Changes in aging of respiratory system full details for md exams 15marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive MD exam answer. Let me compile it.
Changes in the Aging Respiratory System
Sources: Fishman's Pulmonary Diseases and Disorders; Morgan & Mikhail's Clinical Anesthesiology
Introduction
The fastest-growing population segment is those aged ≥65 years. Even in apparently healthy elderly individuals, measurable decrements in respiratory function occur progressively, becoming most marked beyond age 60. These changes are:
- Intrinsic (not purely environmentally mediated)
- Universal
- Progressive
- Generally detrimental
Critically, while routine activities of healthy elderly persons are not limited by these changes, the physiologic reserve — especially for alveolar gas exchange — is substantially reduced, rendering the elderly vulnerable to stresses, diseases, and injuries that younger individuals weather easily.
I. Changes in the Upper Airway
- Cough reflex: Diminished with age due to reduced cortical and subcortical modulation (not just brainstem). This is the single most important defense mechanism against aspiration and its impairment drives the greatly increased risk of aspiration in the elderly.
- Swallowing reflex: Impaired — oropharyngeal dysphagia becomes more common due to muscle weakness and reduced sensory feedback.
- Mucociliary clearance: Impaired, increasing susceptibility to respiratory infections.
- Pharyngeal muscle tone: Reduced, contributing to upper airway collapse and obstructive sleep apnea.
II. Changes in Chest Wall Mechanics
- Chest wall compliance decreases: Progressive calcification of costal cartilages and stiffening of rib articulations make the chest wall less compliant (stiffer). This increases the work of breathing.
- Respiratory muscle strength decreases: Both inspiratory and expiratory muscle mass and function decline. Maximum inspiratory and expiratory pressures are measurably reduced. This limits the ability to generate peak flows during coughing.
- Postural changes: Dorsal kyphosis (due to vertebral collapse/osteoporosis) alters the geometry of the thorax and reduces the efficiency of respiratory muscle mechanics.
- Net effect: The chest wall contributes to an outward recoil of the respiratory system at lower lung volumes, partially offsetting the inward recoil lost from reduced lung elasticity (see below). The combined result is an increase in FRC.
III. Changes in Lung Parenchyma and Elastic Recoil
This is the most fundamental change:
- Decreased lung elastic recoil: Loss of elastin and cross-linking changes in collagen result in the lung becoming more compliant (floppy). This is a near-universal aging change and underlies many downstream alterations.
- Senile emphysema ("ductectasia"): Alveolar ducts enlarge and alveolar walls thin — without inflammatory destruction (distinguishing it from pathologic emphysema). The alveolar surface area decreases.
- Alveolar surface area reduction: From approximately 75 m² in youth to ~60 m² in old age, reducing the diffusing surface.
- Connective tissue remodeling: Altered proteoglycan and elastin composition of the extracellular matrix; reduced matrix metalloproteinase-mediated remodeling capacity.
IV. Lung Volumes — The Most Consistent Changes
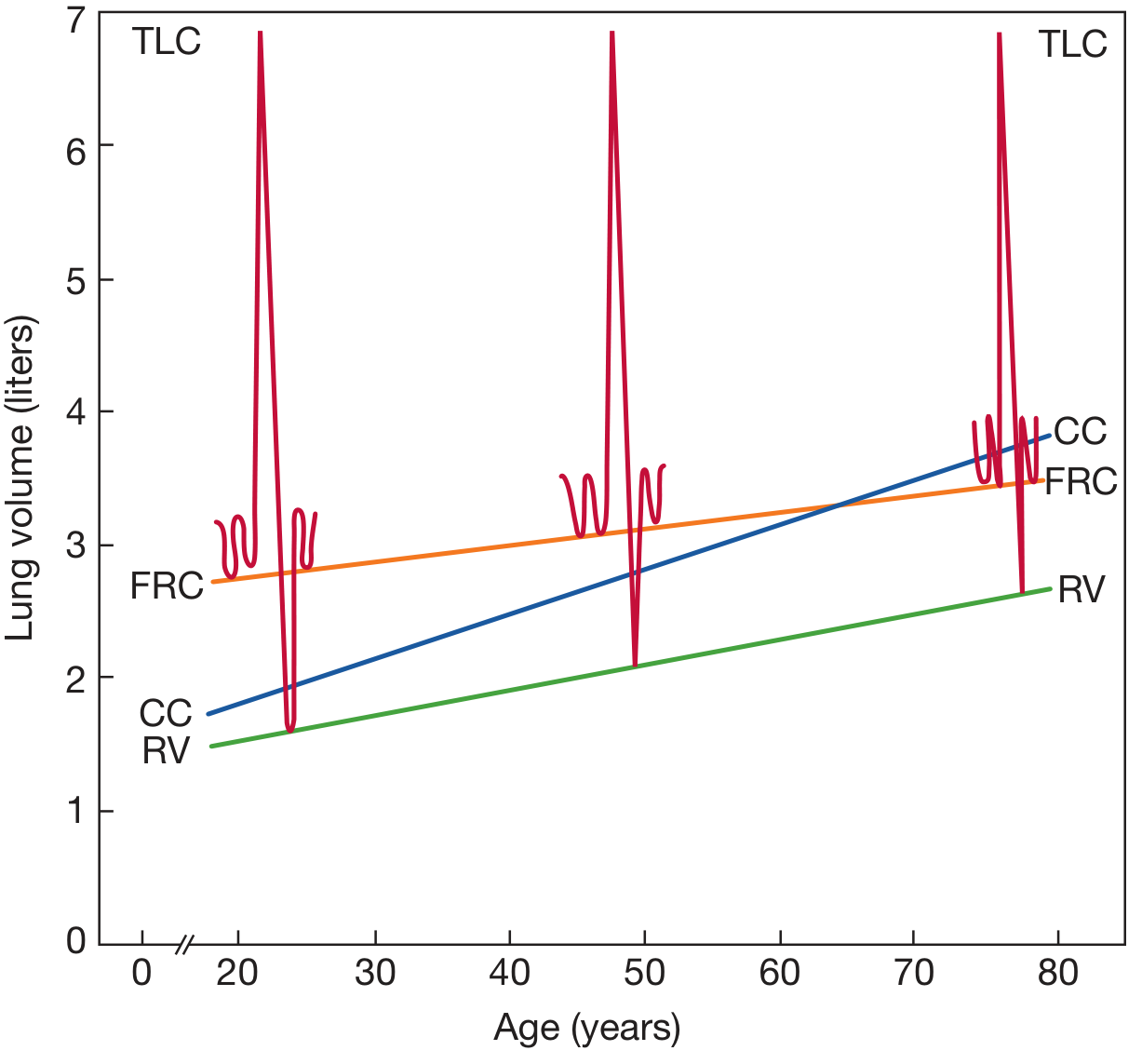
Schematic of lung volume changes with age (cross-sectional studies, seated individuals). RV and CC rise progressively; FRC rises; TLC remains relatively stable; VC falls. — Fishman's Pulmonary Diseases and Disorders
| Volume | Change with Aging | Mechanism |
|---|---|---|
| TLC | Unchanged or ↓ slightly (~8–19 mL/yr) | Opposing forces: ↑ lung compliance vs. ↓ respiratory muscle strength/stiffer chest wall roughly cancel out |
| VC (FVC) | ↓ 21–33 mL/yr (men); 18–29 mL/yr (women) | ↑ RV is the dominant cause |
| RV | ↑ markedly (~13–25 mL/yr) | Small airway collapse during expiration traps air |
| FRC | ↑ | ↓ lung elastic recoil shifts equilibrium point outward |
| CC (Closing Capacity) | ↑ significantly | Early airway closure at higher lung volumes |
Key Closing Capacity Concept (Exam Favourite)
- Closing capacity (CC) rises faster than FRC with age.
- At age 45 years (supine) and 65 years (upright), CC exceeds FRC.
- When CC > FRC, some airways close during normal tidal breathing, causing ventilation-perfusion (V/Q) mismatch and contributing to age-related fall in PaO₂.
V. Airflow and Spirometry
- FEV₁: Declines approximately 30 mL/year after age 30 in non-smokers. This is the most reproducible age-related change.
- FEV₁/FVC ratio: Falls progressively, reflecting disproportionately greater loss of flow rates vs. volumes.
- Peak expiratory flow (PEF): Decreases due to reduced muscle strength and reduced elastic recoil driving expiratory flow.
- Flow-volume loops: Show characteristic reduction in expiratory flow at low lung volumes, indicative of small airway collapse and loss of recoil.
- Pattern: Overall pattern resembles mild obstruction, but due to aging per se (not disease).
VI. Gas Exchange
Diffusing Capacity (DLCO)
- DLCO falls approximately 0.2 mL/min/mmHg/year after age 40.
- Due to: ↓ alveolar surface area, ↓ alveolar capillary surface area, ↓ pulmonary capillary blood volume.
Arterial Blood Gases
- PaO₂ (arterial oxygen tension) falls progressively with age. Estimated by: PaO₂ = 100 − 0.33 × age (in mmHg), or approximately 75–80 mmHg at age 70 in a healthy nonsmoker.
- The primary mechanism is increased V/Q mismatch from CC exceeding FRC and early airway closure, not alveolar hypoventilation.
- PaCO₂: Remains normal (aging does not impair CO₂ elimination under resting conditions).
- A-a gradient: Widens with age (normal value increases approximately with age).
- pH: Normal.
Ventilation-Perfusion (V/Q) Mismatch
- Increased physiologic shunt fraction due to early airway closure.
- Increased physiologic dead space — both anatomic and alveolar.
VII. Control of Ventilation
These changes are often underappreciated but clinically critical:
- Hypoxic ventilatory response (HVR): Reduced by up to 50% in elderly men.
- Hypercapnic ventilatory response (HCVR): Reduced by up to 40%.
- These reductions in chemosensitivity mean the elderly fail to mount an appropriate ventilatory response to hypoxia or hypercapnia, making them vulnerable to:
- Silent hypoxemia during sleep
- Respiratory failure during acute illness
- Opioid- or sedative-induced apnea
- The mechanism involves reduced central chemoreceptor sensitivity and, possibly, reduced peripheral chemoreceptor (carotid body) function.
VIII. Defense Mechanisms and Immunity
- Mucociliary clearance: Reduced cilia beat frequency and altered mucus viscoelasticity impair particle clearance from airways.
- Cough effectiveness: Reduced due to weaker expiratory muscles and impaired glottic function.
- Alveolar macrophage function: Phagocytic activity and cytokine responsiveness are impaired.
- Immunosenescence: Both innate and adaptive immune responses decline, increasing susceptibility to pneumonia (especially pneumococcal), influenza, and reactivation tuberculosis.
- "Inflamm-aging": Low-grade chronic systemic inflammation (elevated IL-6, TNF-α, CRP) paradoxically accompanies this immune decline, contributing to parenchymal remodeling.
IX. Pulmonary Vasculature
- Pulmonary vascular resistance (PVR) increases modestly with age due to intimal thickening and increased wall stiffness of pulmonary vessels.
- Pulmonary artery pressure rises slightly at rest and more markedly with exercise.
- Pulmonary capillary blood volume is reduced, contributing to the fall in DLCO.
X. Exercise Capacity and Breathing Reserve
- VO₂ max decreases approximately 1% per year after age 30, in part due to respiratory limitations.
- Maximal ventilation (MVV) decreases substantially — reduced respiratory muscle strength and increased airway resistance both contribute.
- Breathing reserve (MVV − peak exercise VE) is reduced but usually still adequate for normal activities; the primary limitation to exercise in the elderly is cardiovascular.
- Work of breathing increases due to stiffer chest wall, reduced lung recoil (less stored energy to drive expiration), and increased airway resistance.
XI. Biology of Lung Aging — Molecular Mechanisms
Per the NIH "pillars of aging" framework applied to the lung:
| Pillar | Relevance to Lung Aging |
|---|---|
| Inflammation | Chronic low-grade "inflamm-aging"; altered macrophage/neutrophil function |
| Adaptation to stress | Reduced heat-shock protein response; impaired autophagy |
| Epigenetics | DNA methylation changes alter gene expression in alveolar cells |
| Cellular metabolism | Mitochondrial dysfunction in type II pneumocytes |
| Macromolecular damage | Accumulated oxidative DNA/protein damage; telomere shortening |
| Proteostasis | Impaired protein folding/clearance (relevant to fibrosis pathogenesis) |
| Stem cells/Regeneration | Reduced alveolar epithelial progenitor pool; impaired repair after injury |
These molecular changes link normal aging to accelerated-aging diseases like COPD and idiopathic pulmonary fibrosis (IPF).
XII. Clinical Implications
| Clinical Scenario | Effect of Aging |
|---|---|
| Perioperative | Prolonged preoxygenation needed; higher FiO₂ intraoperatively; PEEP beneficial; more postoperative pulmonary complications |
| Drug sensitivity | Reduced ventilatory response → greater risk of opioid/sedative-induced apnea |
| Infection | Increased risk of pneumonia, impaired recovery, higher mortality |
| Interpreting PFTs | Reference ranges less reliable >age 80; use LLN not fixed 70% cutoff for FEV₁/FVC |
| Aspiration | Markedly increased risk due to impaired swallowing and cough reflexes |
| SARS-CoV-2/COVID-19 | Age is the dominant risk factor for severe disease, critically ill admission, and mortality |
Summary Table — Key Changes at a Glance
| Parameter | Direction | Magnitude/Notes |
|---|---|---|
| Lung elastic recoil | ↓ | Most fundamental change |
| Chest wall compliance | ↓ | Calcification, kyphosis |
| FRC | ↑ | Balance point shifts outward |
| RV | ↑ ↑ | Most consistent change |
| TLC | ↔ or ↓ slightly | Opposing forces balance |
| VC / FVC | ↓ | ~20–30 mL/yr |
| FEV₁ | ↓ | ~30 mL/yr |
| FEV₁/FVC | ↓ | |
| DLCO | ↓ | ~0.2 mL/min/mmHg/yr |
| PaO₂ | ↓ | ~75–80 mmHg at age 70 |
| PaCO₂ | ↔ | |
| A-a gradient | ↑ | |
| HVR / HCVR | ↓ ↓ | 40–50% reduction |
| Respiratory muscle strength | ↓ | |
| Mucociliary clearance | ↓ | |
| Cough reflex | ↓ | Aspiration risk ↑ |
— Fishman's Pulmonary Diseases and Disorders, 6e (Chapter 18: Aging of the Respiratory System); Morgan & Mikhail's Clinical Anesthesiology, 7e (Chapter 43)
This is a shared conversation. Sign in to Orris to start your own chat.