Tympanosclerosis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching Images
tympanosclerosis ear drum tympanic membrane
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive data. Let me compile the complete 50-mark answer on Tympanosclerosis.
TYMPANOSCLEROSIS — 50 MARKS (RGUHS)
1. DEFINITION
Tympanosclerosis is a pathological condition of the middle ear and tympanic membrane characterised by the deposition of acellular hyaline and calcified plaques within the lamina propria of the tympanic membrane (TM) and in the submucosa of the middle ear cleft, occurring as a sequela of chronic inflammation, infection, or trauma.
- When limited to the tympanic membrane → Myringosclerosis
- When involving the middle ear mucosa and ossicles → Tympanosclerosis (proper)
"Tympanosclerosis is thought to be a complication of otitis media in which acellular hyaline and calcified deposits accumulate within the tympanic membrane and the submucosa of the middle ear." — Cummings Otolaryngology, 7th Ed.
2. HISTORICAL BACKGROUND
- The term "tympanosclerosis" was introduced by von Troltsch (1873), who described chalky-white deposits on the tympanic membrane.
- Zöllner and Birken (1956) described the clinical and surgical significance of middle ear involvement.
- Detailed histopathological description was provided by Hussl and Lim (1984) — "Recent Advances in Otitis Media with Effusion" — who elaborated on the two-pathway mechanism of plaque formation.
- Kinney (1978) reported 20% incidence in patients undergoing surgery for chronic otitis media.
3. INCIDENCE AND EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence post-tympanostomy tubes | 59% (Tos & Stangerup) vs 13% in myringotomy-only ears |
| Incidence post-ventilating tubes (6–8 yrs follow-up) | 19.7% (Hussl & Mueller) |
| Children aged 4–15 years (weighted average) | 10% (Daly) |
| Chronic otitis media patients | 9–38% |
| Surgical CSOM patients | 20–23.6% (Kinney; Mangat et al.) |
(Cummings Otolaryngology, Chapter 140)
4. AETIOLOGY AND PREDISPOSING FACTORS
Primary Causes:
- Chronic otitis media (CSOM) — most common
- Recurrent acute otitis media (AOM)
- Otitis media with effusion (OME) + grommet insertion
- Eustachian tube dysfunction — deformation alone (without infection) shown to cause tympanosclerosis in rats (Wielinga et al.)
- Trauma — iatrogenic (myringotomy, paracentesis), temporal bone fracture
Microbial Associations:
- H. pylori identified in tympanosclerotic ears (Saki et al.)
- Chlamydia pneumoniae identified as a possible etiology (Dinc et al.)
Genetic Factors:
- LP/J mouse and Enpp1^asj mutant mice — two animal models showing spontaneous tympanosclerosis, suggesting a genetic predisposition
- Mutations in the ENPP1 gene (encoding ectonucleotide pyrophosphatase/phosphodiesterase 1) implicated in aberrant calcification pathways
5. PATHOGENESIS — DUAL PATHWAY (Hussl & Lim, 1984)
The fundamental process is connective tissue degeneration triggered by pathogenic factors (inflammation, autoimmunity, trauma), leading to calcified plaque formation via two parallel mechanisms:
PATHOGENESIS FLOWCHART (from Cummings — Fig. 140.19):
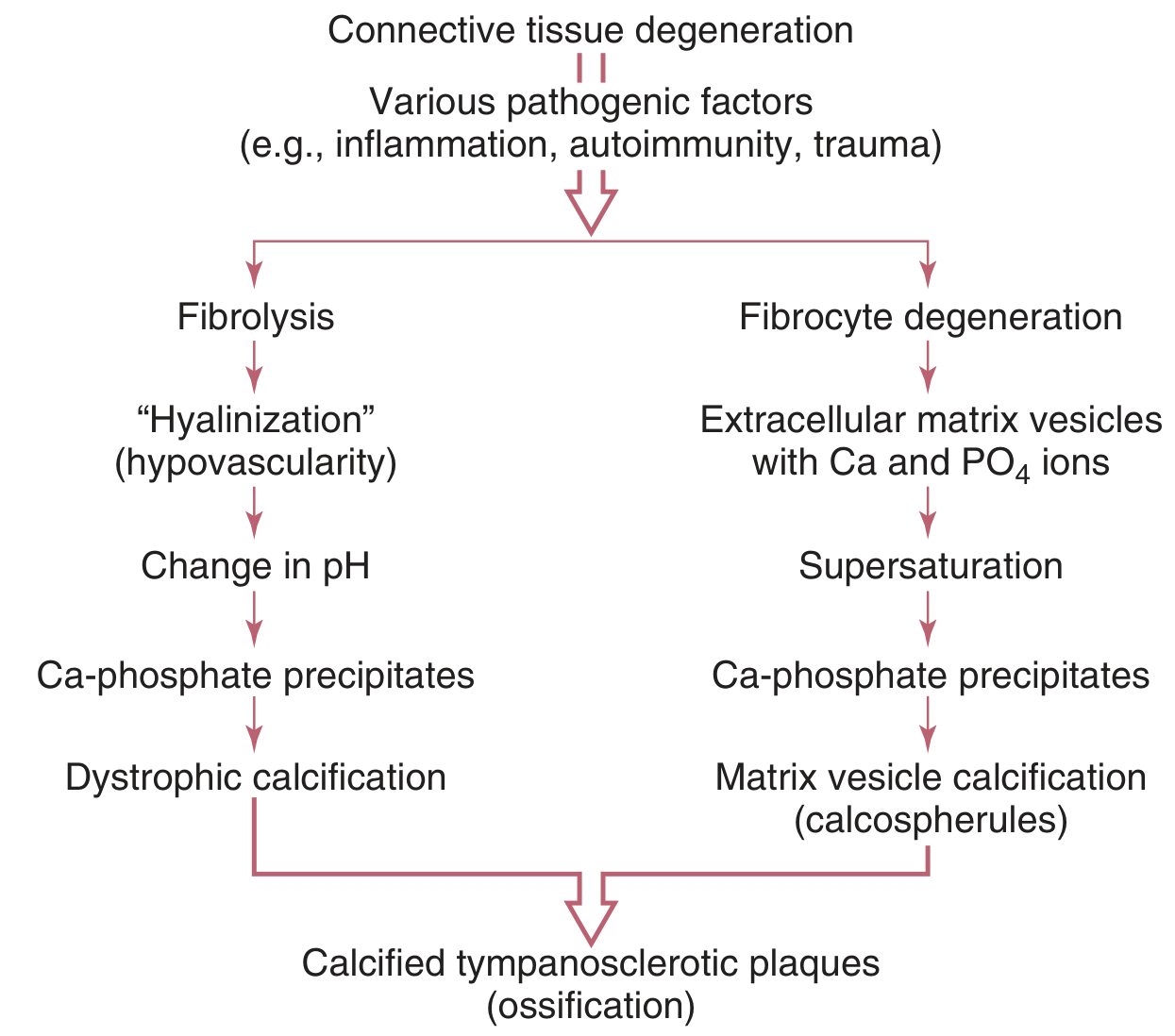
Pathway 1 — Fibrolysis/Dystrophic Calcification:
Connective tissue degeneration
↓
Fibrolysis (enzymatic degradation by bacterial proteinases & collagenases)
↓
"Hyalinization" (hypovascularity)
↓
Change in local pH
↓
Ca-phosphate precipitates
↓
Dystrophic calcification
↓
Calcified tympanosclerotic plaques (ossification)
Pathway 2 — Matrix Vesicle Calcification:
Connective tissue degeneration
↓
Fibrocyte degeneration
↓
Extracellular matrix vesicles released (containing Ca²⁺ and PO₄³⁻ ions)
↓
Supersaturation of ions
↓
Ca-phosphate precipitates
↓
Matrix vesicle calcification → Calcospherules
↓
Calcified tympanosclerotic plaques (ossification)
Both pathways converge to: Calcified tympanosclerotic plaques → Osteoneogenesis → Ossicular fixation
6. PATHOLOGY
Gross Pathology:
- Chalky white, avascular, hard plaques
- Semicircular or horseshoe-shaped deposits within TM (pars tensa)
- In middle ear: deposits around promontory, malleus head, incus body, stapedial footplate
- Plaques attached to ossicles — "onion ring" layered pattern
Histopathology:
- Acellular hyalinisation of subepithelial connective tissue (lamina propria)
- Loss of normal collagen architecture — replaced by homogeneous eosinophilic matrix
- Dystrophic calcification — calcium hydroxyapatite deposits
- Calcospherules — concentric rings of calcified matrix vesicles
- Osteoneogenesis — new bone formation in severe cases (microscopically resembles woven/lamellar bone)
- Plaques limited to lamina propria of pars tensa in myringosclerosis
- Overlying epithelium is intact and normal
- No inflammatory cells in established plaques (acellular)
"Microscopically, collagen and fibrous tissue with hyaline degeneration is present within the lamina propria of the pars tensa and the middle ear mucosa. The deposition of hyaline occurs in layers similar to the rings of an onion and may reach a thickness of a few millimetres." — Cummings Otolaryngology
7. CLASSIFICATION
By Site (Tos Classification — Clinical Relevance):
| Type | Site | Hearing Effect |
|---|---|---|
| Type I (Myringosclerosis) | TM only (lamina propria) | Minimal/nil |
| Type II | Middle ear mucosa (promontory, round window niche) | Variable |
| Type III | Ossicular involvement — malleus/incus fixation | Moderate conductive HL |
| Type IV | Stapes footplate fixation | Severe conductive HL |
| Type V (Pansclerosis) | Diffuse TM + middle ear + ossicular fixation | Maximal conductive HL |
By Extent (Surgical Classification):
- Localised — single plaque, TM only
- Diffuse — multiple plaques, entire TM
- Extensive — TM + ossicular chain + oval window
8. CLINICAL FEATURES
Symptoms:
- Hearing loss — conductive type; degree depends on ossicular involvement
- Hearing may be normal in pure myringosclerosis (TM plaques only)
- History of recurrent otitis media, grommet insertion, or ear surgery
- Tinnitus — occasionally
- No pain, no discharge (unless coexistent CSOM)
Signs — Otoscopic Findings:
- Chalky white semicircular/horseshoe-shaped plaques in pars tensa of TM
- Plaques may be bilateral
- TM may appear thickened, opaque, immobile
- In CSOM with tympanosclerosis: perforation + white plaques on remnant TM
Otoscopic Image — Tympanosclerosis (Myringosclerosis):

Dense, chalky white, semi-circular plaque in the pars tensa — classic myringosclerosis pattern
Multi-modal Diagnostic Image (CT + 3D + Otoscopy):
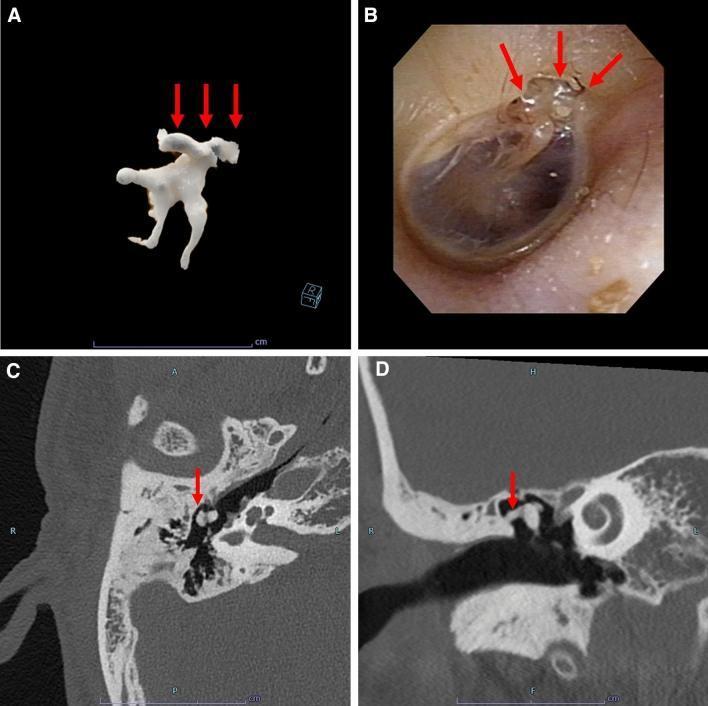
(A) 3D reconstruction showing calcified ossicular deposits (red arrows); (B) Otoscopy — white chalky plaques; (C & D) CT temporal bone (axial & coronal) — hyperattenuating calcifications around malleus and incus
9. DIAGNOSIS
Clinical Diagnosis Flow:
History (recurrent AOM / OME / grommet / CSOM)
↓
Otoscopy → Chalky white TM plaques
↓
Pneumatic otoscopy → Reduced/absent TM mobility
↓
Tuning fork tests → CHL (BC normal, AC reduced)
Rinne negative, Weber lateralises to affected ear
↓
Pure Tone Audiogram → CHL (air-bone gap)
↓
Tympanometry → Type As (stiff) or Type B (if effusion)
↓
HRCT Temporal Bone → Confirm ossicular fixation, extent
↓
Intraoperative findings → Definitive
Investigations:
| Test | Finding in Tympanosclerosis |
|---|---|
| Pure Tone Audiogram (PTA) | Conductive HL; air-bone gap 20–60 dB |
| Tympanometry | Type As (reduced compliance) or flat Type B |
| Acoustic reflexes | Absent |
| HRCT Temporal Bone | Hyperdense calcified plaques; ossicular fixation; oval window involvement |
| Stapes reflex | Absent in ossicular fixation |
"Ossicular fixation from tympanosclerosis should be suspected as the cause of conductive hearing loss when a history of chronic infections is present or when tympanosclerosis is seen on the TM." — Cummings Otolaryngology
Differential Diagnosis:
| Condition | Distinguishing Feature |
|---|---|
| Otosclerosis | Normal TM; stapedial fixation; positive family history; Carhart's notch at 2 kHz; no history of OM |
| Adhesive otitis media | TM retracted, adherent to promontory; no white plaques |
| Cholesteatoma | Pearly white mass; marginal perforation; offensive discharge; bone erosion on CT |
| Middle ear osteoma | Rare; bony mass; CT distinguishes |
10. MANAGEMENT
FLOWCHART — Management of Tympanosclerosis:
Tympanosclerosis
↓
ASSESS
┌────────────┬────────────────────┐
↓ ↓ ↓
TM only Middle ear/ Diffuse +
(Myring- Ossicular Bilateral
osclerosis) involvement
↓ ↓ ↓
Hearing Conductive HL Consider
normal? (air-bone gap) BAHA/HAs
↓
YES → Observe
↓
NO (large plaque
affecting TM) → Surgical removal
during tympanoplasty
↓
SURGERY
┌───────────────────────────────────┐
↓ ↓
TM + Ossicular Stapes fixation
fixation (malleus,
incus)
↓ ↓
Stage I: Stapedectomy /
Myringoplasty + Stapedotomy
Ossiculoplasty (higher cochlear
(TORP/PORP) damage risk!)
↓
Stage II (if needed):
Ossicular reconstruction
A. Conservative Management:
- Observation — for myringosclerosis without hearing loss
- Hearing aids — for elderly, poor surgical candidates, bilateral disease
- BAHA (Bone-Anchored Hearing Aid) — particularly beneficial in tympanosclerosis with ossicular fixation, canal atresia; noted as specifically beneficial in Cummings (Ch. 136)
B. Surgical Management:
Principles (Tos, 1983 — Cummings Chapter 140):
"Whenever possible, an intact ossicular chain is preserved. When the disease is restricted to the TM remnant, smaller areas of myringosclerosis have no effect on hearing and can be left alone; however, tympanosclerosis that affects a large area should be removed and replaced with the graft."
Surgical Options:
| Procedure | Indication |
|---|---|
| Myringoplasty/Tympanoplasty | TM repair; removal of large TM plaques |
| Ossiculoplasty (TORP/PORP) | Malleus-incus fixation; ossicular chain reconstruction |
| Stapedectomy/Stapedotomy | Stapes footplate fixation by tympanosclerosis |
| Mastoidectomy | Coexistent CSOM/mastoid disease |
| Combined approach tympanoplasty | Extensive disease with mastoid involvement |
Surgical Challenges:
- High risk of sensorineural hearing loss (SNHL) — due to extensive dissection required; cochlear damage from manipulation around oval window
- Smyth et al. — 79% excellent results with 2-stage ossicular reconstruction (stapedectomy + TORP)
- Gormley — only 7% had air-bone gap <21 dB on long-term follow-up after stapedectomy
- One-stage procedures — 21% cochlear loss in older series (Cummings)
Risk of Recurrence:
- Tympanosclerosis can recur after surgical removal — ongoing inflammation perpetuates the cycle
- Staging procedures help reduce operative trauma and cochlear risk
11. PROGNOSIS
| Type | Prognosis |
|---|---|
| Myringosclerosis only | Excellent — hearing unaffected |
| Isolated ossicular fixation (malleus/incus) | Good — with ossiculoplasty |
| Stapes footplate fixation | Guarded — high cochlear risk |
| Pansclerosis (TM + ossicles + round window) | Poor — limited surgical options; BAHA preferred |
| Post-operative SNHL | Irreversible |
12. RECENT ADVANCES
1. Molecular / Genetic Mechanisms:
- ENPP1 gene mutations (ectonucleotide pyrophosphatase/phosphodiesterase 1) — identified in Enpp1^asj mice model; ENPP1 regulates inorganic pyrophosphate (PPi) levels, a potent inhibitor of calcification; its dysfunction → excess calcium-phosphate deposition
- Free radical / oxidative stress hypothesis — reactive oxygen species (ROS) from chronic inflammation damage middle ear connective tissue, initiating the hyalinisation-calcification cascade
- Matrix metalloproteinase (MMP) dysregulation — MMPs (collagenases) play a role in aberrant collagen remodelling leading to plaque formation
2. Role of Biofilm:
- Bacterial biofilms (P. aeruginosa, H. influenzae, S. pneumoniae) persist in chronic otitis media; the biofilm microenvironment may potentiate tympanosclerotic changes by chronically stimulating inflammation
- Antibiotic-tolerant "persister cells" within biofilms maintain the chronic inflammatory stimulus
3. Imaging Advances:
- High-resolution CT (HRCT) of the temporal bone — now the gold standard preoperative investigation; delineates exact ossicular fixation, oval/round window involvement
- Cone-beam CT (CBCT) — lower radiation; comparable resolution; emerging role in pre-surgical planning
- 3D reconstruction imaging of ossicular chain — shows calcified deposits and their spatial relationship to critical structures
4. Surgical Advances:
- Endoscopic ear surgery (EES) — transcanal endoscopic approach allows superior visualisation of anterior epitympanum, oval window, and round window niche; improved access for removal of tympanosclerotic plaques with minimal trauma
- Laser-assisted surgery (CO₂, KTP, Er:YAG lasers) — precise removal of calcified plaques around stapes footplate, reducing mechanical trauma and SNHL risk
- Total ossicular replacement prostheses (TORP/PORP) made of hydroxyapatite or titanium — improved biocompatibility and long-term results
- Bone-anchored hearing aids (BAHA/Bonebridge) — increasingly preferred over high-risk ossicular surgery in pansclerosis
5. Free Radical Theory (Reactive Oxygen Species):
- Recent evidence implicates oxidative damage to middle ear mucosa — superoxide dismutase and catalase levels are reduced in tympanosclerotic ears
- N-acetylcysteine (NAC) and antioxidant therapy are experimental strategies to prevent recurrence post-surgery
6. Prevention:
- Proper management of AOM and OME reduces incidence
- Careful technique during ventilating tube insertion and myringotomy — reduces post-procedural tympanosclerosis
- Avoiding prolonged tube retention — long-dwell tubes associated with higher myringosclerosis rates
13. SUMMARY TABLE
| Feature | Detail |
|---|---|
| Definition | Acellular hyaline/calcified deposits in TM and middle ear submucosa |
| Cause | Sequela of chronic OM, recurrent AOM, OME, grommet insertion, trauma |
| Histology | Hyalinisation of lamina propria → dystrophic calcification → osteoneogenesis |
| TM finding | Chalky white horseshoe/crescent plaques in pars tensa |
| Key symptom | Conductive hearing loss (if ossicular involvement) |
| Audiogram | Conductive HL; air-bone gap; absent stapedial reflex |
| Tympanogram | Type As or Type B |
| Gold standard imaging | HRCT temporal bone |
| Treatment of choice | Surgical: tympanoplasty ± ossiculoplasty; BAHA for pansclerosis |
| Most feared complication | Sensorineural hearing loss (cochlear damage intraoperatively) |
| Recurrence | Possible after surgical removal |
REFERENCES (Standard Textbooks)
- Cummings Otolaryngology: Head and Neck Surgery, 7th Edition — Flint PW et al. Chapter 140 (Chronic Otitis Media): Tympanosclerosis — Diagnosis, Pathogenesis, Management; Ossicular Fixation — pp. 2693–2695, 2734.
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery — Gleeson M et al. Section on Tympanosclerosis and sequelae of chronic otitis media.
- Stell and Maran's Head and Neck Surgery — Section on middle ear pathology and sequelae.
- Diseases of Ear, Nose and Throat — P.L. Dhingra, 7th Edition — Chapter on Chronic Suppurative Otitis Media and Tympanosclerosis.
- Hazarika's Textbook of Ear, Nose and Throat — Chapter on CSOM complications and tympanosclerosis.
- K.J. Lee's Essential Otolaryngology — Tympanosclerosis in middle ear disease.
- Hussl B, Lim DJ — Histopathology of tympanosclerosis. In: Lim DJ (ed). Recent Advances in Otitis Media with Effusion, Mosby, 1984.
- Tos M — Surgical treatment of tympanosclerosis. ORL J Otorhinolaryngol Relat Spec, 1983.
- Smyth GD et al. — Ossicular reconstruction in tympanosclerosis. Results of two-stage procedures.
- Wielinga EWJ et al. — Eustachian tube obstruction and tympanosclerosis in rats. Acta Otolaryngol, 1993.
RGUHS Exam Tip: For a 50-mark answer, structure under: Definition → Aetiology → Pathogenesis (with dual-pathway flowchart) → Pathology → Classification → Clinical features → Investigations → Management (flowchart) → Recent advances → Prognosis. The pathogenesis flowchart (Hussl & Lim, from Cummings Fig. 140.19) and the management algorithm are high-yield marks. Emphasise the distinction between myringosclerosis (TM-only, no hearing loss) and true tympanosclerosis (middle ear + ossicular fixation → conductive HL), and the risk of SNHL with stapes surgery in tympanosclerosis.
This is a shared conversation. Sign in to Orris to start your own chat.