Cholecystectomy open and closed with operative steps indication and complications with position and port placement
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information I need from authoritative sources. Let me compile the comprehensive answer.
Cholecystectomy: Open and Laparoscopic
Sources: Schwartz's Principles of Surgery 11e, Bailey & Love's Short Practice of Surgery 28e, Maingot's Abdominal Operations, Mulholland & Greenfield's Surgery 7e, Fischer's Mastery of Surgery 8e
Historical Background
Carl Langenbuch performed the first open cholecystectomy in 1882. Philippe Mouret introduced laparoscopic cholecystectomy in France in 1987, which rapidly became the gold standard. Over 750,000 cholecystectomies are performed annually in the United States alone. - Schwartz's Principles of Surgery, p. 1438
Indications
Symptomatic (Absolute/Strong)
| Indication | Notes |
|---|---|
| Biliary colic / Symptomatic cholelithiasis | Most common indication; once symptomatic, >80% chance of recurrence or complication |
| Acute cholecystitis | Early (same-admission) laparoscopic approach preferred |
| Chronic cholecystitis | Recurrent attacks |
| Choledocholithiasis | With or without cholangitis |
| Gallstone pancreatitis | Cholecystectomy during same admission or within 2 weeks |
| Cholangitis / Obstructive jaundice | After biliary decompression |
| Acalculous cholecystitis / Biliary dyskinesia | Typical symptoms, HIDA ejection fraction <35% |
| Cholecystoenteric fistula | Gallstone ileus, Mirizzi syndrome |
Prophylactic Indications (Asymptomatic Gallstones)
Asymptomatic gallstones carry <20% lifetime risk of symptoms; prophylactic surgery is only justified in:
- Sickle cell disease (difficult to distinguish hepatic crisis from acute cholecystitis)
- Open bariatric surgery (rapid weight loss causes gallstones in ~30% of cases)
- Long-term total parenteral nutrition
- Chronic immunosuppression (post-transplant - masked inflammation)
- Gallbladder polyp >10 mm (malignant potential)
- Porcelain gallbladder (selected cases with malignant risk)
- Large gallstones >2.5 cm (cancer risk, esp. Native Americans)
- Congenital hemolytic anemias (hereditary spherocytosis)
- No access to healthcare (military, missionaries)
- Maingot's Abdominal Operations, p. 1015; Mulholland & Greenfield's Surgery, p. 3066
Preoperative Preparation
- Full blood count, renal and liver function tests, coagulation screen (PT)
- ECG and chest radiograph if medically indicated
- Antibiotic prophylaxis: second-generation cephalosporin at induction
- DVT prophylaxis: LMWH + antiembolic (TED) stockings
- Patient to void before the operation room to avoid catheterization
- Orogastric tube if stomach distended; removed at end of procedure
- Informed consent: procedure, alternatives, risks including bile duct injury and conversion
- Bailey & Love's, p. 1270
Predictors of Difficult Cholecystectomy
| Domain | Factors |
|---|---|
| History | Male sex, age >65, presentation >72-96 hours from onset, previous upper abdominal surgery, prior cholecystostomy |
| Examination | Morbid obesity, high ASA score |
| Labs | Abnormal liver function tests |
| Imaging | Thick-walled gallbladder (>4-5 mm), pericholecystic fluid, impacted stone in neck, Mirizzi syndrome |
Laparoscopic Cholecystectomy (Closed/MIS)
Position
- Supine with the surgeon standing at the patient's left side
- Alternative: split-leg (French) position with surgeon between the patient's legs - gives ergonomic access to the right upper quadrant
- Tuck one arm if intraoperative cholangiogram is planned (to allow fluoroscopy machine to be maneuvered)
- Table tilted reverse Trendelenburg + left lateral tilt to allow the bowel to fall away from the operative field
- Schwartz's Principles of Surgery, p. 1439
Pneumoperitoneum
- CO₂ gas to 12-15 mmHg
- Three techniques:
- Closed Veress needle technique - supraumbilical region (alternate access site if previous surgery/scars)
- Open Hasson technique (cut-down, safer in previous surgery)
- Optical viewing trocar technique
Port Placement (4-Port Standard Technique)
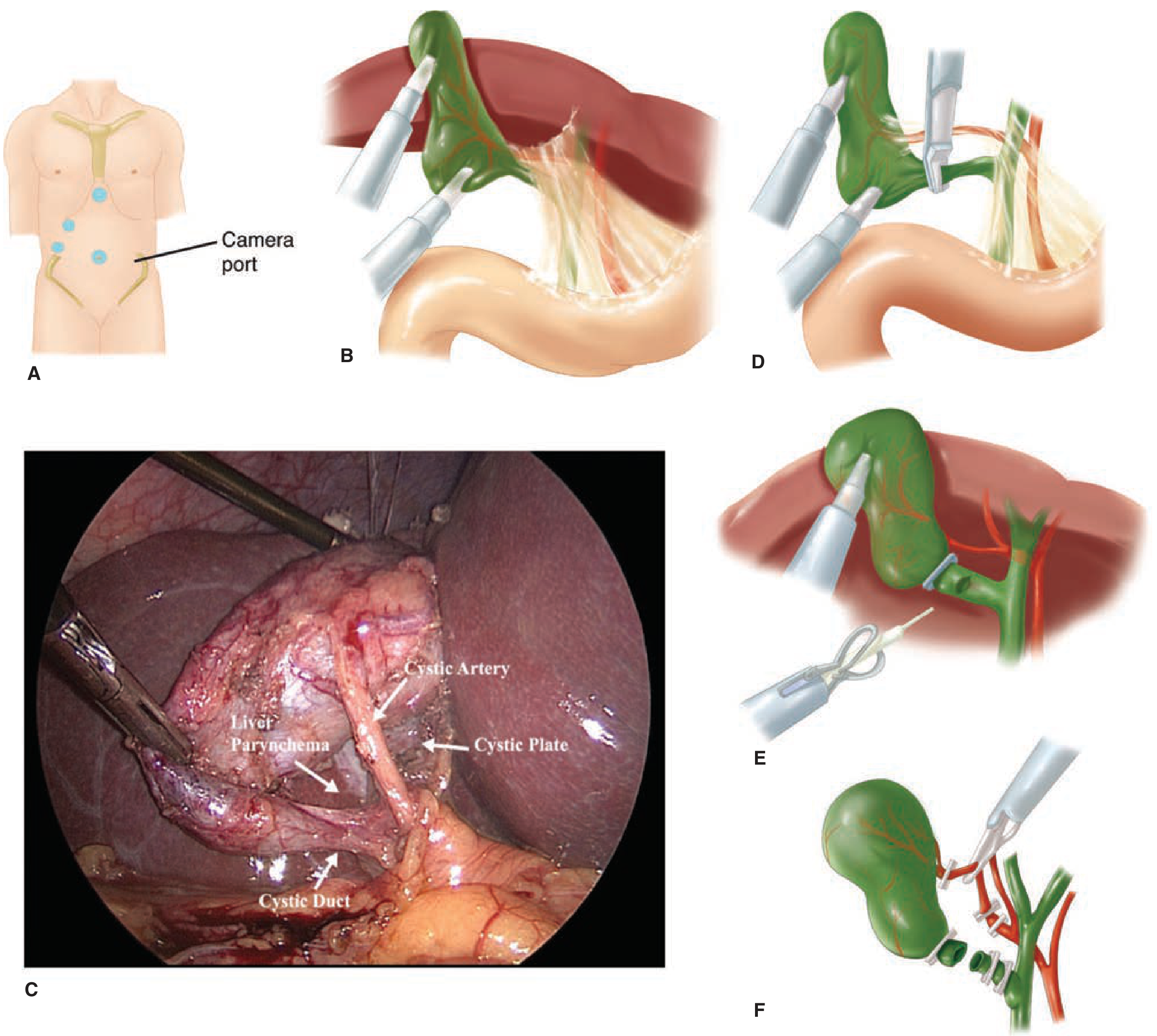
Figure: (A) Port placement - camera port at umbilicus + 3 additional ports. (B) Fundus retracted cephalad, infundibulum retracted inferolaterally to open Calot's triangle. (C) Intraoperative view showing Critical View of Safety (CVS) - cystic artery and duct clearly identified. (D) Clip placement on cystic duct. (E) Cholangiogram catheter insertion. (F) Clips placed, cystic duct divided. - Schwartz's Principles of Surgery
| Port | Size | Location | Purpose |
|---|---|---|---|
| Port 1 (Camera) | 5 or 10 mm | Supra-umbilical | Laparoscope (30° preferred) |
| Port 2 (Working) | 10 or 12 mm | Epigastrium (midline, subxiphoid) | Main working port - dissection, clips, stapler |
| Port 3 | 5 mm | Right mid-clavicular line (RUQ) | Grasper for infundibulum retraction |
| Port 4 | 5 mm | Right flank / anterior axillary line | Locking grasper for fundus retraction |
Additional ports may be added for retraction in difficult cases. - Schwartz's Principles of Surgery, p. 1439
Operative Steps - Laparoscopic Cholecystectomy
Step 1: Establish pneumoperitoneum and insert ports as above.
Step 2: Retraction
- Port 4 (right flank): assistant grasps the fundus and retracts it towards the patient's right shoulder (cephalad, over the liver edge)
- Port 3 (RMC): surgeon grasps the infundibulum (Hartmann's pouch) and retracts it inferolaterally (towards the patient's right side)
- This opens the hepatocystic triangle, increases the angle between the cystic duct and CBD, and limits dissection above Rouvière's sulcus
- B-SAFE landmarks: Bile duct, Sulcus of Rouvière, hepatic Artery, umbilical Fissure, Enteric/duodenum - used to orient the cognitive map
Step 3: Dissect the hepatocystic triangle (Calot's triangle)
- Using hook electrocautery (monopolar ~30 W, short intermittent bursts) from the epigastric port
- Clear all fat, fibrous, and areolar tissue from the hepatocystic triangle
- Dissect both the anterior AND posterior aspects of the triangle
- Safe zone: cephalad to the R4U line (from roof of Rouvière's sulcus to the umbilical fissure)
Step 4: Achieve the Critical View of Safety (CVS)
The CVS (Strasberg) requires ALL three criteria:
- The hepatocystic triangle is cleared of all fat and fibrous tissue
- The lower one-third of the gallbladder is separated from the cystic plate/liver bed
- Only two structures are seen entering the gallbladder (cystic duct + cystic artery)
CVS must be documented - photographically or on video. Difficulty achieving CVS is a red flag to stop dissection.
Step 5: Divide cystic artery and cystic duct
- Two clips proximally (at the base), one clip on the gallbladder side for both structures
- Divide between clips with scissors
- If cystic duct is too dilated for clips: use endoloop, laparoscopic stapler, or suture closure
Step 6: Intraoperative cholangiogram (optional but recommended selectively)
- Selective indications: abnormal LFTs, prior pancreatitis, jaundice, dilated CBD on USS, large duct + small stones, failed preoperative ERCP, or unclear anatomy
- Routine use detects CBD stones in ~7% of patients
- Technique: clip on proximal cystic duct → small anterior incision → insert cholangiogram catheter → fluoroscopy with contrast injection. Ideal cholangiogram shows filling of right and left hepatic ducts + drainage into duodenum + no filling defects
Step 7: Dissect gallbladder from liver bed
- Electrocautery dissection, staying on the cystic plate
- Watch for aberrant posterior bile ducts or arteries
- Before final division, use gallbladder as retractor for final field evaluation
Step 8: Final inspection and removal
- Check for bleeding, bile staining, confirm clip placement on cystic duct and artery
- Remove gallbladder via epigastric or umbilical port (often with retrieval bag; enlarge fascia if needed for large stones)
- Irrigate and retrieve any spilled stones
- Drain placement (under right liver lobe, via 5-mm port) if: severe inflammation, gangrene, spillage of bile, or anticipated accumulation - not routine
- Close fascial defects >10 mm at ports
- Schwartz's Principles of Surgery, pp. 1439-1443; Bailey & Love's, pp. 1270-1272
Tenets for Safe Cholecystectomy (Bailey & Love's Table 71.5)
| Step | Purpose |
|---|---|
| Correct retraction (fundus → right shoulder; infundibulum → inferolaterally) | Opens hepatocystic triangle; increases cystic duct-CBD angle |
| Recognize red flag signs (failure of progression, disorientation, poor visualization) | "Time out" - stop, reorient, seek second opinion |
| Achieve CVS | Conclusive identification before any clip placement |
| Expose cystic plate (lower ⅓ of GB from liver) | Confirms correct dissection plane |
| Separate GB from fossa, leaving cystic plate on liver | Prevents liver sinus bleeding and bile leak |
Bailout Strategies (when CVS cannot be achieved)
- Abort the procedure and return electively
- Convert to open cholecystectomy
- Tube cholecystostomy (14 Fr Foley catheter - bridge to definitive procedure)
- Subtotal cholecystectomy (open or laparoscopic) - safer than risky dissection
- Fundus-first approach
Open Cholecystectomy
Indications for Open Approach
- Hemodynamic instability
- Uncontrolled coagulopathy
- Frank peritonitis
- Severe COPD or CHF (EF <20%) - cannot tolerate pneumoperitoneum
- Conversion from laparoscopic (5% elective; 10-30% emergency/complicated)
- Concurrent laparotomy for another indication
- Schwartz's Principles of Surgery, p. 1439
Position
- Supine
- Bolster/roll under the right side to extend the right upper quadrant (optional)
- Arms extended on arm boards
Incision Options
- Right subcostal (Kocher) incision - most common; centered over the lateral border of the rectus muscle, about 2-3 cm below the costal margin
- Upper midline laparotomy - faster access, better for exploration
- Right upper transverse incision - alternative
Operative Steps - Open Cholecystectomy
Step 1: Exposure
- Kocher incision; deepen through subcutaneous fat, anterior rectus sheath, rectus muscle, posterior sheath, peritoneum
- Place packs on the hepatic flexure of colon, duodenum, and lesser omentum
- Retract with the assistant's hand ("It is the left hand of the assistant that does all the work" - Moynihan) or self-retaining retractor (e.g., Finochietto, Thompson)
Step 2: Expose the gallbladder
- Identify the fundus of the gallbladder
- An Allis/Duval/artery forceps is placed on the infundibulum for traction
Step 3: Dissect Calot's triangle (fundus-first OR infundibulum-first)
- Retrograde (top-down / fundus-first): dissect gallbladder off liver bed starting at fundus, working toward porta hepatis - used in difficult/inflamed cases
- Antegrade (infundibulum-first): dissect from neck downward - traditional technique
- Clear the hepatocystic triangle of all peritoneal and fibrofatty tissue to identify the cystic duct and cystic artery
Step 4: Define and ligate cystic artery
- The cystic artery typically arises from the right hepatic artery within Calot's triangle
- Ligate with 2-0 absorbable ties and divide (or clips)
Step 5: Define and ligate cystic duct
- Pass ligatures around the cystic duct and tie (2-0 absorbable)
- Place a locking clip or ligature on the proximal cystic duct near the CBD junction (confirming it is NOT the CBD)
- Divide between ligatures
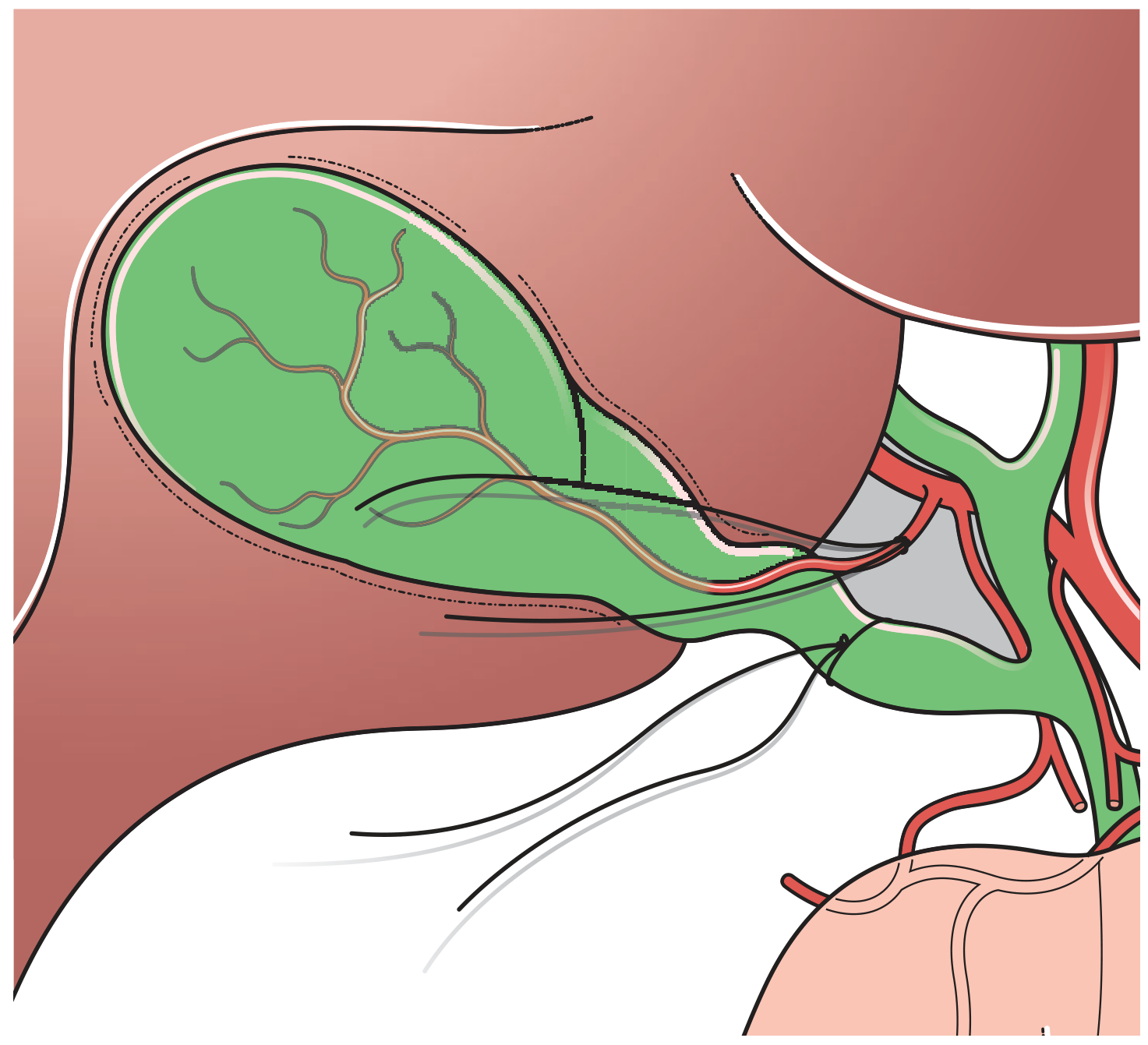
Figure: Ligatures passed and tied around the cystic artery and cystic duct. The shaded area represents Calot's triangle. - Bailey & Love's Surgery
Step 6: Intraoperative cholangiogram (selective, same criteria as laparoscopic)
Step 7: Dissect gallbladder from liver bed
- Sharp or electrocautery dissection, leaving cystic plate on liver
- Control any bleeding from liver sinuses with diathermy or hemostatic agents
Step 8: Partial/Subtotal cholecystectomy (if anatomy unclear)
- Remove as much gallbladder mucosa as possible
- Oversew or close the cystic duct stump with absorbable sutures
- Wide drainage of the area
Step 9: Closure
- Check for bile leak or bleeding
- Drain placement if indicated (sub-hepatic drain)
- Close peritoneum and fascial layers in anatomic layers
- Skin closure
Intraoperative Cholangiogram (IOC)
| Selective Indications |
|---|
| History of jaundice or abnormal LFTs |
| Prior biliary pancreatitis |
| Dilated CBD on preoperative ultrasound |
| Large duct, small stones on imaging |
| Failed or unavailable preoperative ERCP |
| Intraoperative anatomical uncertainty |
Routine IOC detects CBD stones in ~7% of cases. - Schwartz's Principles of Surgery, p. 1443
Complications
Intraoperative
| Complication | Notes |
|---|---|
| Bile duct injury (BDI) | Most feared; laparoscopic 0.3-0.6%, open 0.2-0.3% |
| Right hepatic artery injury | Often accompanies BDI due to proximity |
| Bowel injury | Especially at Veress needle or trocar insertion |
| Major vascular injury | Aorta, IVC, portal vein - Veress/trocar insertion |
| Bleeding | From cystic artery, liver bed, trocar sites |
| Gallbladder perforation / stone spillage | Occurs in 5-40% of laparoscopic cases; spilled stones should all be retrieved |
Postoperative - Early
| Complication | Notes |
|---|---|
| Bile leak | From cystic duct stump, duct of Luschka, or bile duct injury; presents with RUQ pain, fever, bilioma |
| Postoperative jaundice | Must be urgently investigated (USS → MRCP/ERCP) |
| Intra-abdominal abscess | Especially if stones spilled |
| Wound infection | Lower with laparoscopic approach |
| Bleeding | Port site, cystic artery stump clip dislodgement |
| Retained CBD stones | May cause jaundice, cholangitis |
| Acute pancreatitis | CBD stone migration |
| Port-site hernia | Fascial defects >10 mm must be closed |
Postoperative - Late
| Complication | Notes |
|---|---|
| Bile duct stricture | Post-injury; presents with cholestatic jaundice, cholangitis |
| Biliary fistula | Chronic bile leak |
| Peritonitis | From unrecognized bile leak |
| Stone abscess / fistula | From retained spilled stones (months to years later) |
| Post-cholecystectomy syndrome | Residual or recurrent symptoms (~10-15%) |
| Pulmonary complications | More common with open approach |
Overall Mortality
- Open cholecystectomy: <1%; increases with age, comorbidities, acute presentation
- Laparoscopic: ~0.1%
- Bailey & Love's, p. 1273; Mulholland & Greenfield's Surgery, p. 3066
Strasberg Classification of Bile Duct Injuries
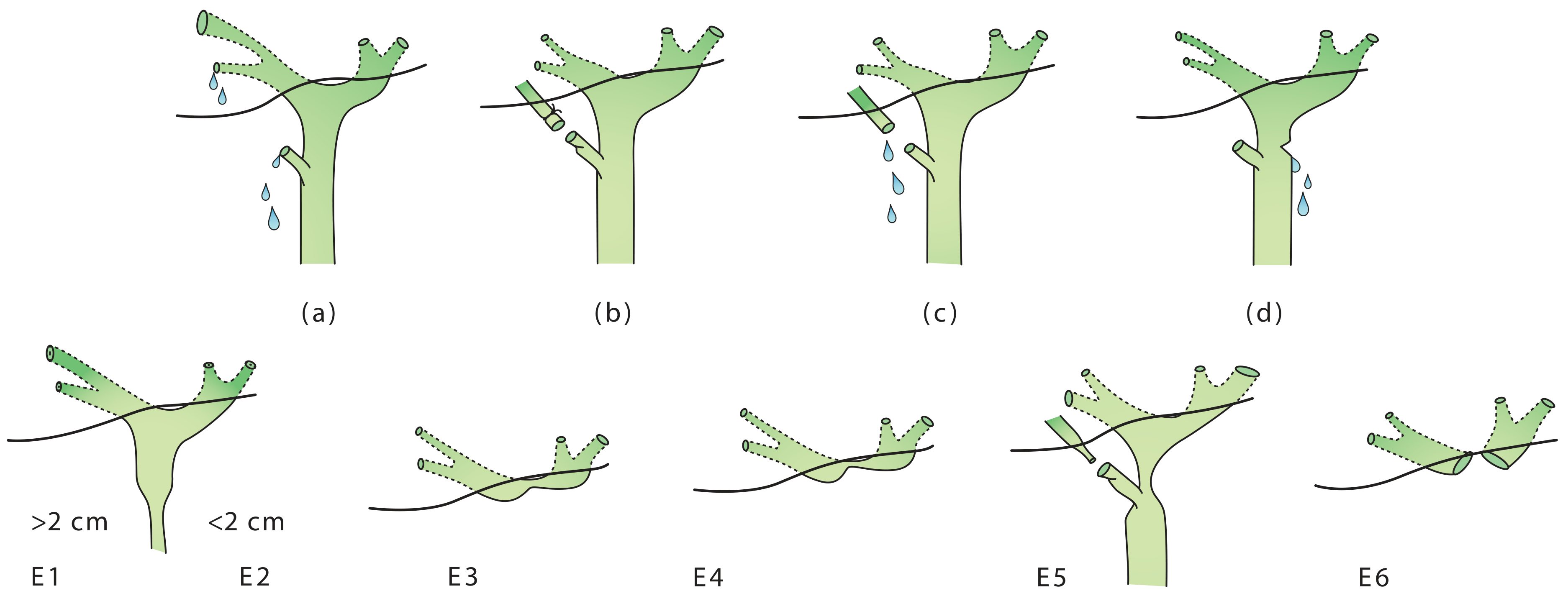
Strasberg classification: (a) Bile leak from cystic duct stump or minor biliary radical. (b) Occluded right posterior sectoral duct. (c) Bile leak from divided right posterior sectoral duct. (d) Bile leak from main bile duct without tissue loss. E1-E6: Transections/strictures of the main bile duct at various levels from the hilum. - Bailey & Love's Surgery, p. 1273
Management of Postoperative Jaundice / Suspected BDI
- Resuscitation + appropriate IV antibiotics
- Urgent RUQ ultrasound (intra/extrahepatic ductal dilatation? fluid collection?)
- MRCP to define anatomy (non-invasive)
- ERCP when therapeutic intervention needed (stone removal, stent across bile leak)
- Surgical repair (hepaticojejunostomy) for major duct injuries - ideally at a specialist hepatobiliary center
Conversion to Open
- Not a failure; should always be an option and discussed preoperatively
- Elective conversion rate: ~5%
- Emergency/complicated cases: 10-30%
- Indications for conversion:
- Unable to tolerate pneumoperitoneum
- Intraoperative complication not manageable laparoscopically
- Cannot achieve CVS / anatomical structures not clearly identified
- No progress after a set time period
- Suspected or confirmed bile duct injury requiring open repair
Comparison: Open vs. Laparoscopic
| Feature | Laparoscopic | Open |
|---|---|---|
| Incision | 4 small (5-12 mm) port sites | Kocher / midline (10-15 cm) |
| Pneumoperitoneum | CO₂, 12-15 mmHg | Not required |
| Pain | Significantly less | More |
| Hospital stay | Day case to 1-2 days | 3-5 days |
| Return to work | 1-2 weeks | 4-6 weeks |
| Wound infection | Lower | Higher |
| Bile duct injury rate | 0.3-0.6% (historically higher; now converging) | 0.2-0.3% |
| Mortality | ~0.1% | <1% |
| Visualization | Magnified laparoscopic view | Direct |
| Gold standard? | Yes | When lap not feasible/safe |
Key teaching point: The Critical View of Safety (CVS) is the single most important operative principle in cholecystectomy. No structure should be clipped or divided until CVS is conclusively achieved and documented. When CVS cannot be safely obtained, a bailout strategy should be employed rather than continuing dissection in a dangerous field. - Bailey & Love's Surgery 28e, p. 1271
Create a surgical procedure guide PDF for intraoperative reference
Reading File
Running Command
Writing File
Running Command
Running Command
Your PDF is ready for download:
Cholecystectomy Surgical Guide
PDF Document · PDF
The guide is 35 KB, A4 format, designed for intraoperative reference. Here's what's included across the pages:
| Section | Content |
|---|---|
| 1. Indications | Symptomatic + prophylactic indications with notes |
| 2. Contraindications & Conversion | Absolute CI to laparoscopic + intraoperative conversion triggers |
| 3. Preoperative Checklist | Bloods, antibiotics, DVT prophylaxis, consent items, predictors of difficult cholecystectomy |
| 4. Laparoscopic Cholecystectomy | Position, 4-port placement table, 9 numbered operative steps (color-coded), CVS alert box, bailout strategies |
| 5. Open Cholecystectomy | Position, incision options, 9 operative steps including subtotal technique |
| 6. Intraoperative Cholangiogram | Selective indications + step-by-step technique |
| 7. Complications | Intraoperative + postoperative tables; Strasberg BDI classification (A/B/C/D/E1–E5); BDI management protocol |
| 8. Open vs Laparoscopic | Side-by-side comparison table |
| 9. Anatomical Landmarks | Calot's triangle, Rouvière's sulcus, B-SAFE, R4U line, cystic plate, Duct of Luschka |
| 10. Safety Checklist | 22-item intraoperative WHO-style checklist |
This is a shared conversation. Sign in to Orris to start your own chat.