mpfl reconstruction
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of MPFL reconstruction based on Miller's Review of Orthopaedics, 9th Edition:
MPFL Reconstruction
Anatomy
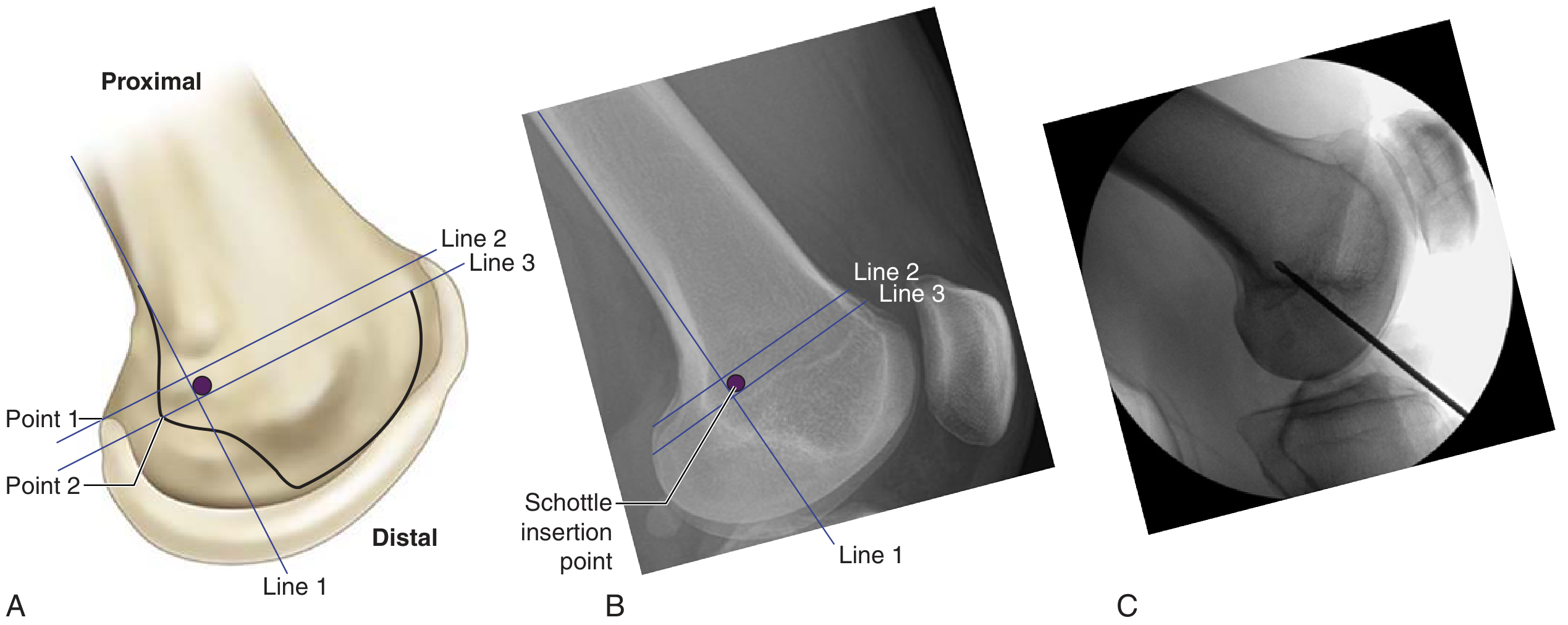
The medial patellofemoral ligament (MPFL) runs from the proximal third of the medial patella to the Schottle point on the femur — located between the adductor tubercle and the medial epicondyle. Radiographically, this point is:
- 1 mm anterior to the posterior cortex extension line
- 2.5 mm distal to the posterior origin of the medial femoral condyle
- Proximal to the most posterior point of the Blumensaat line
The MPFL is the primary passive restraint against lateral patellar translation, especially in early flexion (0–30°).
Indications
MPFL reconstruction is the cornerstone of proximal realignment for recurrent patellar instability. It is indicated when:
- Recurrent lateral patellar dislocation/subluxation is present
- The TT-TG distance is < 20 mm (if ≥ 20 mm, distal realignment with tibial tubercle osteotomy is added)
- Trochlear dysplasia or patella alta may be concurrent factors
Surgical Technique
Graft choice: Gracilis or semitendinosus tendon (autograft or allograft)
Key steps:
- Patellar attachment — graft woven or sutured into the proximal/medial patella
- Femoral attachment — anchored at the Schottle point (confirmed with intraoperative fluoroscopy — see image below)
- Graft tensioned with the knee at ~30° of flexion; must allow full flexion without overtightening
Femoral Tunnel Position: Critical Pitfalls
| Tunnel position | Effect |
|---|---|
| Too proximal | Graft tight in flexion |
| Too distal | Graft loose in flexion |
Accurate placement at the Schottle point is essential for an isometric graft.
Procedures That Have Fallen Out of Favor
- VMO advancement (Green procedure)
- Medial retinacular plication alone
- Isolated lateral release — should NOT be performed for patellar instability
Combined Distal Realignment (When Needed)
Tibial tubercle anteromedialization (Fulkerson osteotomy) is added when:
- TT-TG distance > 20 mm
- Increased Q angle
Contraindication: proximal arthrosis of the medial patellar facet.
Complications
- Medial patellar instability — from overtightening the MPFL graft
- Medial patellar osteoarthritis — also from excessive graft tension
- Recurrent lateral instability — from malpositioned femoral tunnel
Patellar Instability Risk Factors (Context)
Higher recurrence risk with: younger age, female sex, patella alta, and trochlear dysplasia. Recurrence after first-time dislocation ranges from 15–60%.
— Miller's Review of Orthopaedics, 9th Edition, pp. 365–366
give for 20 marks exam essay post graduate
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Now I have comprehensive material. Let me compose the full postgraduate essay.
MPFL Reconstruction — Postgraduate Essay (20 Marks)
Introduction
The medial patellofemoral ligament (MPFL) is the primary passive restraint against lateral patellar displacement, contributing approximately 50–60% of the total medial restraining force, particularly in the critical range of 0–30° of knee flexion. Its reconstruction has emerged as the gold-standard surgical procedure for recurrent lateral patellar instability — a condition that, if untreated, leads to progressive chondral damage, patellofemoral arthritis, and functional disability. An understanding of MPFL anatomy, the pathoanatomy of instability, appropriate patient selection, surgical principles, and potential pitfalls is essential for every orthopaedic surgeon.
Anatomy and Biomechanics
The MPFL is a broad, flat capsular thickening that runs from the proximal third of the medial patellar border to its femoral origin, the Schottle point — located between the adductor tubercle and the medial epicondyle. Radiographically, this point is defined as:
- 1 mm anterior to the posterior cortex extension line
- 2.5 mm distal to the posterior origin of the medial femoral condyle
- Proximal to the most posterior aspect of the Blumensaat line on a true lateral radiograph
The ligament lies just distal to the vastus medialis obliquus (VMO) and deep to the medial retinaculum. It functions as the dominant medial soft-tissue restraint to lateral translation in early flexion, before bony trochlear engagement occurs. Understanding this anatomy is the foundation of any successful reconstruction.
Pathoanatomy of Patellar Instability
Patellar instability, analogous to glenohumeral instability, exists on a spectrum from subtle subluxation to frank dislocation. The etiology is almost always multifactorial, involving:
| Predisposing Factor | Details |
|---|---|
| Traumatic MPFL rupture | Most common mechanism; usually at patellar insertion on MRI |
| Trochlear dysplasia | Dejour classification (Types A–D); identified by crossing sign on lateral X-ray |
| Patella alta | Caton-Deschamps or Insall-Salvati index |
| Increased TT-TG distance | > 20 mm highly associated with instability |
| Ligamentous laxity | Generalised joint hypermobility |
| VMO weakness | Reduced dynamic medial stabilisation |
| Miserable malalignment | Femoral anteversion + genu valgum + pronated feet; exacerbates symptoms in adolescents |
The recurrence rate after first-time lateral dislocation ranges from 15–60%, with higher rates in younger patients, females, those with patella alta, and trochlear dysplasia. Dislocation is a frequent cause of haemarthrosis and commonly injures the articular cartilage of the medial patellar facet during spontaneous reduction.
Clinical Evaluation
History: Mechanism is typically external tibial rotation with a planted foot or a direct blow to the medial knee. A "pop" is often felt and should not be confused with an ACL injury.
Examination:
- Patellar apprehension test — positive (pathognomonic when at 30° flexion)
- J sign — lateral patellar jump at terminal extension
- Lateral patellar glide — 3 to 4 quadrants of lateral translation
- Assessment of generalised ligament laxity, Q-angle, limb alignment, and tibial torsion
Imaging
Plain radiographs: Anteroposterior, lateral, and Merchant (axial) views identify fractures, loose bodies, trochlear morphology, and patellar height. The crossing sign (trochlear groove line intersecting the anterior femoral condyle) on lateral view indicates trochlear dysplasia.
CT scan: Gold standard for measuring the TT-TG (tibial tubercle–trochlear groove) distance:
- Normal: 9–13 mm
- 15–20 mm: questionably abnormal
- > 20 mm: highly associated with patellar instability; indication for distal realignment
Also assesses trochlear dysplasia (Dejour classification) and patellar tilt.
MRI: Identifies MPFL tear (most frequently at the patellar insertion), chondral damage (medial patellar facet most vulnerable), and lateral femoral condyle bone bruising — a pattern characteristic of acute dislocation. MRI tends to underestimate TT-TG distance compared to CT.
Surgical Decision-Making
When to Operate?
Acute first-time dislocations are traditionally managed conservatively with a patellar stabilising brace and physiotherapy. Surgery on first-time dislocation is considered only if:
- A loose body or significant osteochondral fragment is present (requiring arthroscopic retrieval)
- Some centres advocate acute MPFL repair at the medial epicondyle, though this remains controversial
Recurrent instability is the principal indication for MPFL reconstruction.
Choosing the Correct Procedure
The decision tree is based on TT-TG distance and associated pathoanatomy:
| Condition | Procedure |
|---|---|
| Normal TT-TG (< 15 mm), no bony abnormality | Isolated MPFL reconstruction (proximal realignment) |
| TT-TG > 20 mm or increased Q-angle | MPFL reconstruction + tibial tubercle anteromedialization (Fulkerson osteotomy) |
| Significant trochlear dysplasia | Consider trochleoplasty in selected cases |
| Patella alta | Consider distalisation of tibial tubercle |
Procedures that have fallen out of favour and should NOT be performed in isolation:
- VMO advancement (Green procedure)
- Medial retinacular plication alone
- Isolated lateral release — explicitly contraindicated for patellar instability
MPFL Reconstruction: Surgical Technique
Graft Selection
- Autograft: Gracilis or semitendinosus tendon (hamstring)
- Allograft: Same tendons; used when autograft is unavailable or to preserve donor-site integrity
- A doubled gracilis graft provides adequate strength and matches native MPFL dimensions
Step-by-Step Technique
1. Diagnostic Arthroscopy
- Assess chondral surfaces, identify loose bodies or osteochondral fragments
- Address any intra-articular pathology before ligament reconstruction
2. Patellar Tunnel Preparation
- Two diverging bone tunnels (or single tunnel) are created in the proximal-medial patella
- Care is taken not to penetrate the anterior cortex (risk of patellar fracture)
- Tunnels positioned at the proximal-third of the patella, avoiding violation of the articular surface
3. Femoral Tunnel Preparation (Most Critical Step)
- The Schottle point is identified using intraoperative fluoroscopy on a true lateral view
- A guide pin is placed and confirmed before drilling
- A 5–6 mm tunnel is drilled to accept the folded graft or an interference screw
4. Graft Passage and Fixation
- Graft passed deep to the medial retinaculum, superficial to the joint capsule, in the natural MPFL plane
- Patellar end fixed first with interference screws or suture anchors
- Femoral end tensioned and fixed at 30–45° of knee flexion, with the patella held in neutral position
- Graft tensioning is the most technically demanding step — the graft must allow free patellar glide with a physiological check, not a rigid constraint
5. Intraoperative Assessment
- Full passive range of motion tested; should achieve full flexion without tightness
- Lateral patellar translation rechecked — should allow 1–2 quadrants (normal), not be overconstrained
Femoral Tunnel Positioning: Critical Biomechanical Principle
This is the single most important technical consideration. Because the MPFL behaves near-isometrically only when the femoral attachment is at the Schottle point, malposition has predictable biomechanical consequences:
| Femoral Tunnel Position | Consequence |
|---|---|
| Too proximal | Graft is tight in flexion → restricted ROM, medial instability |
| Too distal | Graft is loose in flexion → persistent instability |
| At Schottle point | Near-isometric behaviour throughout arc of motion |
Intraoperative fluoroscopy is not optional — it is mandatory for accurate placement.
Complications
| Complication | Cause / Notes |
|---|---|
| Medial patellar instability | Overtightening of the graft; creates iatrogenic medial instability |
| Medial patellar osteoarthritis | Increased medial patellofemoral contact pressure from overtightening |
| Patellar fracture | Patellar tunnels too close to anterior cortex or too large |
| Graft failure / recurrent instability | Malpositioned femoral tunnel (most common technical error) |
| Stiffness / loss of flexion | Graft tensioned too tight or at wrong knee angle |
| Numbness | Saphenous nerve branches at risk during medial dissection |
Distal Realignment: Tibial Tubercle Anteromedialization (Fulkerson Osteotomy)
When TT-TG > 20 mm or Q-angle is elevated, proximal realignment alone is insufficient. The Fulkerson osteotomy transfers the tibial tubercle anteriorly and medially, achieving:
- Reduction of the TT-TG distance
- Decreased lateral patellar vector
- Anterior translation unloads the distal patellofemoral joint
Absolute contraindication: proximal arthrosis of the medial patellar facet (medialization worsens medial contact stress).
Post-operative Rehabilitation
- 0–2 weeks: Hinged brace locked in extension; toe-touch weight-bearing
- 2–6 weeks: Progressive weight-bearing, range of motion exercises (0–90°)
- 6–12 weeks: Full weight-bearing, quadriceps strengthening (emphasis on VMO)
- 3–6 months: Sport-specific rehabilitation
- Return to sport: Typically at 6–9 months with full quadriceps strength and confidence in stability
Outcomes
- Success rates for MPFL reconstruction in appropriately selected patients: 90–95% return to sport, low redislocation rates (< 5%)
- Poor outcomes are associated with unaddressed bony pathology (trochlear dysplasia, elevated TT-TG) and malpositioned femoral tunnels
- Combined MPFL reconstruction with distal realignment produces superior results when TT-TG > 20 mm compared to MPFL reconstruction alone
Conclusion
MPFL reconstruction is the cornerstone of surgical management for recurrent lateral patellar instability. Success depends on a thorough understanding of the patho-anatomy, meticulous patient selection based on the TT-TG distance and associated bony abnormalities, accurate femoral tunnel placement at the Schottle point under fluoroscopic guidance, and appropriate graft tensioning. Failure to address coexisting bony dysplasia, or technical errors in tunnel positioning, are the leading causes of poor outcomes. When performed correctly in the right patient, MPFL reconstruction reliably restores patellofemoral stability and enables return to sport with low recurrence rates.
— Miller's Review of Orthopaedics, 9th Edition, pp. 190, 365–366
add recent advances and give this answer for 15 marks
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Good. The textbooks confirm dynamic CT utility and the surgical decision framework. I now have all the material needed. Here is the refined 15-mark essay incorporating recent advances.
MPFL Reconstruction — Postgraduate Essay (15 Marks)
Introduction
The medial patellofemoral ligament (MPFL) is the primary passive restraint to lateral patellar displacement, providing approximately 50–60% of medial restraining force, particularly between 0–30° of knee flexion — the critical range before bony trochlear engagement stabilises the patella. Traumatic disruption of this ligament is the defining injury in lateral patellar dislocation. Recurrence after first-time dislocation ranges from 15–60%, with higher rates in younger patients, females, those with patella alta, and trochlear dysplasia. MPFL reconstruction has become the cornerstone of surgical management for recurrent patellar instability.
Anatomy
The MPFL originates from the proximal third of the medial patellar border and inserts at the Schottle point on the femur — located:
- 1 mm anterior to the posterior femoral cortex extension line
- 2.5 mm distal to the posterior origin of the medial femoral condyle
- Proximal to the most posterior aspect of the Blumensaat line on a true lateral radiograph
It lies just distal to the VMO and superficial to the knee joint capsule. Precise knowledge of this anatomy is the foundation of a successful reconstruction.
Pathoanatomy and Patient Assessment
Patellar instability is multifactorial. Predisposing factors include:
- Traumatic MPFL rupture (typically at the patellar insertion on MRI)
- Trochlear dysplasia — Dejour Types A–D; identified by the crossing sign or supratrochlear spur on lateral X-ray
- Patella alta — Caton-Deschamps or Insall-Salvati ratio
- Elevated TT-TG distance — > 20 mm highly associated with instability
- VMO weakness and generalised ligamentous laxity
- Miserable malalignment syndrome (femoral anteversion + genu valgum + pronated feet)
Examination: Patellar apprehension test, J sign, lateral glide assessment (3–4 quadrants), and assessment of alignment.
Imaging:
- Radiographs: Crossing sign, trochlear morphology, patellar height
- CT: Gold standard for TT-TG distance (normal 9–13 mm; > 20 mm = indication for distal realignment) and Dejour grading
- MRI: Confirms MPFL tear site, chondral damage (medial patellar facet most vulnerable), and lateral femoral condyle bone bruise pattern
Surgical Decision-Making
| Clinical Scenario | Procedure |
|---|---|
| Recurrent instability, TT-TG < 15 mm | Isolated MPFL reconstruction |
| TT-TG > 20 mm / increased Q-angle | MPFL reconstruction + Fulkerson tibial tubercle anteromedialization |
| Significant trochlear dysplasia | MPFL reconstruction ± trochleoplasty |
| Patella alta | Consider tibial tubercle distalization |
Procedures explicitly abandoned:
- VMO advancement (Green procedure), medial retinacular plication alone
- Isolated lateral release is contraindicated for patellar instability
Surgical Technique
Graft: Gracilis or semitendinosus autograft (or allograft). The doubled gracilis graft matches native MPFL dimensions and strength adequately.
Steps:
- Diagnostic arthroscopy — address chondral lesions, remove loose bodies
- Patellar fixation — two diverging bone tunnels in the proximal-medial patella (care to avoid anterior cortex breach and articular surface)
- Femoral tunnel — most critical step; Schottle point confirmed by intraoperative fluoroscopy on a true lateral view
- Graft passage — deep to medial retinaculum, superficial to capsule, in the native MPFL plane
- Tensioning and fixation — femoral end fixed at 30–45° of flexion with patella in neutral; must allow free patellar glide, not overconstrain
Femoral tunnel position — biomechanical imperative:
| Tunnel placement | Consequence |
|---|---|
| Too proximal | Tight in flexion → stiffness, medial instability |
| Too distal | Loose in flexion → recurrent instability |
| Schottle point | Near-isometric throughout motion arc |
Complications
- Medial patellar instability / osteoarthritis — from overtightening (most common serious complication)
- Patellar fracture — from large or misdirected patellar tunnels
- Recurrent lateral instability — malpositioned femoral tunnel
- Stiffness — graft too tight or tensioned at wrong flexion angle
- Saphenous nerve injury — during medial dissection
Recent Advances
1. Dynamic (4D) CT
Emerging tool for assessing patellar tracking in motion rather than static anatomical measurements alone. Allows cine-movie reconstructions demonstrating real-time subluxation patterns; utility for surgical planning continues to be evaluated. — Miller's Review of Orthopaedics, 9th Ed.
2. MPFL Repair with Internal Brace Augmentation
Acute primary MPFL repair (traditionally at the medial epicondyle) augmented with a synthetic internal brace/suture tape has gained interest for first-time dislocations with a repairable ligament. Provides immediate load-sharing, protecting the repair during biologic healing. Results comparable to reconstruction in carefully selected acute cases, with the advantage of preserving native tissue.
3. All-Soft-Tissue Patellar Fixation (Suture Anchor Technique)
Traditional patellar bone tunnels carry the risk of fracture, especially in small or dysplastic patellae. Modern techniques using suture anchors or trans-osseous suture fixation without large tunnels have reduced this risk while maintaining equivalent fixation strength. Particularly relevant in skeletally immature patients and those with patella alta (thin patellar bone stock).
4. MPFL Reconstruction in Skeletally Immature Patients
Open physes previously deterred surgeons. Current evidence supports physeal-sparing MPFL reconstruction using soft-tissue fixation that avoids drilling across the distal femoral physis. Gracilis autograft wrapped around the adductor magnus tendon (Avikainen technique or modifications) achieves reliable fixation near the Schottle point without physeal violation. This has expanded surgical indications to younger adolescents with documented recurrent instability.
5. Combined MPFL + Trochleoplasty
For high-grade Dejour Type B/D trochlear dysplasia, sulcus-deepening trochleoplasty combined with MPFL reconstruction is now supported by medium-term studies showing superior redislocation rates compared to MPFL reconstruction alone. Previously feared for chondral damage, refined techniques demonstrate acceptable cartilage outcomes.
6. Medial Patellotibial and Patellomeniscal Ligament Reconstruction
Emerging anatomical research has highlighted the role of the medial patellotibial ligament (MPTL) and medial patellomeniscal ligament as secondary medial stabilisers. Reconstruction of these structures, particularly in cases with distal patellar instability or in combination with MPFL reconstruction, is being investigated to address residual instability after isolated MPFL reconstruction.
7. Computer Navigation and Robotic Assistance
Intraoperative navigation-assisted tunnel placement has been described to improve accuracy of femoral tunnel positioning at the Schottle point, reducing the most common cause of surgical failure (malpositioned tunnel) — though cost and availability currently limit routine adoption.
8. Biologics and Scaffold Augmentation
Platelet-rich plasma (PRP) applied at the graft-tunnel interface and collagen scaffold-augmented repair are under investigation to accelerate ligamentisation and graft incorporation, potentially shortening rehabilitation timelines. Evidence remains preliminary.
Outcomes
In appropriately selected patients with isolated soft-tissue instability:
- Redislocation rate after MPFL reconstruction: < 5%
- Return to sport: 90–95% at 6–9 months
- Poor outcomes correlate with unaddressed trochlear dysplasia, elevated TT-TG, and femoral tunnel malposition
When TT-TG > 20 mm, combined MPFL reconstruction with Fulkerson osteotomy yields superior results over MPFL reconstruction alone.
Conclusion
MPFL reconstruction is a technically demanding but highly effective procedure for recurrent lateral patellar instability. Its success hinges on accurate preoperative planning, fluoroscopy-guided Schottle point tunnel placement, and appropriate graft tensioning. Advances in dynamic CT, physeal-sparing techniques for adolescents, internal brace augmentation, combined trochleoplasty for high-grade dysplasia, and biologic augmentation are reshaping practice. The fundamental principle remains unchanged: address all contributing pathoanatomy — bony and soft-tissue — for a durable, isometric reconstruction.
— Miller's Review of Orthopaedics, 9th Edition, pp. 190, 365–366
bone graft subtitues
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive, textbook-sourced material across all categories. Here is the structured postgraduate essay.
Bone Graft Substitutes — Postgraduate Essay (15 Marks)
Introduction
Autologous bone graft has historically been the gold standard for achieving bone regeneration, possessing all three essential properties of an ideal graft material. However, its limitations — donor site morbidity, haematoma, nerve injury, chronic pain, and an inherently finite supply — have driven the development of a wide range of bone graft substitutes. These materials aim to replicate or augment the biologic and mechanical properties of native bone graft. Understanding their properties, mechanisms, clinical indications, and limitations is fundamental to modern orthopaedic and trauma surgery.
Properties of an Ideal Bone Graft
Every graft material is evaluated against three core properties:
| Property | Definition | Example |
|---|---|---|
| Osteogenic | Contains living cells that directly produce bone (MSCs, osteoblasts, osteocytes) | Autograft, bone marrow aspirate |
| Osteoinductive | Contains signals/growth factors that stimulate undifferentiated host cells to form bone | BMP, DBM |
| Osteoconductive | Provides a structural scaffold through which host bone can grow | Ceramics, allograft |
Additionally, an ideal substitute should provide structural integrity, be biocompatible, resorbable at a rate matching bone ingrowth, free of disease transmission risk, and readily available.
Autograft — The Gold Standard (Comparator)
| Form | Key Properties |
|---|---|
| Cancellous autograft | Osteogenic (excellent), osteoinductive (good), osteoconductive (excellent), rapid incorporation by creeping substitution; poor structural integrity |
| Cortical autograft | Good structural strength; slow incorporation via Haversian remodelling; osteogenic (fair); insufficiency fracture in 25% of massive grafts |
| Vascularised bone graft (e.g., free fibula) | Faster union, preserves cellular viability; best for irradiated tissue or large segmental defects; significant donor site morbidity |
Limitations: Donor site morbidity, limited volume, increased operative time.
Classification of Bone Graft Substitutes
Bone graft substitutes can be classified into:
- Allografts
- Ceramics (calcium phosphate, calcium sulfate)
- Demineralized Bone Matrix (DBM)
- Growth Factors (BMPs)
- Cell-Based Therapies (bone marrow aspirate, MSCs)
- Composite / Combination Materials
1. Allograft
Allograft is cadaveric bone processed to eliminate immunogenicity and disease transmission risk.
Forms and Processing
| Type | Immunogenicity | Osteoinduction | Structural Integrity |
|---|---|---|---|
| Fresh | Highest | Best (BMP preserved) | Good |
| Fresh-frozen | Moderate | BMP preserved | Good |
| Freeze-dried (lyophilized) | Lowest | Least (BMP largely destroyed) | Weakest |
Processing by freeze-drying or irradiation renders the material largely osteoconductive only — it functions as a scaffold but lacks osteogenic and osteoinductive properties.
Indications: Fracture nonunion (augmenting autograft when large volumes required); spinal fusion; acute fracture fixation (tibial plateau, tibial plafond, calcaneus, proximal humerus).
Advantages: Unlimited supply; no donor site morbidity; available in cortical, cancellous, or structural forms.
Disadvantages: No osteogenic potential; rare disease transmission risk; reduced mechanical strength after processing; variable biologic quality.
2. Demineralized Bone Matrix (DBM)
DBM is produced by acid extraction of allograft, removing the inorganic mineral phase and retaining the collagen scaffold, non-collagenous proteins, and growth factors — including BMPs.
- Osteoinductive: Retains variable BMP content (batch-dependent)
- Osteoconductive: Collagen scaffold supports ingrowth
- Osteogenic: None (no viable cells)
- Structural integrity: Poor — not load-bearing
Available as putty, gel, powder, or strips. Often used as an autograft extender to reduce the volume of autograft required.
Clinical pearls: Osteoinductive potency varies significantly between manufacturers and between batches — this is a major limitation. FDA classifies DBM as a tissue product, not a device, limiting standardisation.
3. Ceramics
a) Calcium Phosphate
Three forms exist, differing in resorption rate and mechanical strength:
| Form | Resorption | Compressive Strength |
|---|---|---|
| Hydroxyapatite (HA) | Slowest (still visible on X-ray > 10 years) | Good |
| Beta-tricalcium phosphate (β-TCP) | 6–18 months | Moderate |
| Calcium phosphate cement | Variable | Highest compressive strength of all ceramics |
All three are osteoconductive only — no osteoinductive or osteogenic properties.
Clinical applications:
- Augmentation of depressed tibial plateau fracture fixation (filling metaphyseal voids)
- Distal radius fracture fixation augmentation — RCT evidence supports better early grip strength and motion
- Calcaneus fracture ORIF — better preservation of Böhler angle
- Osteoporotic fractures requiring immediate weight-bearing (calcium phosphate cement augments screw purchase)
Resorption rate hierarchy (fastest → slowest):
Calcium sulfate > β-TCP > Hydroxyapatite
b) Calcium Sulfate
- Osteoconductive only; resorbs rapidly (6–12 weeks)
- Provides compressive strength but loses it quickly as it resorbs
- Primary role in modern practice: antibiotic delivery vehicle (dissolvable local antibiotic depot in infected cases)
- Rapid resorption limits its utility as a standalone bone graft substitute
4. Bone Morphogenetic Proteins (BMPs)
BMPs are members of the TGF-β superfamily and are the most potent known osteoinductive agents. They act by binding to cell surface receptors and activating the SMAD signalling pathway, directing mesenchymal stem cells toward osteoblastic differentiation.
| BMP | Clinical Indication | Approved Use |
|---|---|---|
| BMP-2 (recombinant human BMP-2, rhBMP-2 / INFUSE®) | Acute open tibia fractures; anterior lumbar interbody fusion | FDA approved |
| BMP-7 (OP-1 / Osigraft®) | Tibial nonunions; posterolateral spinal fusion (humanitarian device exemption) | Limited approval |
| BMP-3 | No osteogenic activity | Not used clinically |
Mechanism: Delivered on an absorbable collagen sponge carrier; induces local osteoprogenitor cell differentiation.
Advantages: Eliminates donor site morbidity; potent osteoinduction; reproducible supply.
Complications and controversies:
- Ectopic bone formation — most significant concern; can cause radiculopathy, dysphagia, or airway compromise (anterior cervical use)
- Osteolysis — paradoxical early resorption at the graft site
- Cancer risk — debated; epidemiological concern raised for BMP-2, not definitively proven
- Cost — significantly more expensive than autograft
- Supraphysiologic doses used clinically may account for many adverse effects
5. Cell-Based Therapies
a) Bone Marrow Aspirate (BMA)
- Contains mesenchymal stem cells (MSCs), haematopoietic progenitors, and growth factors
- Harvested from the iliac crest via percutaneous aspiration; minimal morbidity
- Osteogenic and weakly osteoinductive; no structural properties
- Often combined with an osteoconductive carrier (ceramic or allograft)
- Concentration using centrifugation (bone marrow aspirate concentrate, BMAC) increases MSC yield and efficacy
b) Mesenchymal Stem Cells (MSCs)
MSCs are multipotent adult progenitor cells capable of differentiating into osteoblasts, chondrocytes, and adipocytes. Originally described in bone marrow by Friedenstein in the 1960s and later characterised by Arnold Caplan (1990), MSCs are now known to be widely distributed — found in adipose tissue, periosteum, synovium, and muscle.
The International Society for Cell Therapy (2006) defines MSCs by:
- Plastic adherence in culture
- Expression of CD73, CD90, CD105 surface markers
- Absence of haematopoietic markers
- Tri-lineage differentiation potential (bone, fat, cartilage)
Clinical relevance: Delivered with a scaffold, MSCs represent the frontier of bone tissue engineering. Results to date remain variable due to inconsistency in cell populations, doses, timing, and patient heterogeneity.
6. Composite and Combination Materials
Recognising that no single substitute replicates all three properties of autograft, composite grafts combine:
- Osteoconductive scaffold (ceramic or allograft) +
- Osteoinductive signal (DBM or BMP) +
- Osteogenic cells (BMA or MSCs)
This triad approach most closely mimics autologous bone graft. Commercial examples include combinations of β-TCP with DBM, or HA/TCP scaffolds seeded with BMA.
Autograft extenders: When autograft volume is limited, combining a small amount of autograft with an osteoconductive ceramic or allograft effectively "extends" the osteogenic stimulus across a larger volume.
Comparative Summary Table
| Material | Osteoconductive | Osteoinductive | Osteogenic | Structural | Disease Risk | Supply |
|---|---|---|---|---|---|---|
| Autograft (cancellous) | Excellent | Good | Excellent | Poor | None | Limited |
| Autograft (cortical) | Fair | Fair | Fair | Excellent | None | Limited |
| Allograft | Fair | Fair (fresh only) | None | Good | Small | Unlimited |
| DBM | Good | Fair | None | Poor | Small | Unlimited |
| Hydroxyapatite | Fair | None | None | Fair | None | Unlimited |
| β-TCP | Fair | None | None | Fair | None | Unlimited |
| Ca phosphate cement | Fair | None | None | Best (compressive) | None | Unlimited |
| Ca sulfate | Fair | None | None | Poor (rapid resorption) | None | Unlimited |
| BMP-2/7 | None | Excellent | None | None | None | Unlimited |
| BMA/BMAC | Poor | Poor | Good | None | None | Limited (autologous) |
Recent Advances
- Magnesium phosphate cements (MPCs): Higher solubility than calcium phosphates; designed to degrade faster and more predictably — early animal studies promising as an alternative to slowly resorbing calcium phosphate cements
- Synthetic peptides and small molecules: Mimetics of BMP signalling domains to achieve osteoinduction without the large protein molecule and associated ectopic ossification risk
- 3D-printed scaffolds: Patient-specific hydroxyapatite/TCP scaffolds fabricated to exact defect geometry using additive manufacturing; allows precise porosity gradients to optimise vascular ingrowth
- Gene therapy-enhanced grafts: Viral vector delivery of BMP genes into MSCs or local tissue to achieve sustained local BMP expression — investigational
- Exosome-based therapy: Extracellular vesicles derived from MSCs containing osteogenic microRNAs — non-cellular alternative under investigation
- Dynamic CT for planning: Allows precise volumetric quantification of bone defects to guide substitute selection and volume calculation
Clinical Decision Framework
| Clinical Scenario | Preferred Substitute |
|---|---|
| Small-to-medium nonunion with viable biology | Autograft ± DBM as extender |
| Large segmental defect | Vascularised autograft (free fibula) ± allograft strut |
| Acute tibial plateau/calcaneus fixation void | Calcium phosphate cement |
| Open tibia fracture (Grade IIIA/B) | rhBMP-2 on absorbable collagen sponge |
| Tibial nonunion after failed fixation | BMP-7 ± autograft |
| Spinal fusion | rhBMP-2 (ALIF); autograft/allograft (posterolateral) |
| Infected bone void | Calcium sulfate + antibiotic |
| Limited autograft volume | Autograft + osteoconductive ceramic composite |
Conclusion
Bone graft substitutes have expanded the surgical armamentarium for bone regeneration, each offering a specific combination of osteoconductive, osteoinductive, and osteogenic properties. No single substitute yet matches the gold standard of autologous cancellous bone graft, which remains uniquely osteogenic. The ideal strategy involves selecting a substitute — or combination — based on the specific defect characteristics, available biology, and mechanical demands. Advances in cell therapy, 3D bioprinting, and molecular osteoinduction continue to narrow this gap, promising truly autograft-equivalent substitutes in the near future.
— Miller's Review of Orthopaedics, 9th Edition, pp. 35, 131 | Rockwood and Green's Fractures in Adults, 10th Edition, pp. 89–95



