Brachial cyst
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a complete overview of branchial (cleft) cysts:
Branchial Cleft Cyst
Also called a lateral cervical cyst or lymphoepithelial cyst, a branchial cleft cyst is a congenital developmental anomaly of the neck arising from incomplete obliteration of the branchial apparatus during embryogenesis.
Embryological Origin
During embryonic development, the pharyngeal pouches form "out-pocketing" structures that normally give rise to glandular elements (thymus, parathyroids, etc.). Their connections with the pharyngeal lumen — the pharyngobranchial ducts — should obliterate. Failure of obliteration results in a branchial sinus or cyst.
There are two competing theories:
- Cysts are remnants of patent pharyngobranchial ducts
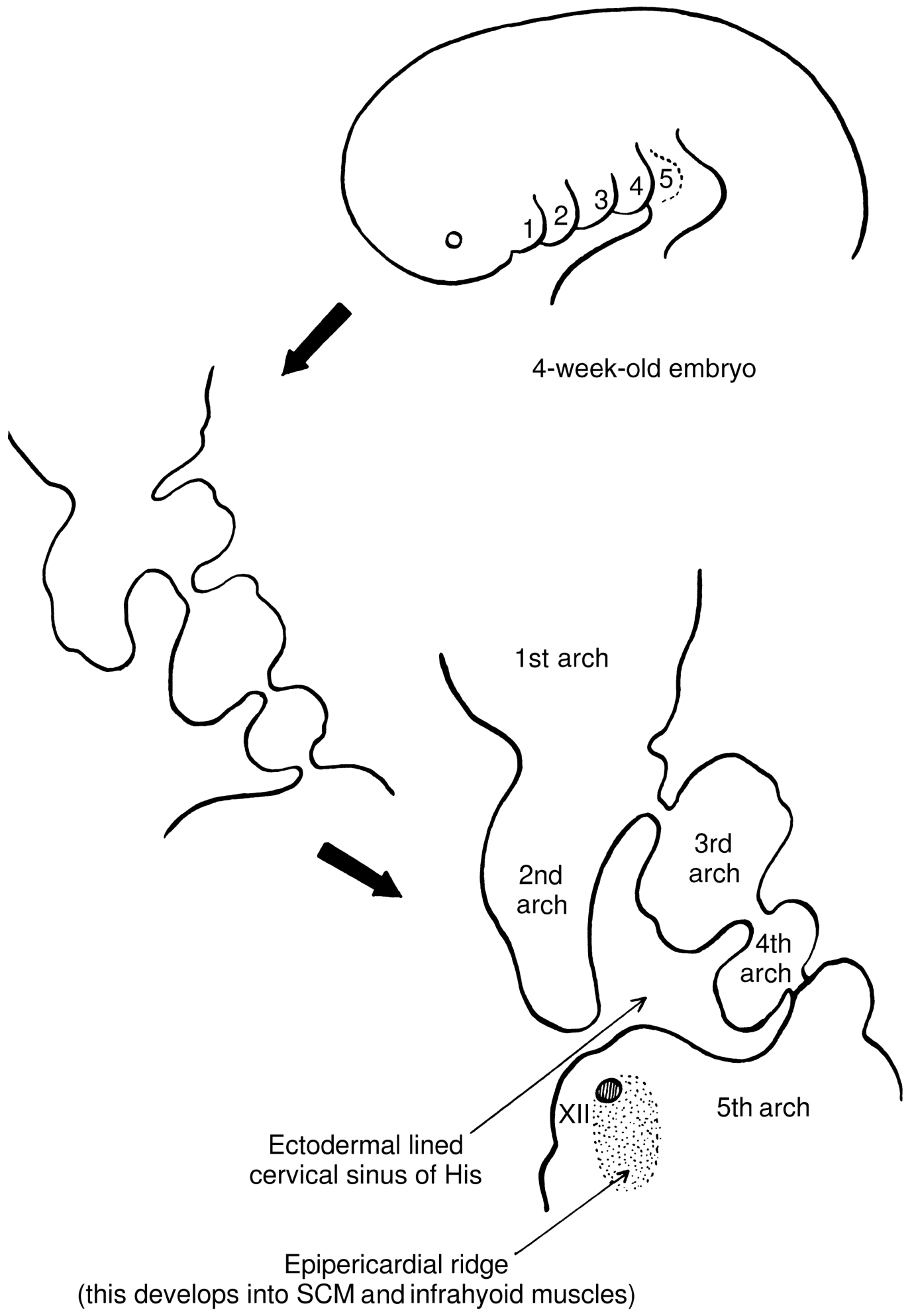
- Cysts are remnants of the cervical sinus of His (an ectodermal-lined structure formed by overgrowth of the 2nd arch over arches 3–5)
Types by Arch of Origin
The vast majority (~90%) arise from the 2nd branchial arch. The cutaneous opening, when present, is always anterior to the anterior border of the sternocleidomastoid (SCM), deep to the platysma (a 2nd arch derivative).
| Type | Origin | Course | Opens Into |
|---|---|---|---|
| 2nd arch (most common, 90%) | Cervical sinus / 2nd pharyngobranchial duct | Deep to 2nd arch derivatives, superficial to 3rd arch derivatives; superficial to CN XII, anterior to SCM; between internal and external carotid arteries; deep to stylohyoid ligament | Tonsillar fossa |
| 3rd arch | 3rd pharyngobranchial duct | Subplatysmal; superficial to CN XII, deep to internal carotid & CN IX; pierces thyrohyoid membrane above internal branch of superior laryngeal nerve | Pyriform fossa |
| 4th arch | 4th pharyngobranchial duct | Right: loops around subclavian artery; Left: may be intrathoracic, medial to ligamentum arteriosum | Lower pyriform sinus or larynx |
Clinical Features
- Most commonly seen in young adults (20–40 years), though can present at any age
- Presents as a smooth, painless, compressible mass along the anterior border of the SCM, frequently at the junction of the superior and middle thirds, just below the angle of the mandible
- May swell and become tender during upper respiratory tract infections (classic history)
- Slow-growing; typically 2–5 cm in diameter
- Usually no sinus tract is visible externally (distinguishing pure cyst from sinus)
- Infection is a frequent cause of presentation
Pathology
- Lining epithelium: stratified squamous or pseudostratified ciliated columnar epithelium
- Cyst wall: fibrous with prominent lymphoid tissue and germinal centers (characteristic feature — also why it is called a lymphoepithelial cyst)
- Contents: clear/watery or mucinous fluid; may contain desquamated cells and granular debris
Anatomical Relationships (2nd arch cyst — surgical importance)
When a 2nd arch cyst passes superiorly through the bifurcation of the common carotid artery (at the level of vertebrae CIII/CIV), it passes:
- Between the internal and external carotid arteries
- Between the stylohyoid ligament and the glossopharyngeal (CN IX) and hypoglossal (CN XII) nerves
- The vagus (CN X) and spinal accessory (CN XI) nerves lie posterior to the cyst
- Terminates at the medial border of the pharyngeal constrictor muscles
These cranial nerves are vulnerable to injury during surgical excision due to their anatomic intimacy with the cyst tract.
Diagnosis
- CT or MRI — to delineate the full extent of the cyst and tract prior to surgery
- Clinically: characteristic location + age + enlargement with infections
Treatment
Surgical excision of the cyst and its complete associated tract. Incomplete excision leads to recurrence.
Important Distinction: Malignancy
- Branchial cleft cysts rarely undergo malignant transformation
- When a cystic neck mass is found in an older patient, especially smoker/drinker, metastatic squamous cell carcinoma (from the oropharynx, tonsil, or base of tongue — especially HPV-related) must be excluded before labeling it a branchial cyst
- "Most cystic SCCs in the neck are metastases from cancers of the upper aerodigestive tract" — Robbins Pathologic Basis of Disease
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | KJ Lee's Essential Otolaryngology | Gray's Anatomy for Students | Dermatology 2-Volume Set 5e
Embroyolgy of pharyngeal arches
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced content for a complete answer. Let me compile it.
Embryology of the Pharyngeal (Branchial) Arches
Overview & Timing
The pharyngeal arches begin developing in the 4th week of embryonic life as neural crest cells migrate into the future head and neck regions. By the end of week 4, four pairs of arches are visible externally as oblique ridges separated by pharyngeal clefts (grooves). The 5th and 6th arches are rudimentary and not visible on the surface — their components are incorporated into the 4th arch in humans. Sonic hedgehog (Shh) and homeobox gene Dlx2 signaling play key roles in arch formation and patterning.
Structural Composition of Each Arch
Each pharyngeal arch has five components — covered externally by ectoderm and internally by endoderm:
| Component | Origin | Gives rise to |
|---|---|---|
| Mesenchyme core | Neural crest cells (predominantly) + paraxial mesoderm | Skeletal elements, connective tissue, dermis, smooth muscle |
| Muscle | Paraxial mesoderm | Arch-specific muscles |
| Cranial nerve | CNS | Arch-specific nerve |
| Aortic arch artery | Lateral plate mesoderm | Arch-specific vessel |
| Cartilaginous bar | Neural crest | Arch-specific skeletal elements |
"Each pharyngeal arch is characterized by its own muscular components. The muscular components of each arch have their own cranial nerve, and wherever the muscle cells migrate, they carry their nerve component with them." — Langman's Medical Embryology
Derivatives of Each Pharyngeal Arch
Arch 1 — Mandibular Arch
Nerve: CN V (mandibular branch of trigeminal)
| Component | Derivative |
|---|---|
| Cartilage (Meckel's cartilage) | Malleus, incus (ossicles); sphenomandibular ligament; anterior ligament of malleus — the rest of Meckel's cartilage disappears |
| Bone (membranous ossification) | Maxilla (via maxillary process), premaxilla, zygomatic bone, part of temporal bone, squamous temporal bone, mandible |
| Muscles | Muscles of mastication (temporalis, masseter, lateral & medial pterygoids), mylohyoid, anterior belly of digastric, tensor tympani, tensor veli palatini |
| Other | Contributes to external ear, external auditory meatus, middle ear bones |
Arch 2 — Hyoid Arch (Reichert's Cartilage)
Nerve: CN VII (facial nerve)
| Component | Derivative |
|---|---|
| Cartilage (Reichert's) | Stapes, styloid process of temporal bone, stylohyoid ligament, lesser cornu of hyoid bone, upper part of hyoid body |
| Muscles | Muscles of facial expression, stylohyoid, posterior belly of digastric, stapedius |
Arch 3
Nerve: CN IX (glossopharyngeal nerve)
| Component | Derivative |
|---|---|
| Cartilage | Greater cornu of hyoid bone, lower part of hyoid body |
| Muscles | Stylopharyngeus (the only muscle from 3rd arch) |
Arch 4 & 6 (combined in humans)
Nerve: CN X (vagus) — superior laryngeal nerve (4th arch) and recurrent laryngeal nerve (6th arch)
| Component | Derivative |
|---|---|
| Cartilages | Laryngeal skeleton — thyroid cartilage, cricoid cartilage, arytenoid, corniculate, and cuneiform cartilages |
| Muscles | Pharyngeal constrictors (4th arch); intrinsic laryngeal muscles (6th arch); cricothyroid |
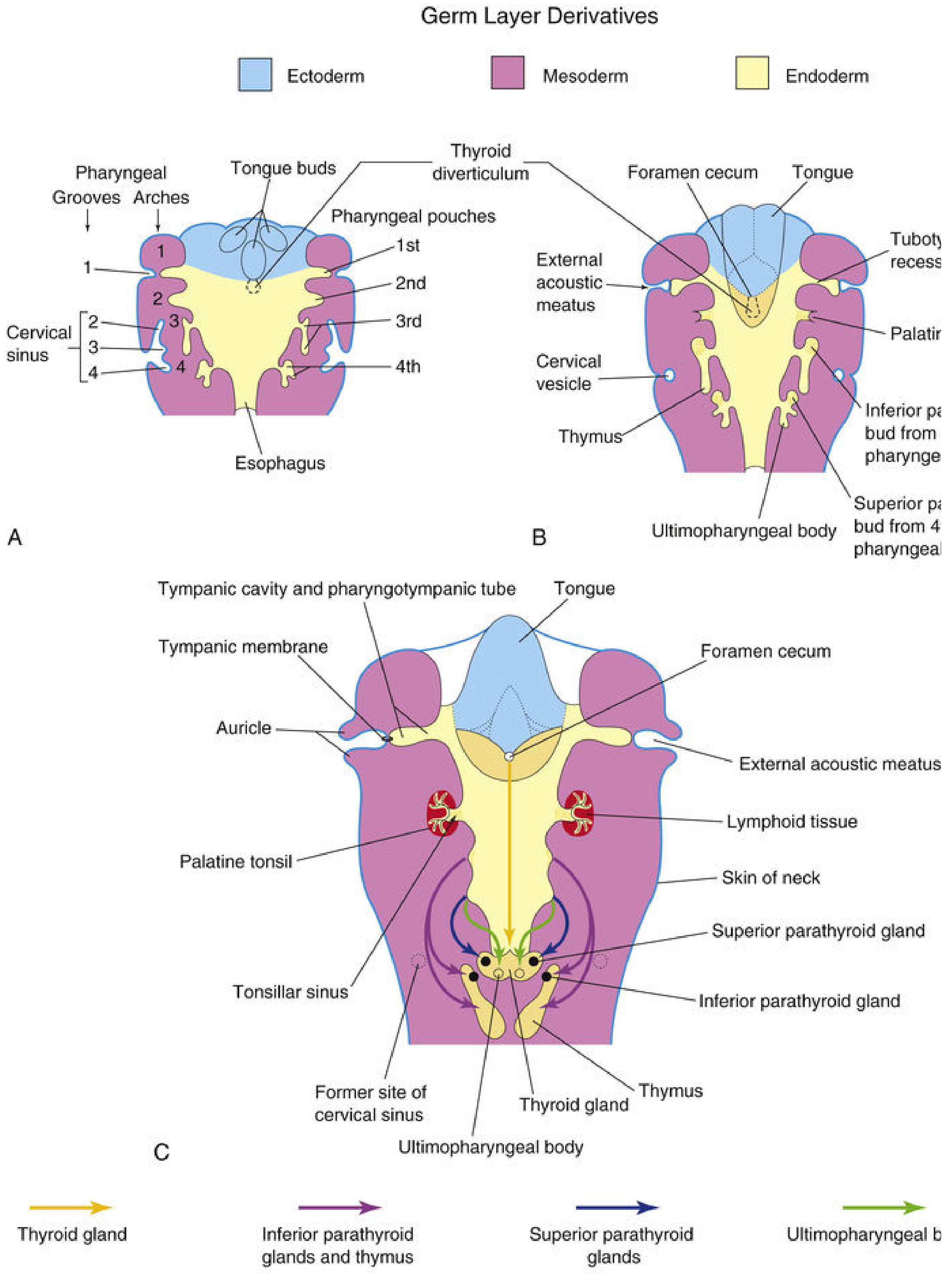
Pharyngeal Pouches (Endodermal — internal)
The endoderm lining the inside of the pharynx forms outpouchings between the arches called pharyngeal pouches. Four pairs are well defined (the 5th is rudimentary).
| Pouch | Derivative |
|---|---|
| 1st | Tubotympanic recess → tympanic cavity, mastoid antrum, pharyngotympanic (Eustachian) tube; contributes to tympanic membrane |
| 2nd | Palatine tonsil; tonsillar sinus (fossa) |
| 3rd | Dorsal part → inferior parathyroid glands (parathyroid III); Ventral part → thymus |
| 4th | Superior parathyroid glands (parathyroid IV); small ventral part → ultimopharyngeal body |
| 5th (rudimentary) | Ultimopharyngeal body → parafollicular C cells of the thyroid (secrete calcitonin) |
Clinical pearl: Because parathyroid III descends with the thymus (which migrates far caudally), parathyroid III ends up inferior to parathyroid IV in the adult — hence "inferior parathyroid" comes from the 3rd pouch and "superior parathyroid" from the 4th pouch.
Pharyngeal Clefts / Grooves (Ectodermal — external)
The ectoderm on the outside forms grooves between the arches called pharyngeal clefts.
| Cleft | Fate |
|---|---|
| 1st | Contributes to external auditory meatus |
| 2nd, 3rd, 4th | Buried by overgrowth of the 2nd arch → form the transient cervical sinus of His; normally obliterate completely |
Failure of obliteration of the cervical sinus gives rise to branchial cysts, sinuses, and fistulas.
Pharyngeal Arch Nerves — Summary
| Arch | Cranial Nerve | Key function |
|---|---|---|
| 1st | CN V (trigeminal — mandibular branch) | Sensory to face, teeth, mucosa; motor to muscles of mastication |
| 2nd | CN VII (facial) | Motor to muscles of facial expression; taste from anterior 2/3 tongue (via chorda tympani) |
| 3rd | CN IX (glossopharyngeal) | Stylopharyngeus; taste/sensation from posterior 1/3 tongue |
| 4th | CN X (superior laryngeal) | Cricothyroid, pharyngeal constrictors |
| 6th | CN X (recurrent laryngeal) | Intrinsic laryngeal muscles |
"The nerve of the fourth arch becomes the superior laryngeal nerve, which supplies the cricothyroid muscle and constrictor muscles of the pharynx. The nerve of the sixth arch becomes the recurrent laryngeal nerve, which supplies various laryngeal muscles." — The Developing Human
Aortic Arch Arteries
Each arch also carries an aortic arch artery. Their adult derivatives:
| Aortic Arch | Adult Derivative |
|---|---|
| 1st | Maxillary artery (largely disappears) |
| 2nd | Stapedial artery, hyoid artery (largely disappears) |
| 3rd | Common carotid artery; proximal internal carotid artery |
| 4th (Left) | Arch of the aorta |
| 4th (Right) | Proximal right subclavian artery |
| 6th (Left) | Left pulmonary artery; ductus arteriosus |
| 6th (Right) | Right pulmonary artery |
Clinical Significance
| Condition | Mechanism |
|---|---|
| Branchial cyst / sinus / fistula | Persistence of cervical sinus (2nd–4th clefts) or pharyngobranchial duct |
| DiGeorge syndrome | Failure of 3rd & 4th pouch development → absent thymus + absent parathyroids (T-cell deficiency + hypocalcaemia); caused by 22q11 deletion |
| First arch syndromes (Treacher Collins, Pierre Robin) | Defective neural crest migration into 1st arch → mandibulofacial deformities |
| Ectopic parathyroid | Failure of normal migration of parathyroid III/IV |
Sources: The Developing Human — Moore & Persaud | Langman's Medical Embryology | THIEME Atlas of Anatomy (General Anatomy)
Digeorge syndrome
This is a shared conversation. Sign in to Orris to start your own chat.