Liver abscess management post pig tail catheter insertion
Reading File
Finding Sources
Finding Sources
Searching PubMed
"liver abscess" AND "percutaneous drainage" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative surgical textbooks. Let me compile the full answer.
Liver Abscess Management Post Pigtail Catheter Insertion
Overview
Percutaneous catheter drainage (PCD) with a pigtail catheter is the standard of care for pyogenic liver abscesses (PLA), effective in 80-90% of cases. Once the drain is in, management shifts to a structured post-drainage protocol covering catheter care, antibiotics, monitoring, and stepwise escalation.
1. Catheter Management
When to remove the drain
- Catheter output must be low AND clear before removal - this is the primary criterion
- Most drains remain in place for 1-2 weeks, but duration varies based on output volume and abscess size
- Perform flushing/irrigation of the catheter with sterile saline (typically 10-20 mL) every 8-12 hours to maintain patency and prevent occlusion
- If the catheter becomes occluded, tissue plasminogen activator (tPA) instillation can facilitate drainage of a blocked catheter
- For very large abscesses (>10 cm), multiple catheters may be required simultaneously
Drain output interpretation
| Output | Action |
|---|---|
| Purulent, high volume | Maintain catheter, continue flushes |
| Decreasing, becoming clear | Continue monitoring, plan for removal |
| Minimal and clear | Remove catheter |
| Sudden increase after initial decrease | Rule out biliary communication or secondary infection |
Sinogram / contrast study
- Before removal, a sinogram (contrast injection through the drain) can confirm the cavity has collapsed and rule out a persistent biliary communication - this is particularly important as biliary fistula is a key cause of treatment failure and recurrence.
2. Antibiotic Therapy
Empiric regimen (adjust to culture)
| Situation | Recommended Regimen |
|---|---|
| Standard (community-acquired) | Piperacillin-tazobactam OR Ceftriaxone + Metronidazole |
| Biliary source / prior biliary instrumentation | Add Enterococcus coverage (ampicillin, or vancomycin if resistant) |
| Prior biliary instrumentation or liver transplant | Consider carbapenem for ESBL coverage |
| Anaerobic coverage | Metronidazole or clindamycin (excellent abscess penetration) |
Route and duration
- Parenteral antibiotics for 2-3 weeks, or until a clear clinical response is established (defervescence, improving WBC, decreasing drain output)
- Transition to oral antibiotics for an additional 2-4 weeks, guided by sensitivities
- Total treatment: 4-6 weeks in most cases
- Do not prolong antibiotic therapy based solely on residual imaging findings - the abscess cavity frequently persists on imaging long after clinical cure. Resolution of cavity lags behind clinical improvement by weeks
Culture-driven therapy
- Blood cultures (positive in >50% of PLAs) and abscess fluid cultures are mandatory before starting antibiotics
- Common organisms:
- Biliary source: E. coli, Klebsiella spp., Enterococcus
- Enteric/portal source: Bacteroides fragilis, anaerobes
- Cryptogenic: Klebsiella pneumoniae (often monomicrobial, hypervirulent strains increasingly recognized)
- Gram-positive: Streptococcus spp. (most common in US/European series)
- Be alert to hypervirulent K. pneumoniae (hvKP) which may cause metastatic septic emboli (endophthalmitis, meningitis, lung) - screen for this in Asian patients or those with cryptogenic abscess
3. Clinical Monitoring Post-Drainage
Parameters to track
- Fever curve - should defervescence within 48-72 hours; persistent fever after 72 hours warrants reassessment
- WBC / CRP - trend downward expected within the first week
- LFTs - alkaline phosphatase, bilirubin (elevated in ~50-80%), transaminases
- Drain output - volume, character, color (bilious output suggests biliary communication)
- Blood glucose - diabetes is a strong independent risk factor for complicated course and prolonged hospitalization
Follow-up imaging
- CT or ultrasound at 4-6 weeks to assess abscess cavity resolution
- Earlier imaging is warranted if:
- Fever persists beyond 72 hours post-drainage
- Drain output increases or becomes bilious
- Clinical deterioration
4. Treating the Underlying Source
This is as important as managing the abscess itself. Common sources and their management:
| Source (% of cases) | Management |
|---|---|
| Biliary obstruction / cholangitis (35%) | ERCP + stenting, stone extraction; biliary drainage within 24-48 hours significantly reduces mortality |
| Portal pyemia from GI tract (appendicitis, diverticulitis) (20%) | Address primary GI pathology (appendectomy, sigmoid resection) |
| Cryptogenic (10%) | Colonoscopy to rule out occult colorectal malignancy (particularly important for monomicrobial Klebsiella abscess) |
| Iatrogenic (post-TACE, biliary instrumentation) | Adjust antibiotic spectrum, monitor for ESBL organisms |
5. Indications for Surgical Escalation
Approximately 10-20% of patients fail percutaneous drainage and require surgery. Indications include:
- Failure of percutaneous drainage after 5-7 days (persistent fever, no reduction in cavity size)
- Large, multiloculated abscesses that cannot be adequately drained percutaneously
- Ruptured abscess with peritonitis or intraperitoneal collection
- Concurrent intraabdominal pathology requiring surgery (perforated diverticulitis, peritonitis)
- Biliary communication not amenable to endoscopic management
- Multiple large abscesses requiring open irrigation and drain placement
Preferred surgical approach: laparoscopy (allows full peritoneal examination and is especially valuable when the source has not been identified). Laparotomy reserved for complex cases. Partial hepatectomy of the diseased segment is sometimes advocated for large multiloculated abscesses failing percutaneous drainage, but has not been shown superior to open surgical drainage plus irrigation.
6. Special Scenarios
Amebic liver abscess (ALA)
- Does not routinely require drainage - most respond to metronidazole alone (750 mg TID x 10 days or tinidazole 2 g/day x 5 days)
- Drainage is indicated if:
- No clinical improvement within 3-5 days of metronidazole
- Left lobe abscess (high risk of pericardial rupture)
- Abscess >10 cm (risk of rupture)
- Diagnostic uncertainty
- Follow with luminal amebicide: Paromomycin 25-30 mg/kg/day in 3 divided doses x 7 days
Recurrent / refractory abscess
- Recurrence risk: 12-38% (higher with diabetes, unidentified source, large initial abscess, biliary communication)
- Strategy: repeat aspiration or re-drain, repeat microbiology, ensure adequate antibiotic duration and source control
- If multiple attempts fail: surgical drainage
Diabetic patients
- Higher risk of treatment failure, longer hospitalization, and mortality
- Some centers favor earlier/more aggressive drainage plus longer antibiotic courses in diabetic patients
7. Complications to Monitor For
| Complication | Features |
|---|---|
| Rupture into peritoneum | Acute abdomen, hemodynamic instability - emergency laparotomy |
| Pleuropulmonary involvement | Sympathetic effusion, empyema, hepatobronchial fistula (especially ALA - 20-30%) |
| Portal vein / hepatic vein thrombosis | Portal hypertension, Budd-Chiari (rare) |
| Metastatic septic emboli (hvKP) | Endophthalmitis, meningitis, lung abscess |
| Biliary fistula | Bilious drain output; requires ERCP/biliary stenting |
| Catheter dislodgement | Imaging-guided repositioning or new drain |
Summary Algorithm (Post-Drain)
Pigtail inserted
↓
Culture-guided IV antibiotics (2-3 weeks)
+ Catheter flush q8-12h
+ Treat underlying source (ERCP / surgery)
↓
Monitor: fever, drain output, WBC, LFTs
↓
Improving (fever resolves, output decreasing, clear)
→ Oral antibiotics (2-4 weeks) → Follow-up CT at 4-6 weeks → Remove drain when minimal clear output
↓
Failing after 72 hours
→ Repeat imaging → Rule out biliary fistula, multiloculation
→ Consider additional drain / repositioning
→ Escalate to surgery if needed
Sources:
- Current Surgical Therapy, 14th ed. - Pyogenic Liver Abscess chapter, pp. 440-442
- Bailey and Love's Short Practice of Surgery, 28th ed. - Liver Abscess, ch. 69
- Yamada's Textbook of Gastroenterology, 7th ed. - Pyogenic Liver Abscess, ch. 102
- Goldman-Cecil Medicine, International ed. - Treatment of Liver Abscess
- Mulholland and Greenfield's Surgery, 7th ed. - Pyogenic Abscess
Erythema nodosum and pyoderma gangrenosum images
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have an excellent set of clinical images from authoritative dermatology textbooks. Here is the complete visual and clinical summary:
Erythema Nodosum (EN)
EN is the most common inflammatory panniculitis - a reactive septal panniculitis, not a primary disease. It is a hypersensitivity response to various triggers.
Key clinical features: Bilateral, symmetric, deep, tender, erythematous nodules 1-10 cm on the anterior shins (pretibial area). No ulceration, no scarring. Lesions evolve from bright red to bruise-like purple-green ("erythema contusiforme") over days. Female predominance (3:1 to 6:1). Associated systemic symptoms: fever, malaise, arthralgias (ankles, knees).
Fig. 1 - Erythema Nodosum (Andrews', Fig. 23.1)
Bilateral, symmetric, erythematous tender nodules on the anterior lower legs - the classic presentation

Fig. 2 - Erythema Nodosum (Fitzpatrick's, Fig. 73-1)
Erythematous nodules on the anterior lower legs, showing the typical bilateral distribution

Fig. 3 - Chronic Erythema Nodosum / EN Migrans (Andrews', Fig. 23.2)
Chronic form: unilateral or asymmetric, less tender, prolonged course of months - note the purple-red bruise-like discoloration on the forearm

Common causes of EN:
| Category | Examples |
|---|---|
| Infections | Streptococcus (most common in children), TB, Yersinia, fungi (coccidioidomycosis, histoplasma) |
| Inflammatory | IBD (Crohn's > UC), Sarcoidosis (Löfgren syndrome), Behçet |
| Drugs | Oral contraceptives, sulfonamides, bromides |
| Idiopathic | 37-60% of cases |
Pyoderma Gangrenosum (PG)
PG is a rare neutrophilic dermatosis - a sterile, destructive, ulcerative skin condition with characteristic morphology. Approximately 50% have an associated systemic disease (IBD most common, then hematologic disorders and inflammatory arthritis).
Key clinical features: Begins as an inflammatory pustule/nodule with violaceous halo → rapidly expands and ulcerates. Classic fully-developed lesion: painful ulcer with undermined, purple-to-gray ("gun-metal") overhanging borders. Pathergy in 20-30% (new lesions triggered by minor trauma - important to note pre-operatively). Heals with cribriform (sieve-like) atrophic scars. Lower extremities and trunk most common sites.
Fig. 4 - Pyoderma Gangrenosum (Andrews', Fig. 7.13)
Classic ulcerative PG: deep, necrotic, hemorrhagic ulcer with the characteristic undermined violaceous border

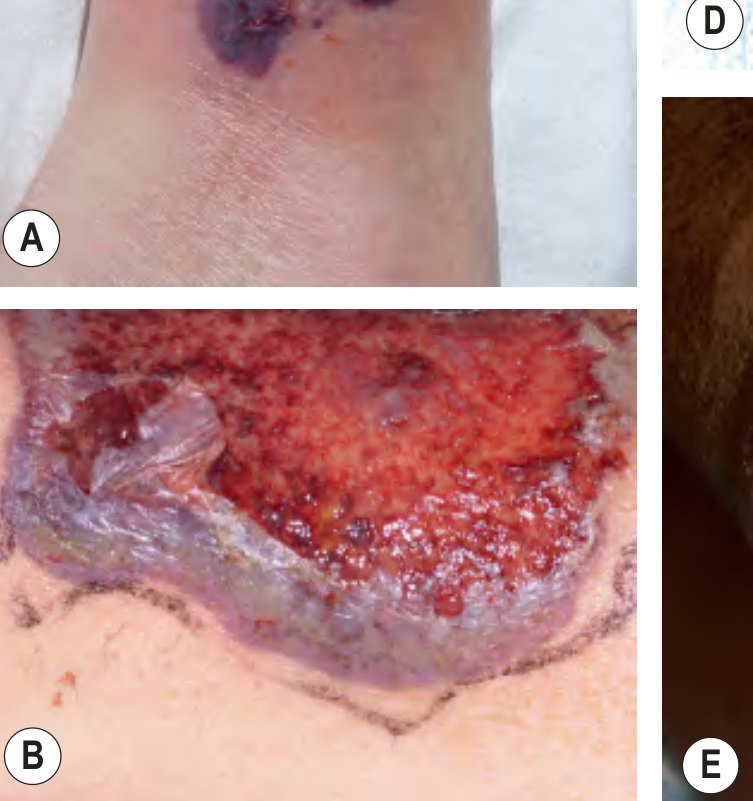
Fig. 5 - Pyoderma Gangrenosum, Clinical Presentations (Dermatology 5e, Fig. 25.10 A & B)
(A) Early PG with violaceous papules and pustules at the ulcer periphery on the ankle. (B) Classic ulcerative PG showing the hallmark undermined, overhanging violet-gray edge and surrounding violaceous border
PG Clinical Variants:
| Variant | Features | Associated Condition |
|---|---|---|
| Ulcerative (classic) | Painful ulcer, undermined violaceous border | IBD, RA |
| Bullous | Superficial, bullae → erosions, upper extremities/face | AML, myelodysplasia, IgA gammopathy |
| Pustular | Multiple sterile pustules, may not ulcerate | IBD (especially UC) |
| Vegetative (superficial granulomatous) | Superficial, chronic, cribriform, trunk, least aggressive | Often no systemic disease |
| Peristomal | Around stoma site | IBD with ostomy |
Key Differentiating Features: EN vs PG
| Feature | Erythema Nodosum | Pyoderma Gangrenosum |
|---|---|---|
| Morphology | Nodules/plaques, no ulceration | Ulcers with undermined purple border |
| Location | Anterior shins (bilateral) | Lower legs, trunk (any site) |
| Surface | Intact skin, bruise-like evolution | Open ulcer, necrotic base |
| Scarring | None | Cribriform (sieve-like) scars |
| Pathergy | No | Yes (20-30%) |
| Histology | Septal panniculitis | Sterile dermal neutrophilic abscess |
| Both shared | IBD association, lower extremity predilection, neutrophilic inflammation |
Sources: Andrews' Diseases of the Skin, 13th ed.; Fitzpatrick's Dermatology, 9th ed.; Dermatology 2-Volume Set, 5th ed.
This is a shared conversation. Sign in to Orris to start your own chat.