmHg | 100–105 mmHg | ↑ |
| PaCO₂ | ~40 mmHg | 27–32 mmHg | ↓ |
| pH | 7.40 | 7.42–7.46 | ↑ (mild respiratory alkalosis) |
| HCO₃⁻ | 24 mEq/L | 18–22 mEq/L | ↓ (renal compensation) |
| Alveolar–arterial O₂ gradient | ~8–10 mmHg | ~20 mmHg (late gestation) | ↑ |
The "Compensated Respiratory Alkalosis of Pregnancy"
- Hyperventilation → ↓ PaCO₂ (physiologic hypocapnia)
- Compensatory renal response: Increased HCO₃⁻ excretion → plasma bicarbonate falls to 18–22 mEq/L
- Net result: pH normalizes to ~7.44 (mild alkalosis)
- Clinical importance: A PaCO₂ of 40 mmHg in the second half of pregnancy is NOT normal — it represents inadequate ventilation and potential respiratory acidosis that could cause fetal distress
The PaCO₂ is linearly and inversely related to the log of progesterone concentration.
PaCO₂ decreases even further at high altitudes as the mother exhibits compensatory hyperventilation to maintain PaO₂.
— Fishman's Pulmonary Diseases and Disorders; Rosen's Emergency Medicine
5. Oxygen Consumption and Delivery
| Parameter | Change |
|---|---|
| O₂ consumption | ↑ 20–33% above pre-pregnancy levels |
| O₂ consumption during labor | Increases further (up to 40–60% above pre-pregnancy) |
The increase in O₂ consumption reflects combined maternal and fetal metabolic demands. This drives the compensatory increase in minute ventilation.
Oxyhemoglobin dissociation curve: The chronic respiratory alkalosis causes a rightward shift of the oxyhemoglobin dissociation curve, facilitating O₂ transfer across the placenta to the fetus.
Diffusion capacity (DLco): Higher in the first trimester (increased cardiac output improves perfusion of lung apices), but declines later — reaching a nadir at 24–27 weeks — due to the dilutional anemia of pregnancy. Overall, DLco shows minimal net change.
6. Dyspnea of Pregnancy
- ~70% of pregnant women experience dyspnea, typically by the third trimester
- This is a physiologic dyspnea — the sensation of breathlessness despite improved oxygenation
- Likely reflects heightened awareness of the augmented ventilatory drive from progesterone
- Must be distinguished from pathologic causes (pulmonary embolism, asthma, peripartum cardiomyopathy)
7. Upper Airway Changes
- Nasal mucosa: Estrogen causes edema, hyperemia, and glandular hypersecretion → gestational rhinitis (last few weeks of pregnancy)
- Nasopharyngeal caliber: Reduced due to mucosal engorgement
- Clinical relevance: Epistaxis is more common; difficult nasotracheal intubation; snoring and obstructive sleep apnea may worsen
Despite reduced nasopharyngeal caliber, air flow rates and airway resistance do not worsen systemically because progesterone causes bronchial smooth muscle relaxation.
8. Changes During Labor and Delivery
- O₂ consumption and MV increase further with uterine contractions
- Hyperventilation during contractions can cause transient hypocapnia and maternal dizziness/tetany
- Pain relief reduces hyperventilation and normalizes gas exchange
- Supine position further reduces FRC → increased risk of atelectasis and V/Q mismatch
Summary Table (High-Yield for Exams)
| Parameter | Change | Magnitude |
|---|---|---|
| Tidal Volume | ↑ | 40–50% |
| Respiratory Rate | ↔ | Unchanged |
| Minute Ventilation | ↑ | ~50% |
| FRC | ↓ | 20–30% |
| RV | ↓ | ~20% |
| ERV | ↓ | ~20% |
| VC | ↔ | No change |
| TLC | ↔/↓ | 4–5% ↓ |
| PaO₂ | ↑ | 100–105 mmHg |
| PaCO₂ | ↓ | 27–32 mmHg |
| HCO₃⁻ | ↓ | 18–22 mEq/L |
| pH | ↑ | 7.42–7.46 (mild alk) |
| O₂ consumption | ↑ | 20–33% |
| Airway resistance | ↓ | Due to bronchodilation |
| Diaphragm | ↑ (cranial) | 4–5 cm |
Mechanisms — Exam Summary
- Progesterone → Respiratory center stimulation → ↑ TV → ↑ MV → ↓ PaCO₂ → Compensated respiratory alkalosis
- Progesterone → Bronchial smooth muscle relaxation → ↓ Airway resistance
- Progesterone → Diaphragm displacement + ↑ carbonic anhydrase B → further ↓ PaCO₂
- Enlarging uterus → Diaphragm elevates 4–5 cm → ↓ FRC, ↓ ERV, ↓ RV
- Estrogen → Nasal mucosal edema → Gestational rhinitis
- Hyperventilation + ↑ PaO₂ → Facilitates O₂ transfer to fetus
- Respiratory alkalosis → Rightward shift of oxyhemoglobin curve → Further facilitates placental O₂ transfer
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Fishman's Pulmonary Diseases and Disorders (2-Volume Set); Medical Physiology (Boron & Boulpaep); Rosen's Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.