Role of lymph nodes dissection in early stage epithelial ovarian cancer and non epithelial ovarian cancer.Detailed overview. Explain the lymphatic drainage of ovary with diagram. Chances of lymph nodes involvement with different histolgies in ovarian cancer in early stages. Role. Of lymph nodes dissection in early stage with evidences in detail. Include latest evidences also. Also mention recommendations by guidelines.
lymph node dissection early stage ovarian cancer
lymph node involvement non-epithelial ovarian cancer germ cell sex cord stromal
ESGO NCCN guidelines 2024 2025 lymph node dissection early stage ovarian cancer recommendations
lymph node dissection early stage ovarian cancer guidelines recommendations
lymph node metastasis rate early ovarian cancer histology serous mucinous
germ cell tumor ovarian lymph node staging surgery
ICON1 ACTION trial lymphadenectomy early ovarian cancer staging survival
systematic lymphadenectomy early ovarian cancer survival upstaging adjuvant chemotherapy
ESGO ESMO 2024 early stage ovarian cancer lymphadenectomy recommendations histology specific
Lymph Node Dissection in Early-Stage Ovarian Cancer: A Detailed Overview
1. Lymphatic Drainage of the Ovary
Diagram
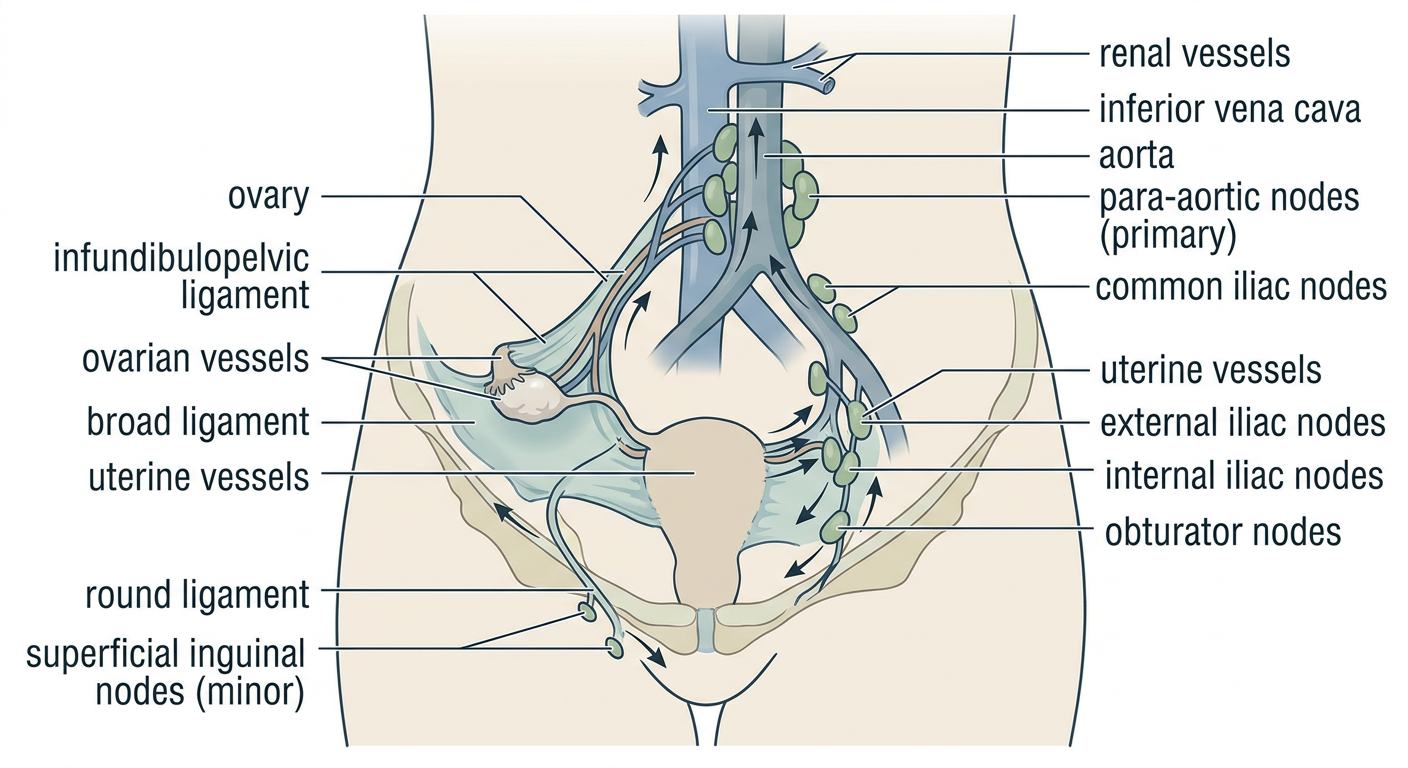
Pathways (Three Main Routes)
- Lymphatics travel alongside the ovarian vessels through the infundibulopelvic ligament
- Drain into the lateral aortic (para-aortic) and preaortic lymph nodes at the level of the renal vessels (L1-L2)
- This is the dominant pathway - explains why isolated para-aortic metastasis can occur without pelvic node involvement
- The right ovarian vein/lymphatics drain into nodes around the inferior vena cava; the left side drains into nodes alongside the left renal vein
- Lymphatics pass through the broad ligament following the uterine drainage
- Drain into the external iliac, internal iliac (hypogastric), obturator, and common iliac nodes
- Less dominant, but responsible for isolated pelvic node positivity
- A minor accessory route traveling alongside the round ligament
- Drains into superficial inguinal nodes
- Rarely clinically significant in ovarian cancer
Key clinical implication: Because para-aortic drainage predominates and can be involved in isolation (without pelvic node involvement), complete lymph node staging must include both para-aortic nodes up to the level of the renal vessels AND pelvic nodes. - Schwartz's Principles of Surgery, 11th Ed.; Campbell-Walsh Urology, 3-Vol Set
2. FIGO Staging and the Role of Lymph Nodes
| Stage | Definition |
|---|---|
| I | Confined to ovaries/fallopian tubes |
| II | Pelvic extension |
| IIIA1 | Positive retroperitoneal lymph nodes ONLY (no peritoneal spread) |
| IIIA1(i) | Nodal metastasis ≤10 mm |
| IIIA1(ii) | Nodal metastasis >10 mm |
| IIIA2 | Microscopic extrapelvic peritoneal + or - positive RPLNs |
3. Lymph Node Involvement Rates by Histology in Early-Stage Ovarian Cancer
Epithelial Ovarian Cancer (EOC)
| Histological Subtype | LN Positivity Rate (Early Stage) | Notes |
|---|---|---|
| High-grade serous carcinoma (HGSC) | ~10-29% | Highest risk; para-aortic involvement common |
| Clear cell carcinoma (CCC) | ~10-17% | Rodrigues Teixeira et al. (2022): 17.2% |
| High-grade endometrioid | ~10-15% | Similar risk to HGSC |
| Low-grade serous (LGSC) | ~5-10% | Lower but not negligible |
| Low-grade endometrioid | ~3-6% | Very low; Chen et al. (2021): LND may not benefit |
| Mucinous (expansile type) | ~0-2% | Extremely low; Kim et al. (2023): <1% upstaged by LN |
| Mucinous (infiltrative type) | ~5% | Slightly higher |
| Low-grade serous with non-invasive implants (borderline) | ~15-20%** | But these are often non-invasive implants in nodes |
- In a series of 142 systematically staged patients (Rodrigues Teixeira et al., Eur J Obstet Gynecol, 2022): overall positivity = 8.4%; HGSC = 10.4%, clear cell = 17.2%, endometrioid = 5.7%; no other histology (mucinous, LGSC, carcinosarcoma) had LN metastasis
- Chen et al. (2021, Front Oncol): overall occult LN metastasis rate = 7.1%; only 2.6% of apparent early-stage patients were upstaged by LN alone; mucinous/endometrioid low-grade tumors had minimal LN involvement
- Kim et al. (2023, Int J Gynecol Cancer): in 149 clinical stage I mucinous carcinomas, only 1 patient (0.7%) was upstaged by LN; lymphadenectomy had no survival benefit
Non-Epithelial Ovarian Cancer
| Subtype | LN Positivity | Notes |
|---|---|---|
| Dysgerminoma | ~25-30% | Highest among GCT; lymphophilic tumor |
| Immature teratoma | ~5-10% | Lower; grade-dependent |
| Yolk sac tumor (endodermal sinus) | ~10-15% | Moderate |
| Mixed GCT | Variable | Depends on dysgerminoma component |
| Subtype | LN Positivity | Notes |
|---|---|---|
| Granulosa cell tumor (GCT-A) | ~1-3% | Very rare LN involvement |
| Sertoli-Leydig cell tumor | ~3% | |
| Other SCST | <2% |
4. Role of Lymph Node Dissection in Early-Stage Ovarian Cancer
4A. Epithelial Ovarian Cancer (EOC)
Rationale FOR Lymphadenectomy
- Staging accuracy and upstaging: Up to 29% of apparently early-stage EOC has occult nodal metastasis, particularly HGSC. Without lymphadenectomy, these patients receive inadequate treatment. A complete lymph node dissection will upstage approximately one-third of patients who appear clinically confined to the pelvis (Schwartz's Surgery, 11th Ed.)
- Determination of adjuvant therapy: Stage IIIA1 disease (LN-only spread) now mandates different adjuvant chemotherapy intensity decisions compared to true stage I
- Potential therapeutic benefit: Removing metastatic nodes may have cytoreductive benefit
Rationale AGAINST Routine Lymphadenectomy
- Morbidity: Lymphedema (~10-15%), vascular injury, ureteric injury, chylous ascites, prolonged operative time, increased blood transfusion rates
- Uncertain survival benefit in RCTs: Observational studies show benefit, but RCT evidence does not confirm survival advantage
- Low yield in specific histologies: Mucinous, low-grade endometrioid tumors have minimal LN involvement
Evidence Summary
| Study | Population | OS Benefit | Conclusion |
|---|---|---|---|
| Zhou et al. 2016 (PMID 27272175) | Mixed stages; 3 RCTs + 11 retrospectives | OR=1.58 (CI 1.41-1.77), P<0.001 | LND associated with improved OS |
| Chiyoda et al. 2020 (PMID 32808497) | Early-stage EOC; 1 RCT + 4 cohorts | Observational HR=0.75 (CI 0.68-0.82); RCT HR=0.85 (CI 0.49-1.47, NS) | Observational studies: benefit; RCT: no survival benefit |
| Yang et al. 2023 (PMID 37667358) | 14 studies, 22,178 patients (eEOC) | HR=0.72 (CI 0.61-0.84), P<0.001; PFS HR=0.74 (CI 0.67-0.80) | LND associated with improved OS, PFS, lower recurrence |
Histology-Specific Approach
| Histology | Recommendation | Rationale |
|---|---|---|
| HGSC (stage I-II) | Systematic pelvic + para-aortic LND | High nodal positivity; upstaging changes management |
| Clear cell carcinoma | Systematic pelvic + para-aortic LND | ~17% nodal positivity; changes adjuvant decisions |
| High-grade endometrioid | Systematic pelvic + para-aortic LND | Similar to HGSC |
| Low-grade endometrioid | May omit systematic LND | Very low positivity; BGCS/Chen et al. support omission |
| Mucinous (expansile) | No routine LND; remove suspicious nodes | <1% LN positivity; lymphadenectomy confers no benefit |
| LGSC | Selective; remove suspicious nodes | Moderate evidence for benefit in serous histology |
4B. Non-Epithelial Ovarian Cancer
Malignant Germ Cell Tumors (MOGCT)
- Dysgerminoma is lymphophilic and has the highest LN involvement (~25-30%), but even here, the excellent chemosensitivity of these tumors (BEP regimen) means that post-operative chemotherapy effectively treats occult nodal disease
- Lv et al. 2023 (PMID 37139156): No significant difference in OS (P=0.621) or DFS (P=0.332) between LND and non-LND groups in 340 MOGCT patients
- Current approach: Unilateral salpingo-oophorectomy + peritoneal staging + removal of grossly enlarged nodes only (not systematic LND). Since virtually all patients with stage IC or higher receive BEP chemotherapy, the therapeutic addition of systematic LND is negligible
- Fertility preservation is a major consideration - unnecessary retroperitoneal dissection adds risk without benefit in this young patient population
Sex Cord-Stromal Tumors (SCST)
- Very low nodal positivity (~1-3%); lymph nodes are rarely involved unless other sites of spread are present
- Billmire et al. 2025 (PMID 40516498): Tumor found in 3-10% of sampled sites, and only from grossly abnormal tissue - confirming that systematic sampling of normal-appearing nodes/tissue adds no staging information
- Current standard: Inspect and palpate all retroperitoneal nodes; remove only grossly enlarged or suspicious nodes; routine systematic LND is not indicated
- NCCN guidelines note that surgical staging for malignant sex cord-stromal tumors "generally doesn't include removing nearby lymph nodes" when they appear normal
Borderline Ovarian Tumors (BOT)
- LN involvement reported in ~15-20%, but these are usually non-invasive implants in lymph nodes (microscopic peritoneal spread), not true nodal metastasis
- Fan et al. 2021 (PMID 34119365): Systematic review and meta-analysis found that neither lymph node involvement nor lymphadenectomy significantly affected survival in BOT
- Current recommendation: No routine lymphadenectomy; remove enlarged/suspicious nodes only
5. Sentinel Lymph Node Biopsy in Early-Stage EOC
- Para-aortic mapping: injection into the infundibulopelvic ligament - pooled detection rate 79.9% (95% CI 66.1-91.4%)
- Pelvic mapping: injection into the utero-ovarian ligament - pooled detection rate 42.7% (95% CI 28.5-57.3%) - significantly lower, limiting utility
- NPV: 100% for both para-aortic and pelvic regions
- Sensitivity: 97.8% (para-aortic), 100% (pelvic)
- Technetium-99m (99mTc) alone or combined with ICG had significantly higher detection rates than ICG alone
- Lower ICG volume (0.2-0.5 mL) performed better than 2 mL for both pelvic and para-aortic detection
- Low pelvic detection rates
- Lack of prospective validation
- Technical challenges related to ovarian anatomy vs. cervical/endometrial cancer
6. Guideline Recommendations (2024-2025)
ESGO-ESMO-ESP Consensus 2024 (PMID 38307807)
- High-grade EC, CCC, high-risk mucinous (stage I-II): Complete surgical staging including TAH+BSO+omentectomy + systematic pelvic and para-aortic LND + peritoneal biopsies + cytology = standard procedure
- LGSC with non-invasive peritoneal implants: Complete removal of implants + peritoneal staging; removal of enlarged/suspicious nodes recommended; routine systematic LND is NOT recommended
- Low-grade mucinous (expansile type), low-grade endometrioid: Systematic LND may not be warranted given very low metastatic risk
- Systematic pelvic and para-aortic LND should NOT be performed if macroscopic complete intra-abdominal resection achieved and nodes are non-suspicious on imaging and intraoperatively
- Remove enlarged/suspicious nodes to achieve complete resection
NCCN Guidelines 2025
- Systematic lymphadenectomy recommended for staging purposes in early-stage EOC
- For clear cell carcinoma: systematic LND included in staging surgery
- For malignant sex cord-stromal tumors: staging surgery is recommended but "generally doesn't include removing nearby lymph nodes" when normal
- LND should extend to the level of the renal vessels (left renal vein)
NICE Guidelines (UK)
- Systematic retroperitoneal lymphadenectomy (pelvic + para-aortic) recommended only when disease is presumed confined to the ovaries
- Not recommended when peritoneal disease is already present
BGCS Guidelines (British)
- Pelvic and para-aortic LND permitted when no peritoneal spread and nodal status expected to influence adjuvant treatment
- More conservative in low-risk histologies (expansile mucinous, low-grade endometrioid)
- Frozen section to confirm malignancy is advised before lymphadenectomy
JSGO (Japan) and Summary Table
| Guideline | Early-Stage EOC | Advanced EOC | Non-Epithelial |
|---|---|---|---|
| ESGO-ESMO 2024 | Systematic LND for HGSC/CCC/high-grade EC; suspicious-only for low-grade | Not for non-suspicious nodes | Not indicated |
| NCCN 2025 | Systematic LND; extends to renal vein | Not for non-suspicious nodes | Generally not LND |
| NICE | LND only if confined to ovary | Not routine | Not specified |
| BGCS | LND if no peritoneal spread | Selective | Conservative |
| JSGO | Systematic LND for staging | Not routine | Not routine |
7. Technical Aspects of Lymph Node Dissection
- Operative time increase: ~60-90 minutes
- Blood transfusion requirement significantly higher in LND group
- Surgery-related deaths: not significantly different
- Lymphedema, chylous ascites: 5-15%
- Grade ≥3 complications: ~4-5%
8. Summary: Current Thinking
- Observational data consistently show improved OS with LND, but this reflects confounding (LND patients were correctly staged and received appropriate chemotherapy)
- RCT data do NOT show a direct survival benefit from LND as a therapeutic maneuver
- The primary value of LND is staging accuracy - correctly identifying stage IIIA1 disease that would otherwise be undertreated
- Histology drives risk: HGSC and CCC warrant systematic LND; mucinous/low-grade tumors do not
- SLN biopsy may replace full LND in the future, pending prospective validation
- Para-aortic SLN mapping via infundibulopelvic ligament injection is feasible and accurate; pelvic mapping remains suboptimal
- Molecular staging (peritoneal cytology + targeted biopsy) may increasingly complement or replace nodal assessment in low-risk histologies
- Ledermann JA et al. ESGO-ESMO-ESP consensus on ovarian cancer. Ann Oncol 2024;35:248-266
- Chiyoda T et al. Lymphadenectomy for primary ovarian cancer: meta-analysis. J Gynecol Oncol 2020
- Yang C et al. Influence of lymphadenectomy in early-stage EOC: meta-analysis. BMC Womens Health 2023
- Zorzato PC et al. SLN biopsy in apparently early-stage EOC. Eur J Surg Oncol 2026
- Rey I et al. SLN biopsy diagnostic accuracy in early ovarian cancer. Int J Gynecol Cancer 2024
- Rodrigues Teixeira F et al. Impact of lymph node staging in presumed early-stage ovarian carcinoma. Eur J Obstet Gynecol 2022
- Lv B et al. Prognosis of lymphadenectomy in malignant ovarian germ cell tumor. Front Oncol 2023
- Billmire DF et al. Surgical staging for ovarian sex cord-stromal tumors. Eur J Obstet Gynecol 2025
- Chen J et al. Systematic LND may be abolished in low-grade mucinous/endometrioid EOC. Front Oncol 2021
- Kim SR et al. Lymphadenectomy in early-stage mucinous ovarian cancer. Int J Gynecol Cancer 2023
- Renz M, Friedlander M, Berek JS. Cancer of the ovary, fallopian tube, and peritoneum: 2025 update. Int J Gynaecol Obstet 2025
- Schwartz's Principles of Surgery, 11th Edition - FIGO staging and ovarian cancer surgical principles
- Campbell-Walsh Urology, 3-Vol Set - Ovarian lymphatic drainage anatomy